
Abstract
Objective:
Stiff person syndrome (SPS) is a rare neurological disorder. Treatments are limited, and non-pharmacologic therapies are recommended based on symptomatology. A G2P2002 post-menopausal 60-year-old female with hypertension, obesity, and type II diabetes, and SPS secondary to a paraneoplastic process cause by endometrioid ovarian adenocarcinoma who presented to acupuncture clinic seeking treatment for SPS and its sequela. Her main complaints upon presentation included muscles spasticity causing low back pain, hip flexor pain, insomnia and chemotherapy induced peripheral neuropathy. Her mood and quality of life were also noted to be poor at presentation.
Materials and Methods:
A case report of implementation and customization of acupuncture treatment protocol for the sequelae of SPS including painful spasticity, insomnia, and reduced quality of life is discussed. Outcomes included measures of stiffness (degree of stiffness, distribution of stiffness, heightened sensitivity score) at each visit and health-related quality of life 14 item index at baseline. These outcomes were measured at the initiation of the acupuncture intervention (baseline) and after 9 weeks of weekly acupuncture treatments. These treatments included body acupuncture, electro acupuncture and auricular acupuncture. Acupuncture was performed in addition to her ongoing IVIG therapy.
Results:
Forward bending increased with maximal benefit observed by treatment 3. Lateral bending showed significant improvement with maximal effect by treatment 4. Timed activity testing (walk and stair climb) initially did not improve but showed a significant and sustained improvement following acupuncture protocol change following week 5. The self-rated quality of life outcome measure of overall health was unchanged (“good” at baseline and at follow-up), but all other quality of life outcome measures showed improvements.
Conclusions:
SPS is a rare disorder causing substantial impairment for patients affected. The evidence supporting the use of acupuncture specifically for SPS is at most limited, however, the evidence supports the use of acupuncture for many of the symptoms experienced by those with SPS. This case illustrates how acupuncture can be considered as an adjunct therapy to improve the quality of life and function of these patients. More studies are needed to further investigate and optimize acupuncture treatment protocols for this rare disease.
INTRODUCTION
Stiff person syndrome (SPS) is a very rare neurological disorder with the hallmark symptom being painful axial or extremity muscle rigidity. 1 Other findings can include brainstem and cerebellar dysfunction and progressive encephalomyelitis. 1 The symptoms of SPS can be vague and vary greatly from one patient to another. SPS can manifest in a variety of ages and ethnicities with middle-aged Caucasian women presenting more frequently. 1 The rare prevalence and the varied nature of presentation often delays identification of this disease and can result in delayed treatment. 1 The etiology is thought to be autoimmune as most patients are found to have antibodies to GAD65, an enzyme involved in the synthesis of γ-aminobutyric acid (GABA); a minority of patients instead have antibodies to the glycine receptor which is located on inhibitory neurons. Antibodies to the glycine receptor cause internalization of the receptor into the neuron, thus inhibiting neuron signaling. 1 A small number of cases (∼5 percent) are thought to be paraneoplastic 1 and have been associated with small cell lung cancer, lymphoma, and breast cancer. 1 Benzodiazepines are first-line therapy followed by immune therapies such as IVIG and therapies that are GABAergic. 1 SPS treatments are limited in number, and non-pharmacologic therapies are recommended based on symptomatology. 2
CASE REPORT
A G2P2002 post-menopausal 60-year-old female with hypertension, obesity, and type II diabetes presented to acupuncture clinic seeking treatment for SPS and its sequela. She had a history of IC1 grade 1–2 endometrioid ovarian adenocarcinoma s/p hysterectomy and salpingo-oophrectomy, chemotherapy, and radiation. Her initial symptom was right lower extremity weakness around the time of her hysterectomy. At 4 months following her cancer diagnosis, she had developed intense acing pain in bilateral legs, constipation, anxiety, and insomnia. These symptoms progressed despite multiple medication trials with minimal improvement and significant side effects including gabapentin (falls), amitriptyline, doxepin, lorazepam, trazodone (double-vision), duloxetine, cyclobenzaprine (sedation), tizanidine (confusion), baclofen (hallucinations), valium, suvorexant, and prednisone. Diagnosis of SPS was confirmed with electromyography testing 16 months following her initial symptoms. Her testing for antibodies to GAD65 and amphiphysin were negative, but she was found to have antibodies to the glycine receptor, making her case even more rare. Her main disease related symptoms upon presentation to acupuncture clinic included muscle spasticity, low back/hip flexor pain, and chemotherapy induced peripheral neuropathy (CIPN). She had received seven IVIG infusions across the previous 11 months with little improvement prior to presentation. Her quality-of-life sequela included insomnia, fatigue, and mood disturbance. Her overall physical mobility had greatly deteriorated, and she was using a cane and sometimes a wheelchair to assist mobility. She was not sleeping well and was missing work frequently. Her mood was poor upon presentation, and she was extremely frustrated by her loss of independence and required assistance with daily activities.
TREATMENT
Rationale
No literature was found specific to point selection for SPS. Studies were reviewed that investigated acupuncture for symptoms and sequalae that are commonly seen in SPS. Studies were reviewed such a spasticity in post-stroke, brain injury, and cerebral palsy.3,4 Several acupuncture styles were used in treatment design based on symptomatology. A Traditional Chinese Medicine acupuncture approach for point selection was employed for well-established indications. A neuro-anatomical approach was utilized for pain. French Energetics was used for pain and fatigue. Auricular and electroacupuncture (EA) were used for treatment augmentation. All EA was applied using ITO ES-130 devices with current applications measured in milliamps. Some points had multiple indications and were used for more than one symptom. An asterisk is placed next to the points stimulated.
Needles for body treatment were 0.25 mm in diameter and 60 mm in length, manufactured by DBC and were made of surgical stainless steel with a spring-style metal handle. Needles were inserted until De Qi or muscle twitch was observed. Auricular acupuncture was performed using auricular semi-permanent needles that were manufactured by Sedatelec.
Dispersion technique used included insertion of the needle until De Qi or muscle twitch followed by no further adjustment or stimulation to the needle.
All treatments were performed by the same provider with board certification in Medical Acupuncture and 11 years’ experience. Treatments varied based on patient symptoms and preferences (Table 1). Treatments listed per session were applied simultaneously. Acupuncture treatment outcome measures were collected weekly for a total of 9 weeks with first treatment 1 day post IVIG treatment.
Acupuncture Points Performed by Each Visit Date Including Needle Retention Time
Indicates which points electroacupuncture was applied.
Sishencong: a collection of points 1 cun from GV-20 in the ventral, dorsal and lateral positions.
BaFeng: a collection of points on the dorsum of the foot near the webs of each toe, there are four on each foot.
Ahshi point: an acupuncture point that manifests are painful or tender when palpated.
Muscle Spasticity
Acupuncture points chosen included LI-4*, SP-6*, ST-36*, ST-41*, GV-20, GB-34*, and LR-3* and were based on point attributes 3 and practitioner experience. For treatments 1–2, EA was applied for a desired frequency of 100 Hz, and the output intensity dials were adapted to comfortable patient stimulus recognition. Stimulation was adjusted after 6 min to address accommodation. Due to decreased sensation, she required higher than normal intensities. For treatments 3–4, EA was applied for a desired frequency of 4 HZ, and the output intensity adjustment dials were adapted to comfortable patient stimulus recognition. This change in frequency was made due to the patients difficulty with appreciating electrical stimulation when using 100 Hz. Treatment was applied for 12 min for the first 4 treatments and for 20 min for subsequent treatments.
Chemotherapy Induced Peripheral Neuropathy
Treatment included EX-10 (Bafeng)*, LR-3*, ST-41*, ST-36* and LI-4*, based on practitioner experience and most commonly used points for CIPN5. Needles located in the first and second web space of the foot were crossed and clipped with the cathode of an alligator clip set, and LR-3 was clipped with the corresponding anode. Needles located in the third and fourth web space of the foot were crossed and clipped with the cathode and ST-41 was clipped with the corresponding anode. EA was applied at a frequency of 60 Hz, and the output intensity dials were adjusted to comfortable intense stimulus recognition. Stimulation was adjusted after 6 min to address accommodation. LI-4 was clipped with the cathode, and ST-36 was clipped with the corresponding anode. EA was applied at a frequency of 4HZ, and the output intensity adjustment dials were adapted to comfortable patient stimulus recognition. Treatment was applied for 12 min for the first 4 treatments and 20 min for subsequent treatments. Bafeng and other points were applied during treatments 1–4, auricular acupuncture was applied during treatments 5–8 as indicated via ear scanning.
Insomnia/Fatigue/Mood
Treatment included EX-NH1 (Sishencong), GV-20, GV-24, Yintang, HT-7, and SP-6, based on practitioner experience, point attributes, and previous work.5,6 All points were center in dispersion during treatment except for SP-6. The Shao Yin-Tai Yang channel was used to combat fatigue in treatments 3, 4, 5, 7, 9, and 11 and included KI-3, KI-10, and BL-60 bilaterally. These were center in dispersion.
Low Back Pain and Hip Spasticity
Protocol was adjusted during treatments 6–11 for patient endorsement of increased low back pain and hip stiffness. Neuro-anatomical approach used was based on the author’s previous work.7,8
OUTCOME MEASURES
Measures of stiffness included degree of stiffness, distribution of stiffness, and heightened sensitivity score.9,10 Degree of stiffness was determined based on measured bending of the spine and timed activity tests. Distribution of stiffness was determined based on number of body areas with stiffness from a predefined list. Heightened sensitivity score was determined by a count of triggers for increased stiffness from a predefined list. Baseline stiffness measurements were collected 1 day prior to IVIG infusion and 1 week prior to the first acupuncture session. Stiffness measures were repeated before each acupuncture treatment session. Quality of life outcomes of general, physical, and mental health as well as pain, mood, and sleep were assessed using the health-related quality of life (HRQOL) 14 item index 11 and were collected at baseline described above and after 3 months of acupuncture therapy.
RESULTS
Differences from baseline in bending measures are presented in Figure 1. Forward bending increased with maximal effect by treatment 3. Lateral spine bending showed significant improvement with peak benefit by treatment 4. Both declined after acupuncture protocol change with only forward bending remaining improved from baseline. These improvements were measurable but not clinically significant to the patient.
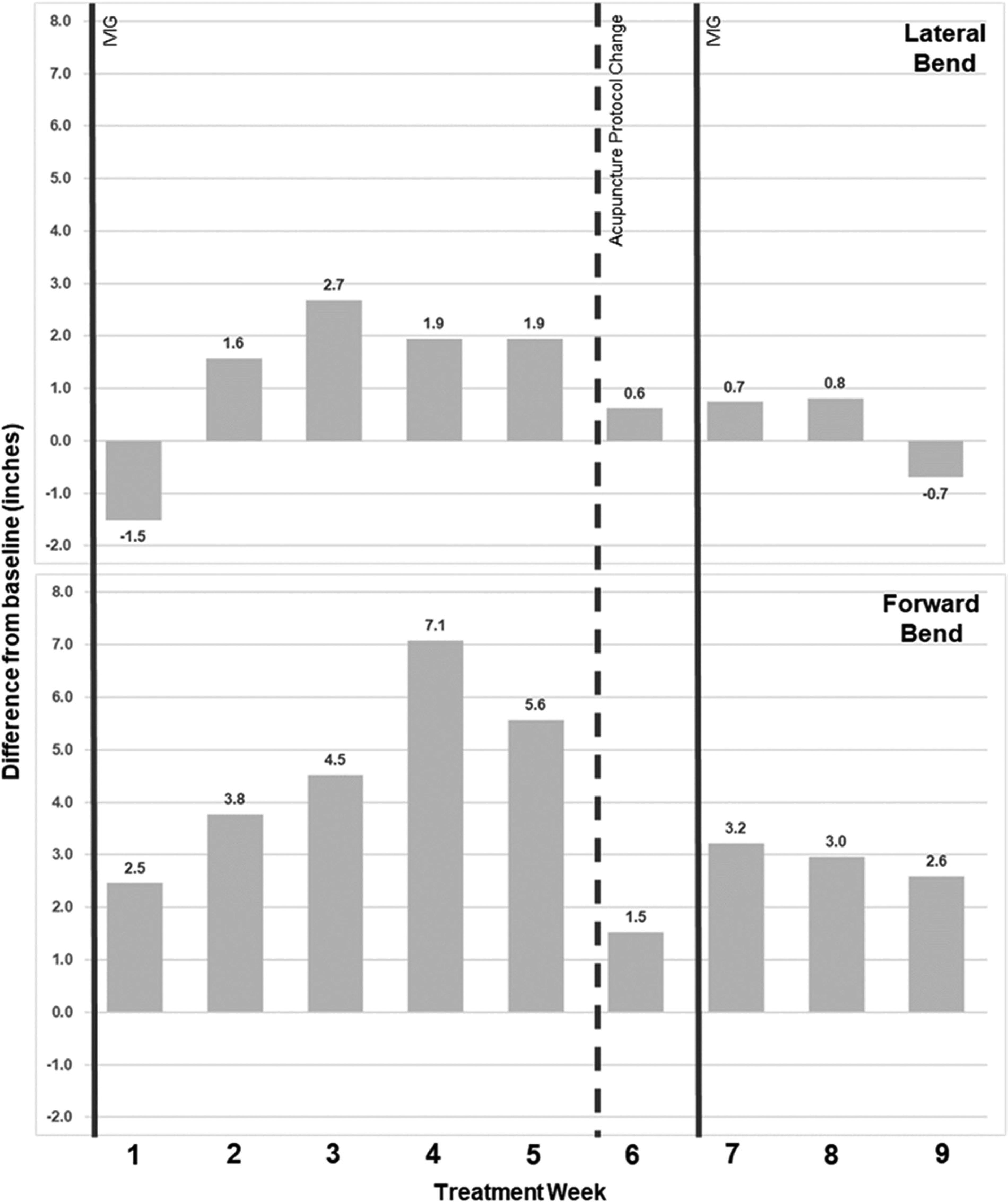
Absolute change (in inches) from baseline of forward and lateral bend measures by week. Timing of IVIG infusions (solid line) and change in acupuncture protocol (dashed line) included.
Differences from baseline in timed activity testing (walk and stair climb) are presented in Figure 2. These measures initially did not improve but showed a significant and sustained improvement following acupuncture protocol change following week 5. This sustained improvement was directly correlated with the change in protocol from traditional body acupuncture point selection to PENS EA combined with Ashi point selection and auriculotherapy. The patient no longer required a cane or other assist device to walk, and her gait and speed of walking were observed to be smoother and more natural.
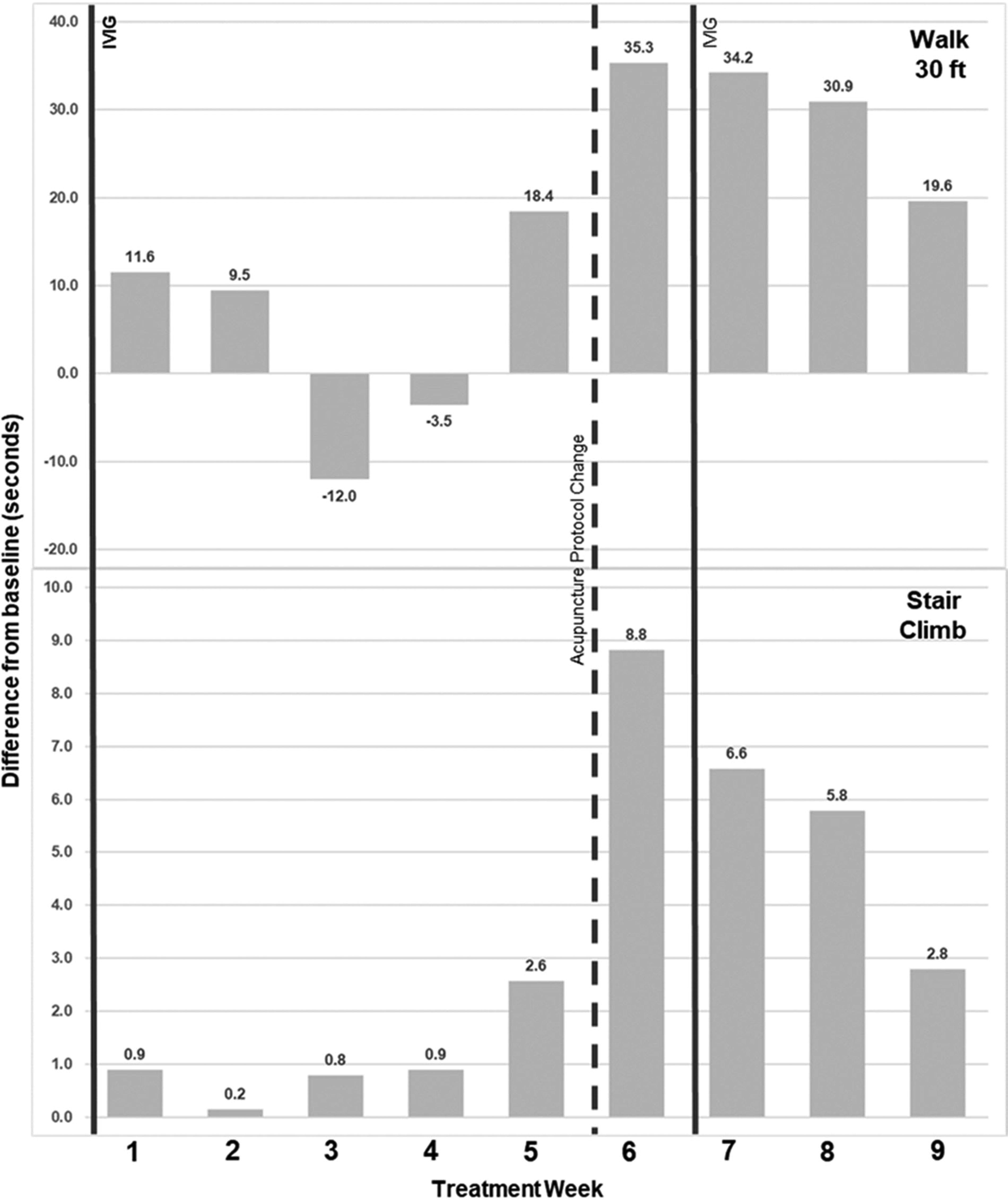
Absolute change (in seconds) from baseline of timed walk and stair climb, measures by week. Timing of IVIG infusions (solid line) and change in acupuncture protocol (dashed line) included. Positive values indicate reduction in time to complete task.
On HRQOL measures patient rated “overall health” as “good” at baseline and following 3 months of therapy, all other measures improved. Patient reported at baseline not getting good rest for 25 out of 30 days, which decreased to 7 out of 30 days at 3 months. Reported days feeling healthy and full of energy increased from 0 of 30 to 14 of 30. Reported days of not good physical health went from 15 of 30 to 5 of 30 and not good mental health from 5 of 30 to 0 of 30. She reported an increase in the ability to perform daily tasks independently, did not call off from work as often, and was able to return to some activities she enjoys.
DISCUSSION
To our knowledge, this is one of the first descriptions of an acupuncture protocol with success in addressing the sequela of symptoms in SPS. This patient presentation is extremely unique in that her SPS was caused by a paraneoplastic process, which is seen in about 5 percent of cases, and the pathogenesis of her SPS was due to antibodies of the glycine receptor, not the more common GAD65 enzyme. She also did not have antibodies to amphiphsin, which is often associated with a paraneoplastic process.
The initial protocol used focused on muscle stiffness and the patient’s objective stiffness measures improved. Although positive progress in stiffness measures was seen, concerns with little change in functional status, mood, sleep and fatigue prompted a protocol change for treatment 6. The patient’s functional ability and low back pain improved significantly after the protocol change and remained improved over the 9-week observation period.
While muscle relaxers and immunomodulators are considered the gold standard for patients with SPS, patients often have refractory symptoms even with treatment. IVIG shows maximum concentrations within 48 hours with wear-off by week 3–4. 12 This patient maintained regular IVIG infusions every 6 weeks during observation. We saw maximum stiffness improvement at week 3–4 during the expected timeframe of IVIG wear-off. This suggests the acupuncture protocol was either directly responsible for the observed improvement or aided sustainment of IVIG treatment effects. Independent effects of the acupuncture protocol are also supported by patient report of little to no improvement in sleep, fatigue, mood, and low back pain during the seven IVIG infusions prior to the addition of acupuncture.
The patient did not experience any relief of CIPN following acupuncture treatments. One explanation could be that treatments were aborted after an average of 5 weeks due to patient preference of change in protocol focus while acupuncture for CIPN shows highest efficacy after longer treatment durations. 13 Also, acupuncture is thought to work by enhancing GABA receptors, 13 which are closely related in function and proximity to glycine receptors damaged by antibodies detected in this patient. It is possible these damaged receptors diminished the potential effects of acupuncture.
Overall, the patient experienced measurable improvements in stiffness, but this did not result in subjective improvement. The changes in activity performance correlated with the protocol change, which was designed to better manage the patient’s pain. The patient did describe an improvement in her pain, which correlated with the improvement in her measurable activity, mood, and sleep scores. This highlights the importance of focusing on patient symptoms rather than only on the stiffness itself.
CONCLUSIONS
SPS is a rare disorder causing substantial impairment for patients affected. Current treatments are helpful but there are limited options and they often come with significant side effects. Acupuncture is a safe and effective treatment with evidence supporting its use for many of the symptoms experienced by those with SPS. This case illustrates how acupuncture can be considered as an adjunct therapy to improve the quality of life and function of these patients. More studies are needed to further investigate and optimize acupuncture treatment protocols for this rare disease.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.