
Abstract
Background:
Failure to thrive (FTT) is a challenging childhood condition that may lead to developmental delays and requires immediate therapeutic strategies. Children are diagnosed with FTT when their weight or rate of weight gain is significantly below that of other children of similar age and sex. A Pub Med literature search revealed no published acupuncture treatments for failure to thrive or faltering growth.
Case:
A 2 year, 4 month-old female was presented with FTT and a history of multiple severe congenital medical conditions. Western medical treatment with optimization of tube feeds achieved weight scores in the third-to-fifth percentile range. Acupuncture points were electrically stimulated for the child once monthly for 30 seconds with a Pointer Plus™ at each of 12 traditional Chinese/Shu Mu points and at several auricular points: Appetite, Stomach, Small Intestine, and Large Intestine bilateral.
Results:
The patient gained weight during the treatment, increasing monthly as shown on fully naked weight measurements to the 25th percentile, 28th percentile, 32nd percentile, 40th percentile, 46th percentile, 61st percentile, and 65th percentile. Her treatment was spaced to every 2.5 months after the 46th percentile measurement, and her weight started to level off when it reached the 61st percentile.
Conclusions:
In this particular case, electroacupuncture (EA) stimulation may have facilitated a weight gain in this female child. EA (nonneedle) research should be explored for FTT.
INTRODUCTION
Failure to thrive (FTT) or faltering growth is elusive to define exactly, and variability exists in the definitions. However, FTT refers to a slower childhood growth rate than would be expected for a patient's age and sex. 1 FTT usually affects children having problems with eating, congenital anomalies, prematurity, surgeries, gastrointestinal (GI) conditions, illnesses, stress, or psychiatric problems; in addition, parents with a paucity of financial resources may affect the development of their children. 2 Additionally, the Johns Hopkins Medicine organization adds to the etiology of FTT: neglect; chromosome abnormalities; major organ system defects; endocrine–growth-hormone deficiency; central nervous–system issues causing feeding difficulties; heart or lung pathologies; anemia; malabsorption; cerebral palsy; long-term infections; metabolic disorders; and low birth weight. 3 Causes of growth faltering ultimately comes down to inadequate caloric intake, inadequate GI absorption, or excessive energy expenditure. 4
There is not a definite consensus on the diagnostic criteria for FTT, but it is often diagnosed when a child is below the third or fifth weight percentile, under 80% of the ideal age weight, or having weight loss crossing 2 major percentile lines on the standard growth chart. 5 In the Merck Manual, it is noted that most children achieve stable weight, defined as above the third percentile. 6 The affected age is usually in the 1–2 year-old range, but FTT may occur at any age. 5 There is a variant of normal growth wherein healthy infants may fall below birth percentiles sometime in the first year of life then achieve their own unique normal percentile for their growth trajectories. 7 In low-income countries, poverty and poor nutrition contribute to a 26% prevalence worldwide for the under-5 age group, while high-income countries reportedly have a prevalence between 1% and 10% of children under 2 years of age. 7
A full history on a patient with FTT should focus on social/nutritional issues, genetic family tendencies, medical conditions, and stressors. 2 A physical examination should assess for genetic dysmorphology, nutritional deficiency, and major system abnormalities of the heart, lungs, liver, intestinal, or neurologic systems. 2 Recommended laboratory tests, if indicated by the clinical picture, include blood count, a metabolic panel, urinalysis, thyroid functions, celiac-disease testing, iron studies, sedimentation rate, cystic-fibrosis testing, human immunodeficiency virus testing, an electrocardiogram, and food-allergy testing.2,8
Western medical treatment may simply be parent education, but, often, hospitalization is needed to coordinate a full biopsychosocial plan. Treatment goals include a proper growth velocity along the growth chart to prevent long-term growth and cognitive delays. 9 Medications are not recommended for most patients, but improvements in caloric intake and appetite might include megestrol or cyproheptadine.10,11 According to information on the Learn Pediatric website, normal weight gain up to 3 years of age is 26–31 g per day. 12 Catch-up growth may take 2 weeks to become evident, even at 150% of the recommended daily caloric intake. It often takes 6–12 months to achieve proper weight fully. 13 Treatment response is achieved when weight and height above the tenth percentile are sustained during 2 consecutive months. For FTT resolution, growth-chart gains need to be consistent for 49 months. 14
FTT sequelae may persist for several years. Follow up-of infants with FTT in London when they reached age 6 showed that the children still had decreased body mass indices, heights, and weights. 15
CASE
History
A 2-year, 4-month-old female was presented with deficient weight gain despite consistent nutritional optimization via tube feeds. Her past medical history was significant for congenital esophageal atresia, a tracheoesophageal fistula, an atrial-septal defect, and hypothyroid and pulmonary hypertension. Her past surgical history was significant for a tracheostomy for subglottic stenosis, gastrojejunal-tube placement (she was tube feed–dependent for her entire life), esophageal-atresia repair, tracheoesophageal fistula repair, atrial-septal defect repair, and esophagus–pulmonary fistula repair. She had been given levothyroxine, aspirin, omeprazole, and probiotics. No oral feedings had been successful since her birth.
Pretreatment Weight and Height
Weight data were not available prior to 2 years of age. Three months prior to her initial clinical examination, her recorded weight (fully clothed including a diaper) was between the fifth and seventh percentiles. Weighing this child clothed and unclothed in the clinic showed a difference of 0.33 lbs. with her shoes off (the shoes were not weighed). Thus, there appeared to be a 0.33-lb. overcalculation for all the pretreatment readings, including on the date of the first treatment. Taking this into account, 2 pretreatment weights were somewhere between the third and fifth percentiles. This was right at the FTT threshold. Pretreatment heights went progressively from the eleventh to the third percentile.
Physical Examination
A clinical examination revealed that this patient was an active, neurologically intact, nondysmorphic, thin 2-year-old female. Her upper body posture tilted slightly to the right. Despite little verbalization, she initiated short phrases with proper operation of the tracheostomy tube. Her jejunostomy (j-tube) tube was in place and functioning. There was a ∼3-cm, well-healed surgical scar under her posterior right axilla. There were no other apparent deficits. No pulse or tongue diagnosis was performed due to the patient's age and intolerance to these maneuvers.
Literature Searches About FTT and Acupuncture
A literature search on FTT and acupuncture was performed in the Cochrane Trials Library from June 30, 2023, for
Electroacupuncture
Treatment was in the patient's primary care pediatric clinic by a single medical acupuncturist who was enlisted by the parent who had been treated in the acupuncture clinic. This parent inquired because the child continued to fall off growth targets despite apparent optimal allopathic treatment. Points were chosen to affect primarily the GI system. In a sitting position, the patient tolerated comfortable 30-second, 10-Hz stimulation with a Pointer PlusTM once per month on body and auricular points. The Pointer Plus was set at a fixed 10 Hz and at an intensity that is adjustable according to product specifications. 16 A monthly interval between treatments was chosen due to the patient's extensive medical-intervention history, which caused her to have a fear of medical procedures, and to allow appropriate time to detect treatment effects best on the growth chart. Nonneedle stimulation was chosen to minimize invasiveness and to increase patient comfort with the procedure.
Body acupuncture points chosen were: Shu Mu points for the Stomach at CV-12 and BL-21; Small Intestine at CV-4 and BL-27; and Large Intestine at ST-25, BL-25, and CV-6.
Auricular acupuncture points chosen were: Stomach; Small Intestine; Large Intestine; and Appetite points bilateral.
For scar treatment, the right axilla surgical scar that caused this patient to chronically lean to the right was stimulated along its length with the Pointer Plus.
Nonacupuncture Treatment
The only nonacupuncture medical visit or treatment during the 8 acupuncture treatment months was a laser laryngeal treatment for postsurgical adhesions a few days before her third acupuncture treatment. Erythromycin was prescribed 4.25 months after the start of acupuncture therapy. This was added by the pediatrics department to potentially assist with gastric motility. Tube feeds were with Nourish® with water at 1250 mL per day, and that had been changed to Nourish with milk when she reached age 2. The milk added ∼200 calories per day
RESULTS
The child tolerated these treatments well, looking at the Pointer Plus, then otherwise being distracted by the electronic entertainment.
Weight and Height
Pre-treatment, the child's 3 documented weights were between the third and fifth percentile. (Fig 1). The patient gained weight during the treatment, increasing monthly as shown on fully naked weight measurements to the 25th percentile, 28th percentile, 32nd percentile, 40th percentile, 46th percentile, 61st percentile, and 65th percentile. Her treatment was spaced to every 2.5 months after the 46th percentile measurement, and her weight started to level off when it reached the 61st percentile.
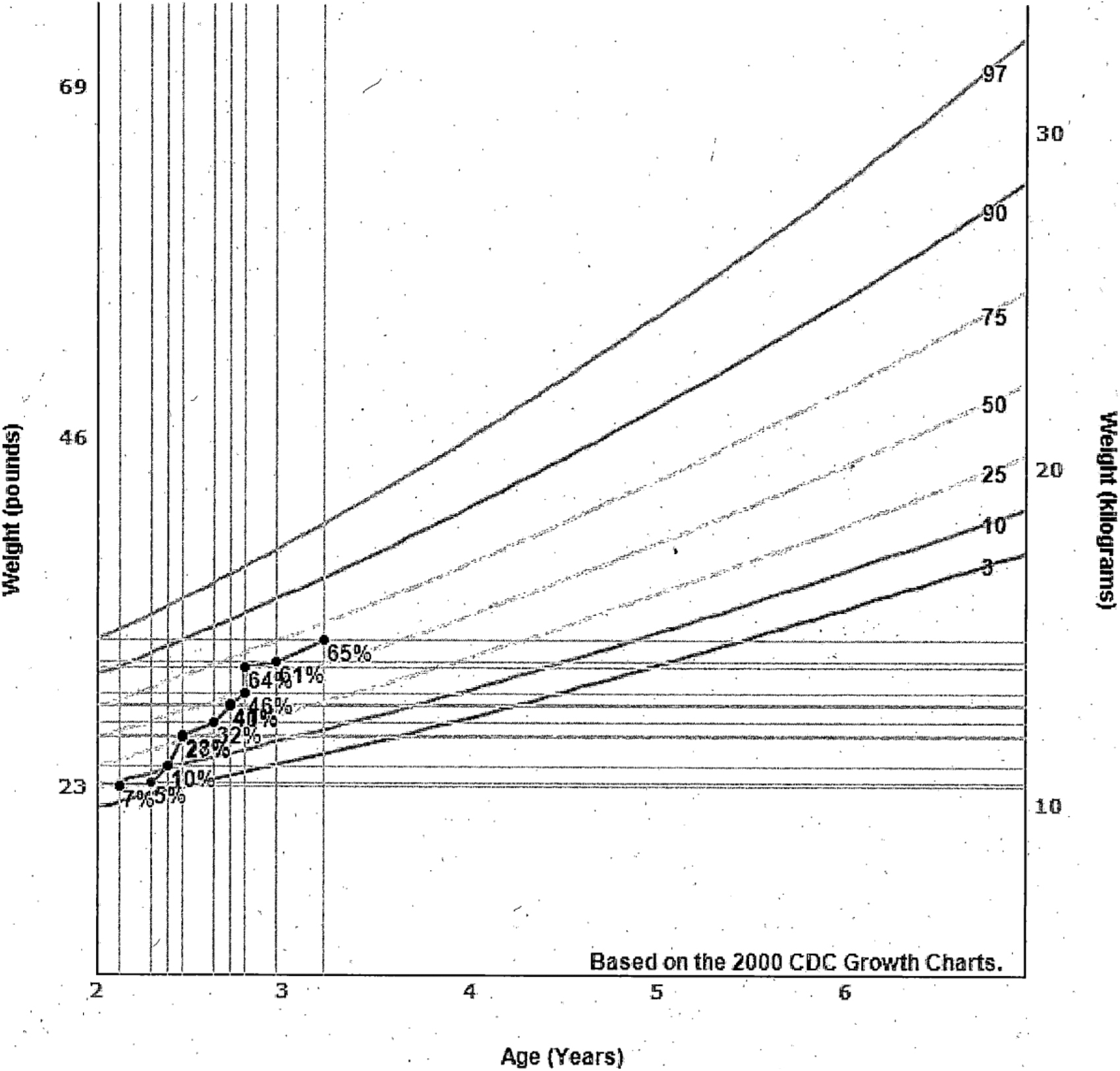
Girl's weight versus age at 24 months to 20 years. CDC, Centers for Disease Control and Prevention.
Her height started at the third percentile at the first treatment. Measurements showed periodic steps just above or below the 25th percentile line (Fig. 2) after the first month of treatment. The last measurement after the last treatment was at the 37th percentile. This also crossed 2 major percentile lines and approached a third major percentile line. Overall, such a result is far beyond the typical goal of therapy for FTT. This increase was despite no change in the exclusive nutrition via j-tube feeds. There was no change in the formulation or composition of the tube feeds during the treatment period.

Girl's stature versus age at 24 months to 20 years. CDC, Centers for Disease Control and Prevention.
Posture
There was no change in the patient's posture noted until the fifth visit. At that visit, she had a relatively straight posture for the first time, presumably from local scar-stimulation treatments. There were no other conventional interventions performed for this issue.
DISCUSSION
FTT is a high-risk condition for young children that may lead to growth- and developmental-delays. If there is good caloric intake, the cause may be organic. When FTT persists beyond 6 months of age, there may be increased rates of depressed psychomotor scores and high rates of school failure. 17 Among the mechanisms of poor growth are inadequate absorption of nutrients and increased metabolic demand, both of which could have had roles in the current patient, with multiple chronic conditions and a stable caloric intake. Because the issue may have been related to caloric usage rather than socioeconomic status, treatment was targeted to her GI system.
It is not unusual for acupuncturists who treat children to be willing to treat FTT, but there is a lack of treatment standardization and there have been no notable scholarly articles published on this subject. Acupuncture treatments were selected to impact the GI system, using both traditional and auricular acupuncture points. Because this case involved a very young nonverbal child, who had an extensive, very invasive medical-intervention history, stimulation was only applied with the Pointer Plus device without the use of needles. A textbook on pediatric acupuncture by Scott and Barlow, noted that FTT can be caused by weak Kidney energy, insufficient Qi from the parents, or another pathologic factor. 18 Scott and Barlow's treatment for lingering pathologic factors included ST-36, SP-6, and CV-12 with moxibustion at CV-12; for weak Kidney energy, the recommended treatment was BL-20, BL-23 and SP-6; and other points, depending on specific symptoms. 18
Bahrami et al. noted possible GI indications for acupuncture in children with constipation and nausea and vomiting. 19 Loo mentioned many GI treatments for children with various conditions, but none were close to low weight, weight loss, or FTT. 20 Others who performed pediatric acupuncture typically used massage of acupuncture points in children.
In this FTT case, CV-4, CV-6, CV-12, BL-21, BL-25, BL-27, and ST-25 were selected for their usefulness for GI disturbances, because it was thought was that calorie absorption due to the patient's tracheoesophageal fistula history was the culprit, and there did not appear to be any other offending, ongoing FTT etiology.
There were no English-language journal articles found on acupuncture treatment for FTT, nor were there any that mentioned nonneedle electrical stimulation of acupuncture points in children. The main pertinent result on acupuncture for FTT was in Korean by Lee et al., but this article was not available online or in English. 21 Expanding the search for weight yielded a study by a different Lee et al., which assessed the literature on idiopathic short stature and did note some benefit when treatment was combined with growth hormone, but included acupuncture with other traditional Eastern medicine treatments. 22
Guo et al. assessed acupuncture at Sifeng (Ex-UE-10) with Wang's Baochi Pill for pediatric malnutrition and found that the acupuncture with these pills was better than the pills alone. 23 Given that this study was not cited in a medical journal and was in Chinese, no other details on this article were available.
Lee et al.'s anorexia (as a symptom) article was somewhat related to this case, reviewing 32 randomized controlled trials, all in Chinese from China, concerning acupuncture treatment for childhood anorexia. 24 Sifeng was the most commonly used point with a 3-edged needle, treating once per week for a typical duration of 1 month. 24 Acupoint herbal patching, manual acupuncture, laser acupuncture, acupressure, moxibustion, and combinations produced improvements in anorexia with no adverse events reported. 24 Most of the other closest results had to do with acupuncture for abdominal pain, colic, or acute GI surgical issues.
Loo mentioned many GI treatments in children for various conditions, but no specific acupuncture treatment. 20 In the same publication, Loo, states that gastroesophageal reflux disease (GERD) is another cause of FTT but states there are no acupuncture studies on this. However, in the case at hand, the child did not have GERD.
Typically, electroacupuncture (EA) involves the use of electricity through needles. As noted previously, this case involved a very young nonverbal child; thus, stimulation was only given the Pointer Plus without the use of needles. This stimulation was set at a fixed 10-Hz and the intensity was adjustable according to product specifications. 17
The milk, mixed in the otherwise stable formula for the tube feeds, is a confounding variable that makes it difficult to ascertain the degree of benefit from the calories and from the acupuncture. The erythromycin added at the 4.25-month point could also have been a confounder, but it is associated with possible side-effects of pyloric stenosis, abdominal pain, anorexia, nausea, vomiting, and diarrhea which would have been unlikely to help this patient's weight. 25
CONCLUSIONS
In this case, nonneedle acupuncture was helpful. The case highlights the potential benefit of nonneedle stimulation of typical acupuncture points in children. More research is warranted, but this case showed the utility of EA stimulation in a very young child.
Footnotes
AUTHOR DISCLOSURE STATEMENT
There are no competing financial interests.
FUNDING INFORMATION
No funding was received for work on this article.