
Abstract
Objective:
Japanese acupuncture practice cannot easily predict the prognosis of patients with peripheral facial palsy. Electroneurography (ENoG) predicts prognosis in patients with peripheral facial palsy; however, the difference between ENoG values and degree of facial muscle contraction response (FMCR) to electroacupuncture stimulation (ES) targeting the affected facial nerve is unexplored. Therefore, an exploratory evaluation of the differences in ENoG values was conducted across the degrees of FMCR induced by ES targeting the affected facial nerve in patients with peripheral facial nerve palsy.
Methods:
In total, 90 patients with peripheral facial nerve palsy were selected who underwent acupuncture treatment at the Department of Oriental Medicine, Saitama Medical University Hospital, between January 2005 and December 2014. The FMCR degree and ENoG values were assessed through patients' medical records. The patients were divided into excellent, moderate, and noresponse groups (65, 16, and 9 patients, respectively) according to the FMCR degree. The differences in ENoG values were analyzed among the groups.
Results:
The ENoG values were 26.6% (10.4%–55.9%), 2.45% (0.35%–8.80%), and 2.00% (0.00%–5.10%) for the excellent, moderate, and no-response groups, respectively. These values significantly differed between the excellent group and the no-response (P < 0.01) and moderate (P < 0.01) groups.
Conclusion:
The ENoG values varied according to degree of FMCR induced by ES targeting the facial nerve in patients with peripheral facial nerve palsy. This might allow to predict the prognosis based on the ES-induced FMCR.
INTRODUCTION
Facial palsy occurs when the facial nerve is damaged, and presents with facial muscle paralysis. Bell's palsy is the most common peripheral facial nerve palsy, with an incidence of 20–30 per 100,000 people. 1 In addition, Ramsay Hunt syndrome, a form of peripheral facial nerve palsy, presents with herpes zoster, and symptoms originating from the vestibulocochlear nerve, 2 thus reaching an incidence of ∼5 per 100,000 people. 3 Bell's palsy has a relatively good prognosis, with ∼70% of the patients recovering to normal function 4 ; in contrast, Ramsay Hunt syndrome has a worse prognosis. 5
Electrodiagnostic tests for facial nerve palsy include electroneurography (ENoG) and nerve excitability testing (NET). ENoG was first reported by Esslen in 1973, 6 and is one of the most widespread electrodiagnostic tests. ENoG derives the compound muscle action potential (CMAP) by inducing facial muscle contractions through the transcutaneous electrical stimulation of the facial nerve exiting the stalk mastoid foramen. 7 The ENoG value is derived from the ratio of CMAP on the healthy side to that on the affected side, and is used to predict patient prognosis.8,9
Moreover, NET is an electrodiagnostic testing modality first reported by Laumans and Jongkees in 1963, and is widely used with EnoG. 10 NET involves transcutaneous electrical stimulation of the facial nerve neighboring the stylomastoid foramen to examine the contractile response of facial muscles. In a previous logistic regression analysis of the prognostic factors in patients with peripheral facial nerve palsy, the odds ratio for an abnormal NET response was 222.235.
One month after the onset of palsy, the risk of poor prognosis was 83% after combining the grade 4 or worse odds ratios on the House–Brackmann facial grading scale. 11 Coker et al. further assessed the correlation between NET and optimized lead-placement ENoG and reported a correlation coefficient of 0.849, 12 making NET as useful an electrophysiological test as ENoG.
Acupuncture is a traditional treatment in East Asia that has been utilized for Bell's palsy, 13 including electroacupuncture. 14 Electroacupuncture stimulation (ES) neighboring a peripheral nerve can induce the contraction of skeletal muscles in the area innervated by the motor nerve. Thus, ES on the facial nerve can induce contraction of facial muscles. This method is similar to NET. In clinical practice, ES is occasionally applied to acupuncture points on the affected facial nerve in patients with peripheral facial paralysis. 15 However, patients often observed that the degree of contraction of the facial muscle induced by ES varies across cases.
Most acupuncturists in Japan are engaged in acupuncture treatment at acupuncture clinics, which are different from clinics operated by physicians. Therefore, it is difficult to obtain information on ENoG values and estimate the prognosis of patients with acute peripheral facial palsy who visit acupuncture clinics. Furthermore, other facilities that do not have the equipment to perform ENoG need alternative methods to assess the prognosis of patients with peripheral facial nerve palsy.
A previous study compared the prognostic value of facial muscle contraction induced by ES and the House–Brackmann facial grading scale in patients with peripheral facial palsy. 16 However, to date, no study has examined the relationship between the facial muscle contraction response (FMCR) induced by ES targeting the facial nerve and the ENoG values.
It was hypothesized that the ENoG values would vary with the degree of FMCR induced by ES targeting the facial nerve. Thus, an exploratory and retrospective study was aimed to conduct and examine differences between the degrees of FMCR induced by ES targeting the affected facial nerve and the ENoG values.
MATERIALS AND METHODS
This retrospective study was approved by the institutional review board of the Saitama Medical University Hospital (20121.01). Data of the participants were anonymized for the analysis. Anonymization was done by assigning a personal number to each subject to exclude individual identification from the obtained data. Patients with peripheral facial palsy were recruited who underwent acupuncture at the Department of Oriental Medicine, Saitama Medical University Hospital, between January 2005 and December 2014. An opt-out format was employed, and a summary of the research was published on the website while ensuring the participants' right to refuse.
The inclusion criteria were as follows: (1) patients who visited the department within 2 weeks of the onset of symptoms for acupuncture treatment and received ENoG within a similar period and (2) those with an FMCR documented in their medical records. The exclusion criteria were as follows: (1) no physician's diagnosis documented in the medical record, (2) bilateral peripheral facial nerve palsy or a history of peripheral facial nerve palsy, (3) unknown date of onset or history, or (4) ENoG values >100%.
Electroneurography
ENoG was performed according to the methods of Esslen, 7 using Neuropack X1 MEB-2300 (NIHON KOHDEN Co, Tokyo, Japan). The stimulation current was a square wave of 0.2 ms, stimulation frequency was 1 Hz, and current amplitude was 35–40 mA. Surface electrodes for stimulation were placed adjacent to the stylomastoid foramen and the front of the tragus. The conducting electrodes were placed in the nasolabial fold, such that 1 electrode was adjacent to the ala nasi and the other electrode located in the fold.
This step was performed on the healthy and affected sides to derive the respective CMAPs, followed by calculating the ENoG value using the following formula: ENoG value = (CMAP on affected side/CMAP on the healthy side) × 100. A laboratory technician uninvolved in this study conducted the ENoG assessments at the Department of Neuro-Otology, Saitama Medical University Hospital.
Facial Muscle Contraction Response
FMCR is a contractile response of the facial muscles that can be elicited by inserting acupuncture needles in the vicinity of the affected facial nerve and by applying an electric current to the needles using an electroacupuncture device. Acupuncture needles of 40-mm length and 0.16-mm diameter (SEIRIN Corporation, Shizuoka, Japan) were inserted at 15–20 mm into GB2 and ST7 on the affected side. Subsequently, they were stimulated with a continuous 1-Hz wave using an electroacupuncture device (Ohm Pulser LFP-4500 [Zeniryoki Co, Fukuoka, Japan; asymmetric pulse wave] Pulse Generator PG-6 [Ito Co., Ltd, Saitama; asymmetric pulse wave], or Pulse Generator PG-306 [Suzukiiryoki Co, Tokyo, Japan, pulse wave]).
Since these acupuncture energization devices output bipolar waveform electricity, the polarity of the leads was not specified. The FMCR was visually confirmed and divided into excellent (overall contraction of the facial muscles), moderate (partial contraction of the facial muscles or total contraction of the facial muscles to a weak degree), or no-response (no contraction of the facial muscles) groups.
The excellent group included patients in whom all facial muscles innervated by the upper and lower trunks of the facial nerve contracted with ES to the extent that patients were not aware of pain, the moderate group included patients in whom the facial muscles innervated by either the upper or lower trunks of the facial nerve contracted with ES to the extent that patients were not aware of pain or in whom the degree of facial muscle contraction was clearly weak despite the ES to the extent that patients were aware of pain, and the no-response group included patients in whom no facial muscle contraction was observed despite the ES to the extent that patients were aware of pain. The FMCR grades were assessed by the acupuncturist who supervised the acupuncture session on the day of ENoG or the closest day.
Outcomes
The difference in ENoG values for each FMCR degree was the primary outcome. The following demographic data were also assessed: age, medical history, lowest Yanagihara score, medications, number of days from facial palsy onset to start of acupuncture, and number of days from facial palsy onset to performing ENoG. The Yanagihara score is an evaluation tool for facial muscle paralysis, based on the symmetry of the facial region at rest and 9 facial muscle movements, including maximum 4 points for each item, thus reaching a total of 40 points. 17
Statistical Analysis
A sample size calculation was not performed as the focus was on an exploratory evaluation of differences in ENoG values among different degrees of FMCR grades. Statistical analyses were performed using SPSS 28.0 (IBM Co, Armonk, NY) to assess the differences among groups. The Shapiro–Wilk test was performed to assess whether the ENoG values for all participants and for each FMCR group were normally distributed. Demographic data and ENoG values for each group were analyzed using the Fisher's exact test and the Kruskal–Wallis test.
In case of a statistically significant difference in the Kruskal–Wallis test, multiple comparisons were performed using the Dunn test to analyze the differences across groups. Continuous variables were expressed as the median and interquartile range (IQR). The statistical significance was set to P < 0.05.
RESULTS
Participant Characteristics
Initially, 553 patients were considered for the study. Of these, 463 were excluded for the following reasons: the absence of ENoG (409), visit after 2 weeks of the onset (24), ENoG value >100% (5), history of bilateral facial nerve palsy (4), no FMCR entry in the medical records (2), ENoG performed after 2 weeks of onset (6), and an unknown date of onset (13). The remaining 90 patients met the inclusion criteria and were enrolled in the study. The FMCR degree was measured in these patients and patients were divided into the excellent (65), moderate (16), and no-response (9) groups. Table 1 summarizes patients' demographic data.
Demographic and Clinical Data of All Participants
A significant difference was observed between the excellent and no-response groups using the Dunn's test (P < 0.05).
ENoG, electroneurography; FMCR, facial muscle contraction response.
In addition, the lowest Yanagihara score significantly differed among groups according to the Kruskal–Wallis test (P = 0.029). Results also significantly differed between the excellent and no-response groups according to the Dunn test (P = 0.049). Other data were similar across the groups.
ENoG Values for Each Group
Histograms of the ENoG values for all patients, A, B, and C, are presented in Supplementary Data S1. The Shapiro–Wilk test, performed to verify the normality of ENoG values, was P < 0.05. The normality of the ENoG values for each group was similarly assessed with P < 0.001 for all groups. Figure 1 depicts ENoG values for each FMCR grading groups. The ENoG values for the excellent, moderate, and no-response groups were 26.6% (10.4%–55.9%), 2.45% (0.35%–8.80%), and 2.00% (0.00%–5.10%), respectively. The values significantly differed between the excellent and the no-response (P < 0.01) and moderate (P < 0.01) groups (Fig. 1).
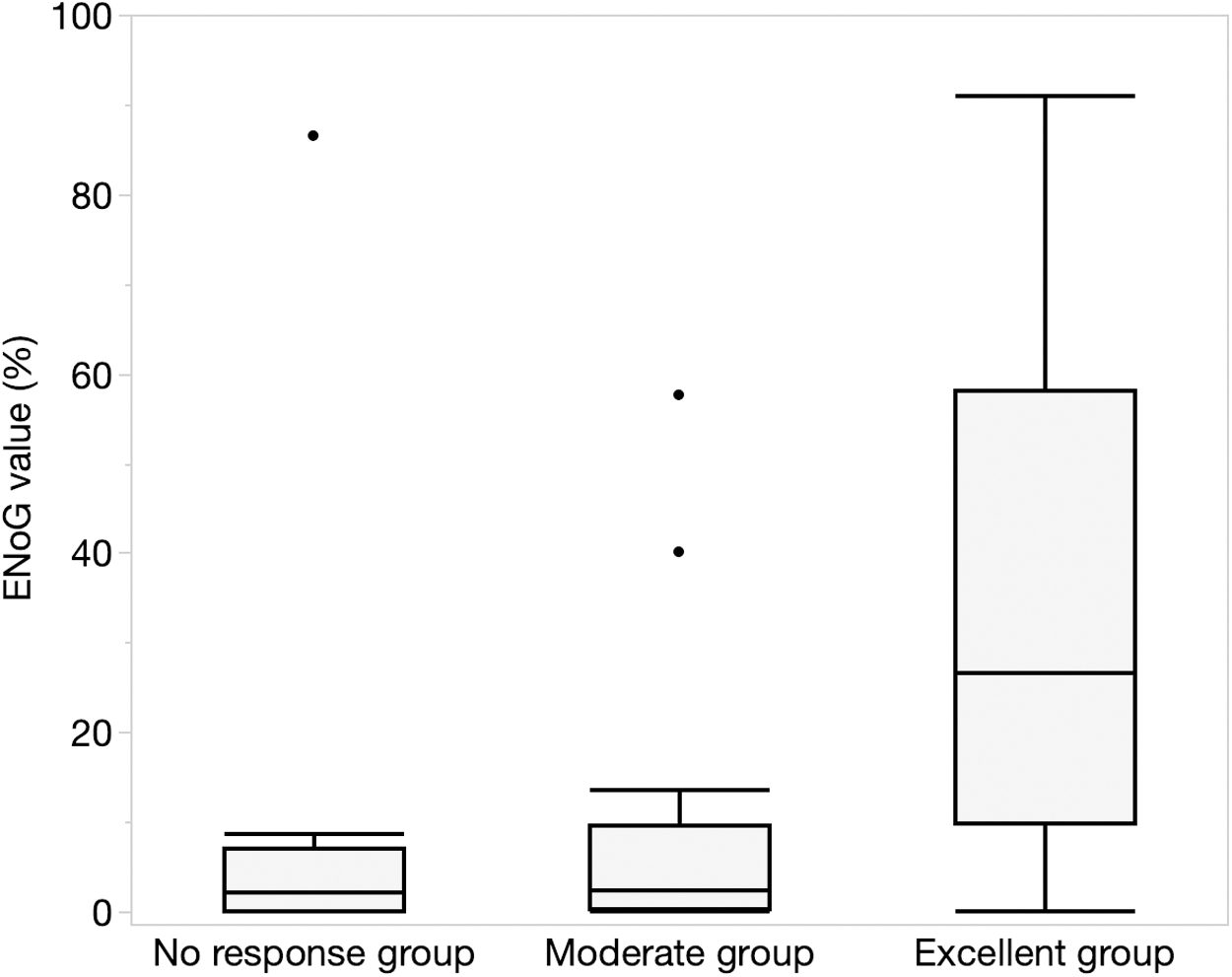
ENoG values calculated for each FMCR group. An ∼10-fold difference appears between the excellent and remaining groups. The Dunn's test reveals that this difference is statistically significant. Outliers indicate values more than ±1.5 times away from the IQR. ENoG, electroneurography; FMCR, facial muscle contraction response; IQR, interquartile range.
DISCUSSION
This novel exploratory study reported the differences in the ENoG values for varied degrees of FMCR obtained using ES at acupoints adjacent to the facial nerve. The findings revealed a significant difference in ENoG values between the excellent and moderate and no-response groups, thereby suggesting possible variations in the severity of facial nerve palsy among the groups. In addition, there was no significant difference in the ENoG values between the moderate and no-response groups; thus, the severity of facial nerve palsy may be similar in these groups.
ENoG was first reported by Esslen in 1973, and it is one of the most widely used electrodiagnostic tests 6 to assess the prognosis of patients with peripheral facial nerve palsy. The nonrecovery rate increases with the degree of facial nerve degeneration. 18 The presence of >85% neurodegeneration assessed using ENoG predicts nonrecovery, with a sensitivity of 71.4% and specificity of 77.8%. 19 On comparing the aberrant regeneration ratio of cases with ENoG values ranging from 10% to 20% and <10%, lower ENoG values implied a higher stray regeneration rate. 9
Furthermore, an ENoG value of 46.5% reportedly predicts synkinesis with <85% inferior eye opening, with a sensitivity of 97.1% and specificity of 77.5%. 20 Thus, ENoG is a useful electrodiagnostic test for prognosis, and physicians should examine ENoG results while clinically treating peripheral facial nerve palsy.
However, acupuncturists working in acupuncture clinics across Japan are not permitted to perform electrodiagnostic tests. This necessitates the identification of a process to use acupuncture needles that is available to acupuncturists. The FMCR measured in this study was derived from acupoints on the facial nerve track. The FMCR and NET are mechanistically similar; therefore, the FMCR induced by ES may be weakened in case of a severely affected facial nerve, causing differences in the ENoG values based on the FMCR degree.
There are several reports on the use of acupuncture needles to predict the prognosis of patients with peripheral facial nerve palsy. Kobayashi assessed the difference between acupuncture needle electrodes and surface electrodes as the stimulation electrodes for NET. The temporal change in the electromyography pattern obtained by the contractile response of facial muscles differed between the groups. 21 In this report, the threshold of NETs was lower for acupuncture needle electrodes than for surface electrodes.
Thus, FMCR can be performed with a low threshold, and the burden on the patient is relatively low. Huang et al. compared the prognosis of acupuncture for patients with peripheral facial nerve palsy using the House–Brackmann facial grading scale and electrical response grading based on ES to the affected facial muscles. Both groups displayed low consistency, and the electrical response grading was more strongly correlated with the therapeutic effect of acupuncture. 16 This study differed from this report on ES. The method was novel as the acupuncture needles were inserted near the facial nerve, thereby reducing the number of puncture points to 2 and lowering the invasiveness for the patient.
The findings revealed a significant difference in the lowest Yanagihara score between the excellent and no-response groups. Moreover, a difference in the ENoG values between the excellent and no-response groups was observed. The degree of paralysis was higher in the no-response group than in the excellent group, which may have caused the difference in the lowest Yanagihara score between these groups. Thus, practitioners may use the FMCR induced by ES targeting the affected facial nerve to infer the ENoG values.
Limitations
An advantage of this study was that it employed ES, which is considered less burdensome to patients, thereby demonstrating that ENoG values differed depending on the FMCR degree. However, there were some limitations regarding the interpretation of the results.
First, there was potential misclassification of the FMCR degree. Particularly, the excellent group displayed large IQR of ENoG values. The FMCR was assessed visually and may be misclassified as per variations in the evaluation among the examiners. In addition, ST7 is located on the masseter muscle and ES to ST7 may have induced contraction of the masseter muscle. This in turn may have been erroneously identified as contraction of the facial muscles, resulting in cases that should have been included in the moderate or no-response group to be misclassified into the excellent group.
The second limitation was the variability of the ENoG values. Esslen reported 3% left–right difference in the ENoG values in healthy individuals. 7 In contrast, ENoG levels may fluctuate even in healthy individuals. 22 This phenomenon may have influenced the results.
The third limitation was related to information bias. A retrospective study was performed. Performing ENoG before ES could have enabled browsing the ENoG values in the medical records. The FMCR degree was possibly overestimated or underestimated based on this information, thus explaining the outliers in this study.
The fourth limitation was the failure to calculate the expected sample size. Additionally, the no-response group had fewer patients. Therefore, the results must be cautiously interpreted.
Finally, this study was based on a retrospective and cross-sectional design, and the treatment course of the participants was not investigated. Therefore, the FMCR cannot be used for prognostic estimations based on the results, thereby necessitating future prospective studies.
CONCLUSION
ES-induced FMCR targeting of the affected facial nerve in patients with peripheral facial paralysis was confirmed. Patients were grouped according to their FMCR degree, and the differences in the ENoG values were assessed across groups. The ENoG values differed according to the degree of FMCR. Thus, the FMCR induced by ES targeting the facial nerve may be used to infer the ENoG values.
Footnotes
ACKNOWLEDGMENTS
The authors thank Ai Kouchi and Shintaro Ibata, affiliated with the Department of Oriental Medicine, Saitama Medical University, for their help in proofreading this article. They also thank Tomokazu Kikuchi, affiliated with the Japan School of Acupuncture and Moxibustion Therapy, for providing assistance in planning the study.
AUTHORs' CONTRIBUTIONS
G.H. designed this study, obtained and analyzed the data, and wrote the first draft. A.I. and S.Y. proofread the study design prepared by G.H. and contributed to the critical interpretation of the obtained data and the proofreading of the article. All authors read and approved the final version of the article accepted for publication.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.