
Abstract
This clinical study looks at radial pulse findings using Chinese Pulse Diagnosis (CPD) in the diagnostic assessment of the acutely hospitalized adult to verify CPD as a diagnostic tool and more quickly develop a more precise differential diagnosis. Pulse findings collected, blinded initially to patient history, physical exam, diagnosis, or treatment plan for 132 patients, were later compared with the evolving assessment and plan for the patient using the electronic medical record for chart review. Correlations were drawn between different aspects of the pulse and later diagnosed allopathic medical conditions. The neuro psychological rough vibration pulse had the strongest association with psychiatric diagnoses. Gender-related pulse predominance for female/right and male/left pulses was statistically significant. Evaluation of organ systems among pulse findings demonstrated concordance with principal Western diagnoses that did not reach statistical significance due to the lower number of patients in various diagnostic groups.
INTRODUCTION
Pulse diagnosis has arisen in medicine in multiple cultures (Chinese, Tibetan, 1 Ayurvedic, Greco-Persian, Japanese, 2 Arabic, and Hebrew 3 ) over time. Whether there was a transfer of medical knowledge related to trade routes, or this way of knowing occurred independently, is unknown. Most intriguing is the development of pulse diagnosis among Yucatan Mayans, with no known prior Eurasian contacts. 4
Chinese Pulse Diagnosis (CPD) is one aspect of Chinese medicine stretching back to the first century BCE, where it was first described in the Huang Di Nei Jing (Yellow Emperor’s Cannon of Internal Medicine). Early in the Western Jin Dynasty (265–316), details of pulse diagnosis were summarized in the Mai Jing. CPD is by Western standards an arcane art. The older apprenticeships were limited to mostly male family lineage, or physicians were affirmed as proficient after decades of training, making this approach to education limited. Different systems have differing verbal or poetic descriptors for pulses that lend to diagnostic confusion and limited translation across systems. 3
Pulse data, like noting an elevated patient temperature, can lead to varied diagnoses and is best utilized in the context of an overall assessment of the patient, including a detailed history and physical exam. CPD is usually performed with the patient at rest and the examiner palpating the radial artery’s pulse using the first three fingers of the examiner’s contralateral hand in a horizontal and supported position. Other systems may use different body pulses or hand positioning. Pulse taking can also be used to assess the efficacy of acupuncture treatment, with a decrease in force or normalization of certain pulse areas following treatment. The extraordinary pulses are eight in number (Figs. 1 and 2), representing a deceptively simpler understanding of the flow and purpose of qi coursing through the body and having multiple associations. 5
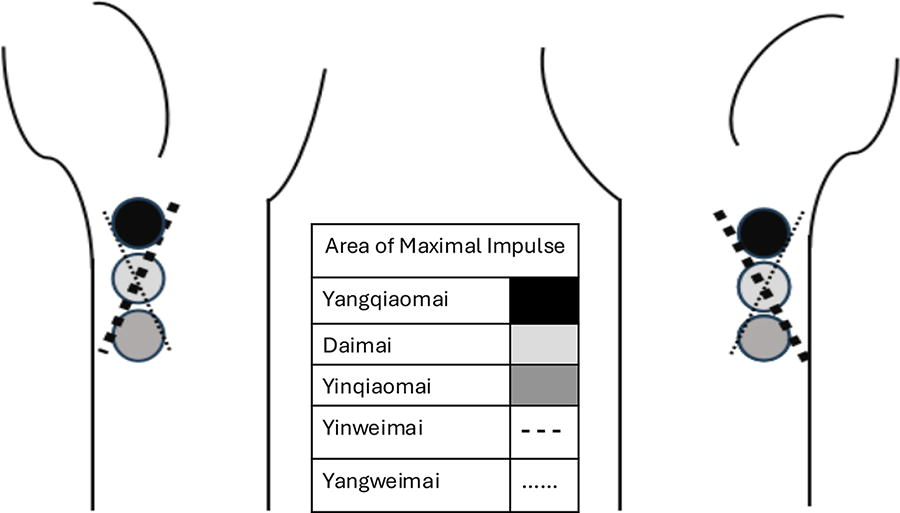
Extraordinary Pulse Locations Along Radial Arteries.
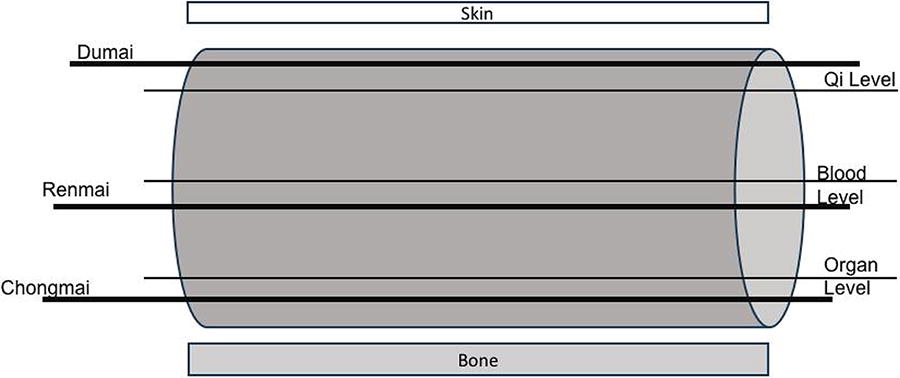
Extraordinary Meridian Pulse Depths Along Length of Radial Pulse.
MATERIAL AND METHODS
IRB approvals were obtained through The Christ Hospital and the University of Cincinnati to carry out this study. Patient recruitment began in July 2020 and ended in May 2022. A total of 132 adult patients (aged 22–86 [average 62]) were recruited among those patients able to give informed consent after their admission to The Christ Hospital Family Medicine Inpatient Team. The investigator initially had access to the patient’s name, age, hospital room number, and fasting status only. The basic premise of the study was explained, and written consent was obtained, including investigator-performed EMR chart review up through 6 months after their entry into the study.
Three different paradigms for CPD were used in this study. Contemporary Chinese Pulse Diagnosis (CCPD), as synthesized into Western language and diagnosis by Dr. Hammer from the Ding and Shen lineage, 6 was chosen because of the accessibility and further development (Figs. 3 and 4) from the traditional Chinese medicine pulse paradigm of six pulse locations and two depths (Fig. 5). Extraordinary pulses were included as a different system to assess the pulse.

Pulse Depths Along Length of Radial Pulse—Contemporary Chinese Pulse Diagnosis.

Left and Right Radial Principal and Complementary Pulse Locations—Contemporary Chinese Pulse Diagnosis.

Principal Radial Pulse Positions and Organ-Meridian Associations.
The pulse diagnosis record (Fig. 6) was adapted heavily from the work of Hammer. 7 No other history was elicited. The patient’s pulse was examined in the supine, semi-Fowler, or Fowler’s position. The wrists were examined with forearms and hands rested gently in supination. Radial pulse findings were recorded on the pulse diagnosis record form. The patients were not asked to exert themselves as part of this assessment, but variations in the rate during the exam were noted if present. There were no other patient contacts or any communication with treating physicians regarding patient care of study enrollees.
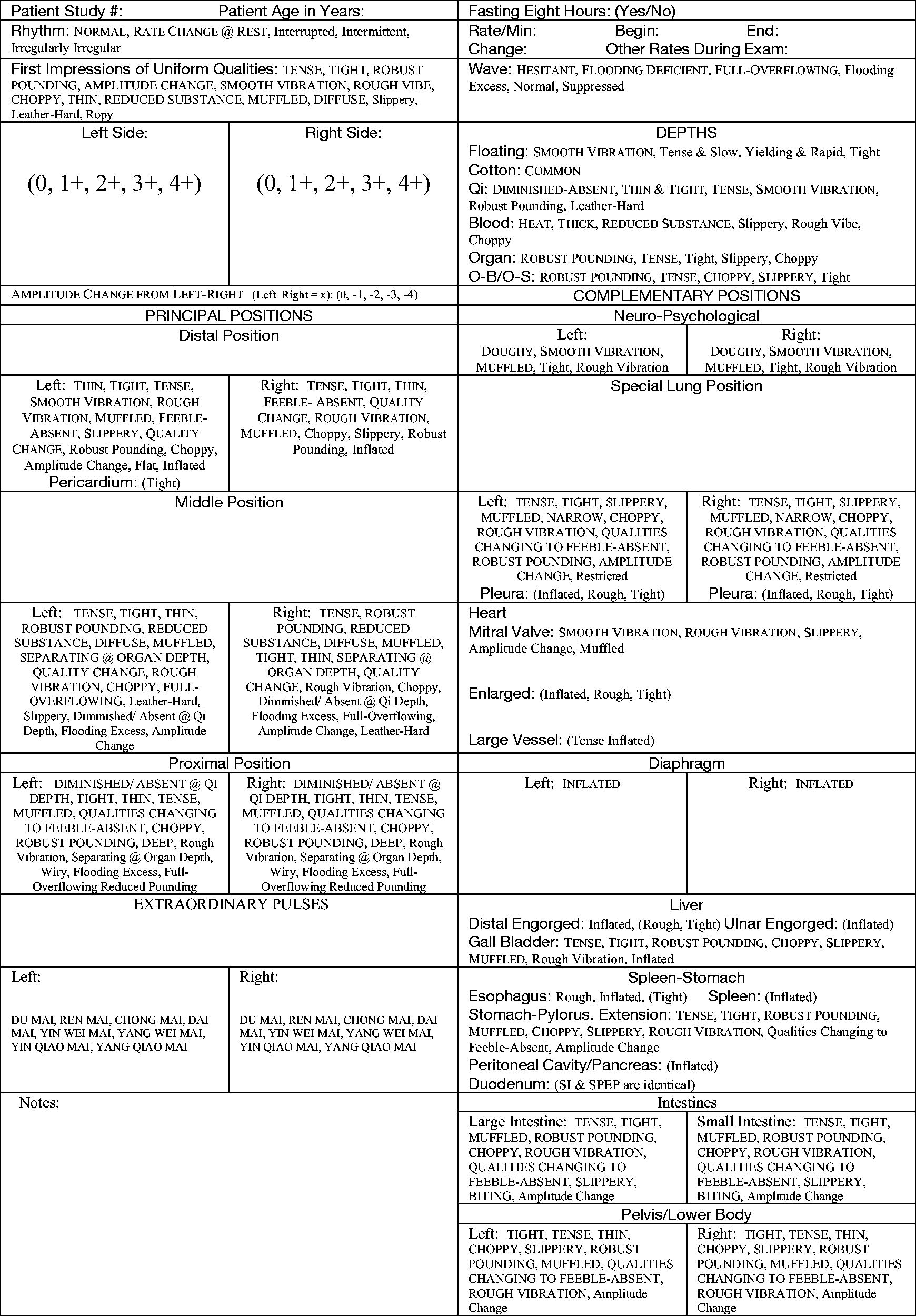
Pulse Diagnosis Record.
The patients’ charts were reviewed in the EMR by the investigator at 1 day, 2 months, and 6 months after pulse data collection. Recorded were the patient’s admitting diagnoses, whether the patient’s major problem was undifferentiated, past medical history, declared gender, medications, types of lab tests done, types of imaging done, and types of physician consults engaged. This information was linked to pulse diagnosis findings. This larger data set was analyzed, comparing major Western diagnostic groups with principal and complementary pulse and extraordinary pulse findings. Descriptor statistics and the chi square test (Fisher’s exact test) were used for comparing female and male pulses using IBM SPSS 29.
FINDINGS
The frequency of 273 pulse findings among major organ systems of the thorax and abdomen was later correlated with diagnostic groups: upper gastrointestinal bleeding, pancreas, diarrhea/colitis, lower gastrointestinal bleeding, biliary colic, transaminitis, urinary tract infection (UTI), congestive heart failure (CHF), atrial flutter/fibrillation, myocardial infarction/cardiac ischemia, chronic obstructive pulmonary disease (COPD), pneumonia, hypoxic respiratory failure, acute kidney injury (AKI), chronic kidney disease (CKD), end-stage renal disease (ESRD), bacteremia, cellulitis, and type 2 diabetes mellitus (T2DM).
For the following Western diseases, ≥50% of patients had the following pulse findings, but no disease category had more than 30 patients. Biliary colic (n = 9) had diminished absent pulses at the qi depth in the left and right proximal positions, a flooding deficient wave, diminished absent pulses at the qi level, reduced substance at the blood level, robust pounding at the organ and bone levels, robust pounding in the gallbladder area, and qualities changing the feeble absent in the small intestine area. UTI (n = 10) was associated with diminished absent pulses at the qi depths in the left and right proximal positions, Yangqiaomai extraordinary pulses, diminished absent or thin and tight pulses at the qi level, thick or reduced substance pulses at the blood level, robust pounding at the organ and bone levels, and qualities changing to feeble absent at the left and right pelvis lower body areas. CHF (n = 20) associated findings were qualities changing to feeble absent in the right proximal position, diminished absent pulses at the qi level, reduced substance at the blood level, and robust pounding at the organ and bone levels. Pneumonia (n = 6) pulses were tense and tight overall, with rough vibration in the right distal position, diminished absent at the qi level, reduced substance at the blood level, robust pounding at the organ and bone levels, and rough vibration at the left special lung position. Atrial flutter/fibrillation (n = 8) associated findings were a flooding deficient wave, diminished absent at the qi level, and robust pounding at the organ level. COPD (n = 13) pulses were tense overall, diminished absent at qi depth in the right proximal position, diminished absent at the qi level, robust pounding at the organ and bones levels, and qualities changing to feeble absent at the left and right pelvis lower body areas. AKI (n = 13) pulses were rough vibration in the right distal position, tense or robust pounding in the left middle position, diminished/absent at qi depth in both proximal positions, a flooding deficient wave, diminished or absent at the qi level, reduced substance at the blood level, robust pounding at the organ and bone levels, qualities changing to feeble absent in the left special lung position, and qualities changing to feeble absent in both pelvis lower body positions. CKD (n = 12) pulses were tense and robust, pounding overall, with robust pounding at the organ and bone levels, muffled in the right special lung position, robust pounding at gall bladder and stomach-pylorus extension, and tight in the large and small intestine positions. Bacteremia (n = 5) associated findings were tense and tight overall, muffled in the right distal position, deep in the right proximal position, a flooding deficient wave, thin and tight at the qi level, and reduced substance at the blood level. Cellulitis (n = 7) associated findings were qualities changing to feeble absent in the left and right proximal position, diminished absent at the qi level, reduced substance at the blood level, qualities changing to feeble absent at the left and right special lung position, and qualities changing to feeble absent at the left and right pelvis lower body position.
For pulse in the CCPD complementary neuro psychological position (n = 47), the smooth vibration, muffled, tight, and rough vibration pulses were more often associated with established psychiatric disorders. Pulses in the neuro psychological position showed up in all the patients with documented bipolar disorder, schizoaffective disorder, mood disorder, and schizophrenia. Rough vibration (83.3%) was the most common pulse quality when any pulse was noted in this position.
Certain disease entities had limited representation in this data set but are remarkable for their findings. The findings in the case for acute thyroiditis were notable for suggesting an acute inflammatory process in the endocrine system at the organ level when the diagnosis was undifferentiated. The patient had no major comorbidities, making pulse diagnosis relatively straightforward. The patient had presented with complaints of shortness of breath and a rash, but the exam, vital signs, labs, and in-hospital workup were inconclusive. It was not until more than a month later, labs finally confirmed the diagnosis of acute thyroiditis, a disease the pulse was already revealing. In the mitral valve position, findings of smooth vibration pulses were noted in two patients who had the only documented mitral valve disease, and a muffled or rough vibration pulse in the mitral valve position was noted in two patients with the only documented aortic valvular disease.
There was a mild increase for the resting pulse among acutely hospitalized patients as compared with normal ranges as tested with CCPD (Table 1). Gender differences (Table 2) were compared in this study and found to agree, with classical Chinese literature indicating that women had right radial pulses, stronger than the left, and men having stronger left-sided pulses (p = 0.001).
Comparison among Acutely Hospitalized Women and Men with Contemporary Chinese Pulse Diagnosis CCPD Pulse Normal Ranges, 3 by Age
Comparison among Acutely Hospitalized Women and Men with CPD Pulse Amplitude Differences. (p = 0.001—Fischer’s Exact Test)
DISCUSSION
CPD has intriguing potential in sifting through the differential diagnosis of the acutely ill hospitalized patient, potentially speeding along that process and reducing unnecessary diagnostic testing and interventions in situations where the western medical differential diagnosis on admission is broad and not as clear. It also has the potential to identify patients who are premorbid, where the patient and physician are unaware of the patient’s impending illness, or objectify disease early in “evolution,” where the physician cannot measure or confirm the patient’s symptoms at that time. It is best done in conjunction with a detailed history and physical exam of the patient, although alone it has predictive power as demonstrated in the case of acute thyroiditis.
This study had only one investigator and no opportunity to compare CPD findings by other examiners contemporaneously, so inter-observer differences could not be assessed. Also, testing was done once and not repeated during the hospital admission, so retesting intra-observer differences were not assessed.
One study 8 refutes the dogma that women have right radial pulses, stronger than the left, and men have stronger left-sided pulses. Another pulse study 9 using machine testing supports a female/right predominant pulse and male/left predominant pulse. In this study, gender differences were consistent with classical Chinese literature indicating that women have right radial pulses, stronger than the left.
Variability of heart rate due to exercise was not assessed, given the presumed frailty of some patients.
Despite the admonition, “Early in the morning…no food has yet been taken…(morning) is the appropriate (time) for pulse examination. Later than that time it is not proper,” 10 most pulse diagnosis occurs in office or clinic settings at various times of the day. Only 15/132 (11.36%) of hospitalized patients in this study reported being in a fasting state at the time of their pulse taking. This number is not enough to make comparisons with non-fasting patients with similar diagnosis profiles. Even in the rather controlled diet setting of a hospital, capturing fasting patient data were challenge. Eating, particularly a larger meal, can shift pulses, particularly in the right middle position. This may explain some of the predominance of Daimai pulses seen.
These patients were evaluated as to their pulse qualities after assessment and treatment had begun in their admission to the hospital. None of them were evaluated in the triage and/or resuscitative care that occurs in the emergency room or intensive care unit, nor immediately upon admission. Pulses measured reflect their subacute disease with some stage of treatment underway. Pulses reflecting comorbidities, which impacted or were affected by the acute process, were difficult to tease out from the principal diagnosis and often showed up in a less prominent way than the pulses associated with disease before treatment has been initiated. Patients usually were on multiple medications. Antibiotics can blunt or muffle a pulse, and beta blockers slow the heart rate.
Patients who had delirium, were nonverbal, or had baseline cognitive impairment were not included in this study. Their care represents a diagnostic challenge for most physicians, as history is an essential component of medical care. Pulse diagnosis may be a tool to assist in initial diagnostic inquiry in these patient groups, in particular.
Pneumonia and CHF often overlap in symptom presentation, and even radiologists have difficulty offering diagnostic certainty. In this study, both disease entities manifested reduced substance at the blood level, diminished absent pulses at the qi level, and robust pounding at the organ and bone levels. CHF-associated findings were remarkable in that most patients had qualities changing to feeble or absent in the right proximal position. These were unique as compared with those for pneumonia, where pulses were tense and tight overall, with rough vibration in the right distal position and rough vibration at the left special lung position. CCPD has a possible role in streamlining diagnosis and tailoring treatment for these initially confusing or overlapping disease entities.
CCPD was limited and unhelpful in diagnosing T2DM as a comorbid factor, and it was not the primary diagnosis among any of the patients.
CCPD was the most complex paradigm used, and yet the multiple pulse qualities assessed allowed for a more robust description of the patient through the pulse. The best description of CCPD, pulse qualities, and their significance comes from the works by Hammer,3,7 and the serious practitioner of CPD would find these resources most helpful. Subsequent research will focus more on the use of this CCPD paradigm.
Most patients with end-stage renal disease already had fistula(s) in place in the arm(s), making radial pulses more difficult to assess.
The most frequently encountered extraordinary pulse finding was Daimai. This number of pulse findings was disproportionately high. It may be artificially elevated because of the noted drug effect on the Daimai pulse, with the use of antidepressants, antibiotics, nonsteroidal anti-inflammatory drugs, steroids, or tranquilizers. 11 Eighty-four of one hundred two patients (82.3%) with Daimai pulses were taking at least one of these types of drugs at the time of their pulse exam. No Yinweimai nor Yangweimai pulses were identified among patients in this study.
The validity and consistency of pulse diagnosis remain a criticism in both Western and Eastern medicine. In one recent study, inter-rater reliability, regardless of the level of training, indicated overall agreement to be low among 38 practitioners in assessing ten patients. 12 Challenges remain in diagnostic accuracy, translation to a western understanding of physiology, and the meanings attached to findings.
On the horizon are electromechanical means of measuring the pulse. Electronic pulse recording has been verified in diagnosing controlled diabetes, hypertension, 13 gastrointestinal disease, hepatic steatosis, 14 and lung cancer. 15 Investigators in Singapore have identified 13 distinct pulse qualities correlated with CPD, using wrist pressure transducers. 16 Moving toward a sophisticated mechanical means may lead to less varied pulse interpretation, either due to skill, pulse-taking paradigm, or inter-tester differences.
CONCLUSIONS
The premise that males tend to have left-sided radial pulses of greater amplitude than females is borne out in this study of acutely hospitalized patients, with a p-value <0.05. In general, patients in this study had slightly higher average resting pulse (79) than average (70) 3 with no gender-related differences.
The results from extraordinary pulses were of limited utility in this study and do not support their use as a quick diagnostic approach. The predominant Daimai pulse among patients in this study may reflect the dosing of pulse-altering medication, acutely ill (sick enough to be hospitalized) constitution, nonfasting status, or other attributes of this pulse type. No diagnoses specific to the Daimai pulse can be drawn from this study because of these confounding variables.
The rough vibration pulse in the neuro psychological complementary position had the strongest association with psychiatric diagnoses. These did not reach statistical significance due to the low total number of neuro psychological pulses detected.
There were multiple data elements identified in this study and not associated uniquely with any diagnosis, confirming CCPD is not a simple paradigm but a rather complex one with nuances appreciated and integrated by skilled pulse takers. Among major Western diagnosis groups of diseases focused on organs in the thoracic/abdominal trunk, there were subtle differences in pulse, but no one pulse quality other than normal rhythm was present in 100% of patients with a given Western diagnosis. A computer algorithm application of pulse findings may lend itself to broader application of CPD in Western medicine.
This study was done, blinded to the patient’s history and exam, to verify CPD in translating those findings to a Western medical paradigm. It included adult hospitalized patients with a wide variety of acute illnesses superimposed on chronic disease, making CPD a challenge. Further CPD data collection among acutely ill patients, including the history and exam at the time of hospital admission, correlated with presumed Western diagnoses, may help provide a larger data set to help further validate CPD pulses as being consistent across a larger panel of patients with similar diagnoses. CPD has the potential beyond Medical Acupuncture or TCM for broader diagnostic use by Western-trained physicians.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
Statistical support in evaluating pulse data was generously provided by the Research Division of the Department of Family and Community Medicine, University of Cincinnati. Sabbatical support for the principal investigator was also provided by the Department of Family and Community Medicine.