
Abstract
Background:
Clinical studies have shown that electroacupuncture (EA) has therapeutic and modulatory effects on managing heart failure (HF) risk factors.
Objective:
This study aimed to determine the impact of combination drugs and EA on chronic HF patients with reduced ejection fraction (HFrEF) to maintain a stable heart rate (HR) and mean arterial pressure (MAP).
Materials and Methods:
This single-blind clinical randomized controlled trial included 42 patients with chronic HFrEF. The patients were divided into 3 groups: patients taking drugs and EA, patients taking drugs and sham EA (sham acupuncture [SA]), and patients taking drugs without EA. All patients underwent 16 sessions of therapy for 8 weeks.
Results:
There was a significant difference in the average MAP based on therapy duration in the drugs + EA group, whereas there was no significant difference between drugs + SA and drugs without EA groups. There was a substantial difference between the average MAP in the drugs + EA group at the beginning of therapy compared with that at midtherapy (P < 0.05) and at the beginning of treatment and at the end of therapy (P < 0.05). There was no significant difference in the mean HR between the groups. Clinically, after 16 treatment sessions, patients receiving combined drugs and EA treatment presented with stable MAP and HR.
Conclusions:
Drugs combined with EA maintained the stability of MAP and HR in patients with chronic HFrEF.
INTRODUCTION
Heart failure (HF) is a disease caused by a structural or functional problem in the heart that reduces the vital ability of the ventricles to pump blood, with high morbidity and mortality rates.1–3 According to the New York Heart Association's (NYHA) guidelines, HF can be divided into several categories based on symptoms that affect functional ability. 4 HF is characterized by excessive compensatory neurohormonal activity, including the renin–angiotensin–aldosterone system activation and sympathetic activity.5,6
The body responds to these conditions by performing a series of compensatory actions, including hemodynamics (increase in blood flow, stimulation of vasoconstriction, stimulation of heart rate (HR), and contractility to maintain perfusion pressure in essential organs), an inflammatory response (body organs react as though an external agent is attacking them; inflammatory cytokines and reactive oxygen species play a crucial role in this response), a ventricular hypertrophy response, and mean arterial pressure (MAP) regulation.5,7
Lower cardiac output causes a decrease in MAP, and worse tissue perfusion eventually exacerbates HF.8,9 The sympathetic nervous system (SNS) stimulates and releases catecholamines (norepinephrine and epinephrine), which directly increase HR and contractility of peripheral blood vessels (vasoconstriction) while increasing stroke volume and total peripheral resistance. Long-term SNS overstimulation causes decreased ejection fraction (EF).10–12 The HR must be significantly decreased to reverse poor left ventricular function.12–14
Previous studies have shown that electroacupuncture (EA) significantly reduces sympathetic activity and inhibits cardiovascular sympathetic afferent reflex reactions induced by chemical, mechanical, and electrical stimuli.3,8 A systematic review of clinical trials on the effects of acupuncture on HF by Lee et al. reported that acupuncture increases cardiac function capacity, hemodynamic parameters, and HR variability time parameters. 15
METHODS
Study Design
This study was a single-blind hospital-based randomized controlled trial (RCT). Data were collected from March 2019 to July 2019.
Participants and Recruitments
The participants were recruited from the Heart Failure Clinic, Universitas Sebelas Maret Teaching Hospital, Central Java, Indonesia. Patients were screened for eligibility using the following criteria: (1) diagnosed with HF (NYHA class II–III with reduced EF <40%) by a cardiologist; (2) aged >21 years; (3) a prescription for standard HF drugs that are balanced and optimal according to European Society Cardiology (ESC) guideline 201613 standards by a cardiologist consisting of β-blockers (Bisoprolol 2.5 mg once daily up titrated until the maximum tolerated evidence-based dose), Angiotensin-converting enzyme (ACE) inhibitors (ramipril/lisinopril tablets 10 mg once daily), aldosterone antagonists (spironolactone tablets 25 mg once daily), and diuretics (furosemide 40 mg in patients with signs and symptoms of congestion); and (4) willing to participate in the study. Patients who had recently undergone acupuncture therapy and had a history of heavy bleeding, malignant arrhythmia, were pregnant, had severe skin lesions, a fever >38°C, infection, swelling, or metal implants were excluded.
We calculated the sample size adequacy using the test of difference in 2 independent proportions, with a dropout calculation of 10%. This calculation yielded a required total sample size of 39 according to an α level of 0.05, a conventional medium effect size of 0.5, and a power of β = 0.80 for the F-test. Therefore, the number of participants in this study was considered appropriate. 16 The participants were allocated to 3 groups: Group A (drugs + EA), Group B (drugs + sham acupuncture), and Group C (drugs without EA). The clinical coordinator enrolled the participants. Through use of a computer, patients were coded and randomly assigned to 1 of the 3 sets of treatment. Cardiologist and assessors who analyzed the outcomes (MAP and HR) were blinded to the EA treatment.
Intervention
All groups received routine monitoring and drug titration from the cardiologist based on ESC guidelines 2016 for HF. 13 EA therapy in the form of Western medical acupuncture was prescribed for Group A. Disposable sterile stainless steel acupuncture needles with the dimension of 0.25 × 25 mm were inserted bilaterally, perpendicularly into 1 of 2 sets of acupoints, including PC5 Jianshi—PC6 Neiguan (on the palmar side of both arms, ∼4 and 6 cm [2 and 3 cun] above the crease of the wrist, respectively, between the tendons of the long palmar muscle and radial flexor muscle of the wrist, overlying the median nerve), ST36 Zusanli (on the anterolateral side of the leg, ∼2 cm [1 cun] lateral to the anterior crest of the tibia, overlying the deep peroneal nerve), and paired with SP6 Sanyinjiao (on the tibial aspect of the leg, posterior to the medial border of the tibia 6 cm [3 cun] superior to the prominence of the medial malleolus). 17
For safety, pairs of ipsilateral acupoints on each side were stimulated during EA so that current flowed between the 2 adjacent electrodes rather than through the body to the contralateral extremity. 18 These 2 sets of acupoints were stimulated bilaterally (8 needles for each patient). Needles were inserted and stimulated for 30 minutes using currents at low intensity and low frequency (2 mA and 2–4 Hz) in continuous waves by a Hwato-type SDZ-V digital electrostimulator (from China).16,18–20 Group B gets acupuncture needles at the same acupoints, but the needles are stuck in the plaster that cannot penetrate the skin, and the electrostimulator is inactive. Group C gets drugs without EA.
The reasons for choosing the PC5–PC6 point include that together they inhibit the cardiovascular sympathoexcitatory pressor reflex, which, through activation of μ and δ receptors, will inhibit sympathetic activity to improve cardiac function and cardiac remodeling, as well as modulate cardiac autonomic nervous imbalances by increasing the vagal component of the heart in HR variability.3,21 In principle, acupuncture works to balance the body's homeostasis so that the ST36 and SP6 acupoints, mediated by opioids (β-endorphins and enkephalins), will reduce inflammation and reduce blood pressure that is too high. As well as, if blood pressure is too low, ST36 can activate a decrease in the SNS and increase MAP.8,22
Protocols
Forty-seven patients entered into this study were treated twice a week for a total of 16 sessions. Patients in Groups A and B were treated in the supine position. In all groups, data were collected at baseline (1st session), middle (8th session), and at end of therapy (16th session). Cuff BP and HR were recorded before and after the 20 minutes of treatment. Group C came to the hospital to have the same measurements taken, to match the follow-up method with the other groups. After treatment, 5 patients declined to continue with the follow-up for >2 sessions despite encouragement. Thus, 42 patients received full-session therapy (Fig. 1).
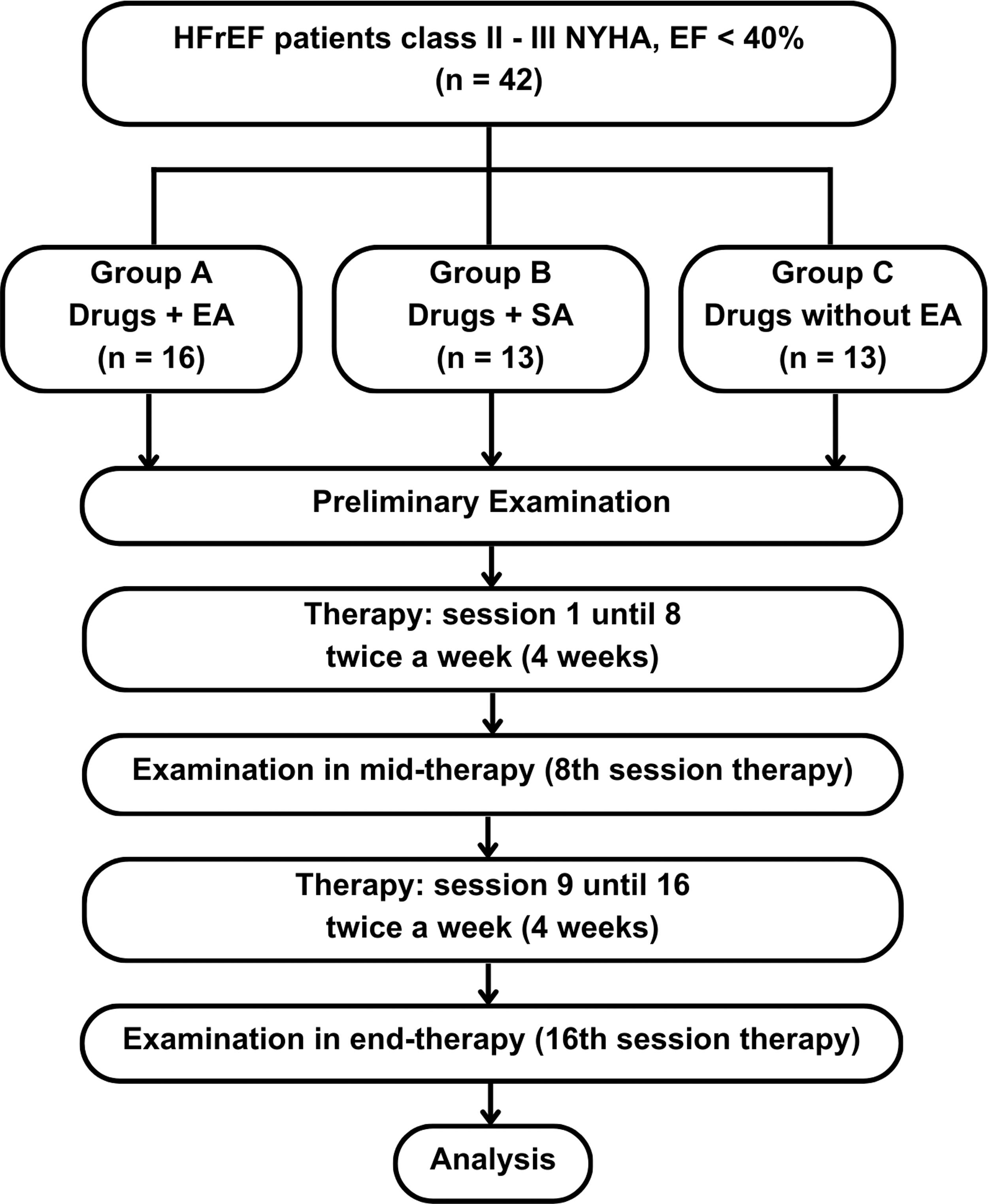
Research flow scheme. EA, electroacupuncture; HFrEF, HF patients with reduced ejection fraction; NYHA, New York Heart Association's; SA, sham acupuncture.
Statistical Analyses
Descriptive statistics and one-way analysis of variance (ANOVA) were used to describe univariable data. The study's objectives were to determine the effectiveness of drugs combined with EA by comparing the HR and MAP of both groups at baseline and follow-up using repeated-measures ANOVA as a statistical analysis.
Ethical Consideration
This study was approved by the health research ethics committee of the University of Indonesia and the Cipto Mangunkusumo Hospital (No. KET-245/UN2.F1/ETIK/PPM.00.02/2019).
RESULTS
Baseline Characteristics
Forty-seven patients were enrolled, and 42 patients completed the study, with a response rate of 89.4%. Notably, there were 16 patients in Group A, 13 in Group B, and 13 in Group C. The baseline characteristics of the respondents presented in Table 1 show no significant differences in age and gender between treatment groups. Likewise, for initial data, examination of patients' left ventricular ejection fraction, HR, and MAP at the start of therapy did not show significant differences in the 3 groups.
Homogeneity of Demographic and Clinical Characteristics Between Groups (N = 42)
Kruskal–Wallis test.
One-way analysis of variance test.
bpm, beat per minute; EA, electroacupuncture; HR, heart rate; LVEF, left ventricular ejection fraction; MAP, mean arterial pressure; SA, sham acupuncture.
Effect of Combined Drugs and EA on Maintenance Stability of MAP in Chronic HF Patients with Reduced Ejection Fraction Patients
The ANOVA and Freidman test showed the comparisons between beginning and end measurements in each treatment group. There was a significant difference in average MAP over time in Group A but no significant difference in average MAP over time in Groups B and C (Table 2).
Results of Repeated Analysis of Variance and Friedman Test in Each Treatment Group for Mean Arterial Pressure Measurement
Greenhouse–Geisser (tests of within-subject's effects).
Friedman test.
EA, electroacupuncture; SA, sham acupuncture.
In Group A, there was a significant difference in the mean MAP between the beginning and middle of therapy (P < 0.05), as well as between the beginning and end of treatment (P < 0.05). However, there was no discernible difference in average MAP measurements between the middle and end of the course of treatment. There were no noticeable differences in the mean MAP measurements at the start, middle, or end of therapy between the groups (Table 3).
Pairwise Comparison Analysis Results Between Mean Arterial Pressure Measurement Time Intervals
Repeated analysis of variance test.
Paired t-test.
Wilcoxon test.
EA, electroacupuncture; MAP, mean arterial pressure; SA, sham acupuncture.
Clinically, individuals receiving a combination of drugs and EA displayed stable MAP variability after 16 treatment sessions (Fig. 2).
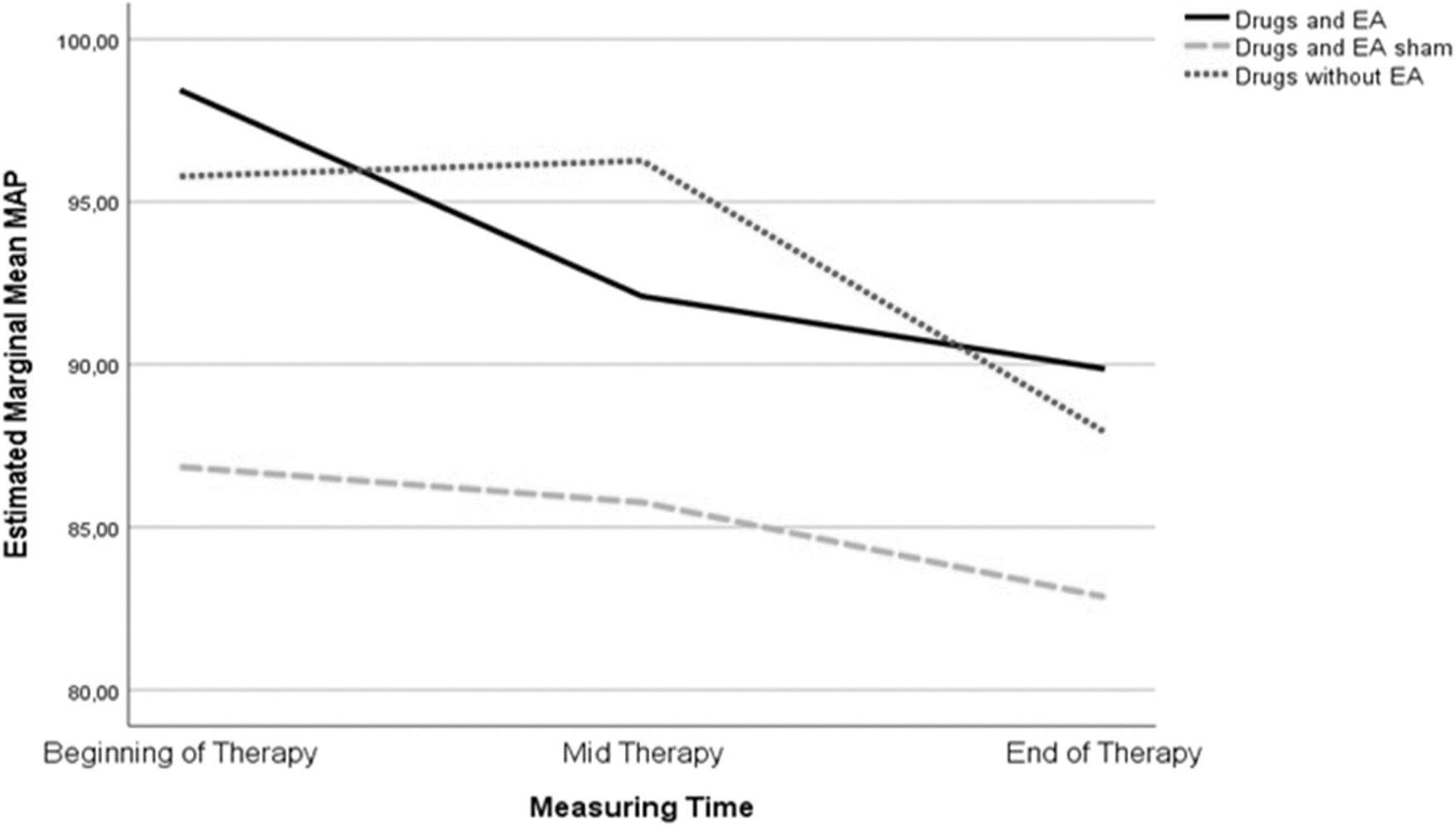
Trends for MAP measurement in the 3 treatment groups during follow-up. EA, electroacupuncture; MAP, mean arterial pressure.
The average MAP measurement results of the 3 treatment groups were not significantly different at the beginning, midtherapy, or end of therapy. At the beginning, middle, and end of therapy, there were no appreciable differences between the average MAP measurements of the 3 treatment groups (P > 0.05), and there was no discernible change in the mean MAP in any of the groups (P > 0.05) (Table 4).
Results of Intertreatment Group and Between the 3 Treatment Groups Analysis for Mean Arterial Pressure Measurement
One-way analysis of variance test.
Mann–Whitney test.
Independent t-test.
Kruskal–Wallis test.
EA, electroacupuncture; SA, sham acupuncture.
Effect of Combined Drugs and EA on Maintenance Stability of MAP
After 16 treatment sessions, Group A presented HR stability (Fig. 3).
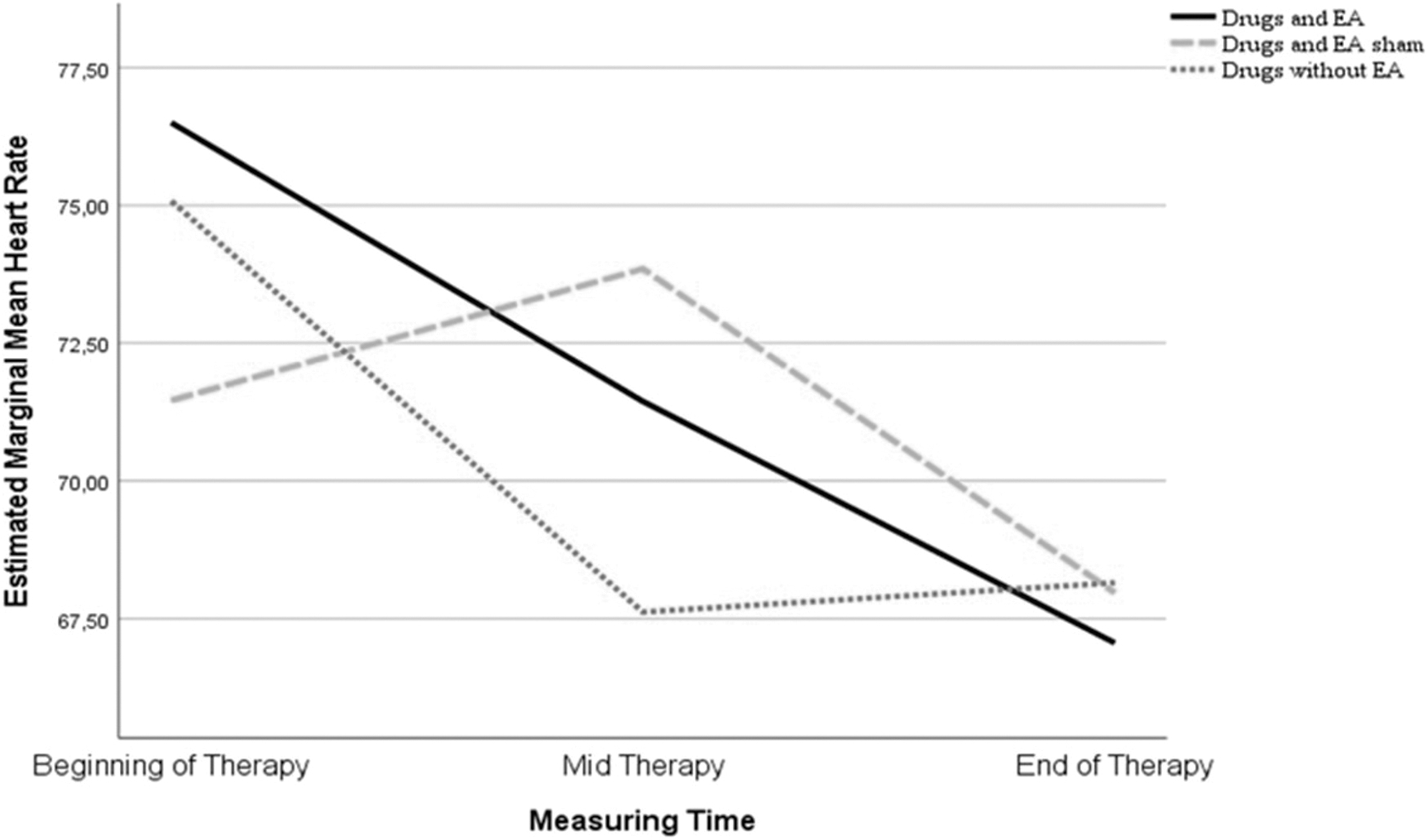
Trends in HR reduction during follow-up among the study groups. EA, electroacupuncture; HR, heart rate.
There was no significant difference in the average HR in all groups (P > 0.05) (Table 5).
Pairwise Comparison Analysis Results Between Heart Rate Measurement Time Intervals
Repeated analysis of variance test.
Paired t-test.
Wilcoxon test.
EA, electroacupuncture; SA, sham acupuncture.
Analysis of differences in the effect of therapy between the 3 groups is presented in Table 6. The average HR measurement results for the 3 treatment groups did not differ significantly. There was no significant difference in the mean HR between the groups at the beginning, middle, or future stages of treatment.
Results of One-Way Analysis of Variance Test Analysis and Kruskal–Wallis Test Between the Treatment Groups for Measuring Heart Rate
Analysis of variance test.
Kruskal–Wallis test.
DISCUSSION
This study evaluated MAP and HR in HF patients with reduced ejection fraction (HFrEF) who received a combination of drugs and EA. Acupoints were chosen based on a previous study that showed that these acupoints successfully preserved and enhanced MAP and HR stability. The neurohormonal compensatory HF mechanisms and the EA modality can considerably lower sympathetic activity and suppress cardiovascular sympathetic reflex responses. Low-frequency EA provides a tonifying effect in chronic cases and stimulates cell repair. 23
Acupuncture and HR stability have been linked in previous studies. According to Wang et al., acupuncture increases vagal activity and decreases sympathetic activity in healthy humans. 24 The results of this study indicated that there was no change in HR in any of the treatment groups. The average HR in the measurement results of the 3-time intervals in this study was within the normal limits (60–100 beats/minute). The average HR during the 3 times of data collection did not differ significantly between all groups.
At the beginning, middle, or end of the therapy, there were no appreciable differences between the average HR measurement results. There was no discernible difference in the average HR between the groups. The findings of this study are consistent with those of Lima et al., 8 Middlekauff et al., 25 and Kristen et al. 26 that found no discernible difference in mean HR between EA and control groups.
This study showed a significant difference in average MAP over time in Group A. In Group A, there was a significant difference between the initial average MAP measurement of therapy and MAP at the 8th session of therapy, and a significant difference between the average initial MAP measurement and MAP at the 16th session of therapy. However, the average MAP measurement results of the 3 groups did not differ significantly at the beginning, middle, or end of the therapy. Previous studies have also shown that EA provides benefits for MAP repair. Ma et al. 3 found that rats with HF treated with EA had significantly improved MAP compared with the sham rat group.
The EA-stimulating effect is comparable with that of the selective B-1 blocker mesoprolol on heart function and structure in experimental animals. 3 Likewise, the study by Michikami et al., 27 who used EA at the ST36 point, showed a decrease in arterial pressure, which indicates the mechanism of action of acupuncture on arterial baroreflexes, which means it is related to MAP. Lima et al. 8 also looked at the long-term effects of EA at the ST36 point on the function of baroreceptors in animals with HF. Compared with the control group, the MAP went up in the EA group.
Acupuncture at acupoints PC6 Neiguan and PC5 Jianshi has been shown to improve cardiac function, prevent regional myocardial ischemia caused by an increase in cardiac oxygen demand caused by sympathetic innervation (increased oxidative phosphorylation in the myocardium), and stimulate the median nerve. 26 Acupuncture at acupoint ST36 Zusanli has been shown to induce SNS depression, encourage higher MAP, and increase cardiac function.14,28
Mediated by opioids (significant effect), such as endorphins, EA acts on the sympathetic system and the renin–aldosterone system to lower blood pressure, together with PC6 Neiguan, to reduce and prevent arrhythmias (but is insufficient for severe arrhythmias), as well as for combined immunity with SP6 Sanyinjiao, and catecholamine leuenkephalin, which are similar to noradrenaline.29,30 By considerably increasing the protein and messenger RNA levels of endothelial nitric oxide synthase and lowering the proinflammatory cytokine IL-6, ST36 Zusanli increased blood flow.29,31,32 The SP6 Sanyinjiao point undergoes acupuncture to increase IL-10 concentration,10,30 which decreases pain and inflammation while lowering blood pressure, and ST36 Zusanli.8,33
Understanding how clinical scientific investigations were conducted and how acupuncture established its effects on particular medical disorders is essential for comprehending the mechanisms of acupuncture. The rostral Ventro Lateral Medulla (rVLM) is a crucial brainstem area.29,31 Studies in both humans and experimental animals have shown that EA has a prolonged duration of action. Although each acupuncture episode lasts only a few minutes (15–45 minutes), the long-term effects of EA are clinically significant.
To obtain a sufficient clinical response, patients can be treated once or twice a week if there is a persistent impact on cardiovascular function. Since it processes many afferent inputs, such as those from somatic and visceral systems that are activated during EA and excitatory reflexes linked to gastric stimulation (stomach acupoint), the rVLM is likely a center that supports this long response. EA with selected acupuncture points is expected to improve cardiac function and remodeling by activating opioid receptors. Activation of this receptor increases cardiac vagal components, increases MAP, decreases the proinflammatory cytokine IL-6, and increases IL-10 concentration, which is expected to reduce cardiac fibrosis.29,34
However, clinical research on EA using chronic HF-afflicted human subjects is relatively uncommon. Therefore, it is used as an adjuvant treatment with prescription medications and other medical therapies provided by cardiologists for patient safety factors. During the study, no side effects, such as infection or hematoma, were found in the area of the acupuncture points. The weakness of this study is that the length of therapy sessions—16 sessions for 8 weeks—significantly affects the regularity of patient arrivals for therapy and the risk of dropping out.
Even though we have followed the ESC guidelines in administering pharmacology by a cardiologist, the pharmacologic intervention should be addressed as a confounding issue. Although β-blockers can limit changes in both HR and MAP, ACE inhibitors and diuretics can limit changes in MAP, potentially blocking acupuncture effects. Further research should focus on controlling for comorbid factors that can potentially be confounding factors.
CONCLUSION
This randomized controlled single-blind trial suggests that EA may keep MAP and HR stability in people with HFrEF when given in addition to standard HF treatment that is working well. More research needs to be done on the positive effects of EA in HFrEF, especially its effects on the balance of neurohormones and the production of inflammatory cytokines.
Footnotes
AUTHORs' CONTRIBUTIONS
D.S.S. contributed to conceptualization (lead), writing–original draft (equal), and review and editing (equal). A.E.P. was involved in methodology and analysis (lead), writing–original draft (lead), and writing–review and editing (equal). H.A. was in charge of conceptualization (equal), writing–original draft (supporting), and review and editing (equal).
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.
CME Quiz Questions
Publication date: December 13, 2023
Expiration date: December 31, 2026
None of the authors, editors, or reviewers of this educational activity, have relevant financial relationship(s) with ineligible companies to disclose.
Articles in Medical Acupuncture will focus on acupuncture research through controlled studies (comparative effectiveness or randomized trials); provide systematic reviews and meta-analysis of existing systematic reviews of acupuncture research and provide basic education on how to perform various types and styles of acupuncture. Participants in this journal-based CME activity should be able to demonstrate increased understanding of the material specific to the article featured and be able to apply relevant information to clinical practice.
You may earn CME credit by reading the CME-designated article in this issue of Medical Acupuncture and taking the quiz online. A score of 75% is required to receive CME credit. To complete the CME quiz online, go to ![]() – AAMA members will need to login to their member account. Non-members have opportunity to participate for small fee.
– AAMA members will need to login to their member account. Non-members have opportunity to participate for small fee.