
Abstract
Introduction:
Pain after rotator cuff surgery is prolonged. This has led to the need for opioids and the risk of developing opioid use disorder. This study was designed to investigate the role that active auriculotherapy treatment (AT) may play in reducing opioid consumption following rotator cuff surgery.
Methods:
Fifty patients who underwent a primary ambulatory unilateral rotator cuff surgery participated in this randomized, placebo-controlled study. Each patient was randomized to either the AT group or the placebo group (P group). The primary endpoint was overall opioid consumption (oral morphine equivalent in mg) in the first five days after surgery. Secondary endpoints included pain at rest and with movement, non-narcotic analgesic consumption, functional recovery, time to discharge from the recovery room and hospital, patient satisfaction, and the number of patients readmitted to the hospital because of pain.
Results:
The use of AT (n = 20) significantly decrease by 35% opioid consumption (p = 0.0307). The pain with movement in the AT group was significantly lower compared to the P group at 14 days (4.47 ± 2.12 vs. 5.84 ± 2.39, respectively; p = 0.0394). No differences in time to discharge from the recovery room and the hospital and functional recovery were recorded. The use of AT was also associated with an increase in satisfaction at 90 days compared to the P group (5.9 ± 0.3 vs. 4.9 ± 1.9, respectively; p = 0.0267).
Discussion:
Our data, based on a randomized, placebo-controlled study, demonstrated that AT using cryogenic needles and nine ear points is an effective technique to reduce postoperative opioid requirement in opioid-naïve patients following rotator cuff surgery.
Conclusion:
Our data suggest that the use of AT may help reduce opioid consumption following ambulatory rotator-cuff surgery.
INTRODUCTION
Rotator cuff surgery is a model of moderate to severe pain. Although interscalene block is considered an effective technique for postoperative pain management following shoulder surgery, 1 evidence suggests that the duration of the block is short in comparison with the duration of pain after rotator cuff surgery. The discrepancy between the duration of the interscalene block and the duration of the postoperative pain often leaves patients in severe pain and in need of opioids.
The current opioid epidemic has led to a renewed interest in exploring nonpharmacological techniques to treat postoperative pain. 2 This is especially important in the case of upper extremity surgery, since Warrender et al. reported an up to 15% persistence in opioid use in patients undergoing upper extremity surgery. 3 Furthermore, it is well established that the use of opioids is often associated with significant adverse effects, including nausea and vomiting, respiratory depression, hypotension, immunosuppression, and constipation.4–7
Auriculotherapy is a form of acupuncture based on the use of on points located on the ear. It is believed to have been practiced for thousands of years.8,9 Anecdotal reports have suggested that auriculotherapy may be an effective way to treat dental anxiety and pain,10,11 decrease opioid requirement following hip arthroplasty, 12 enhance the quality of recovery, and decrease the frequency of postoperative nausea and vomiting following either gynecological surgery,13,14 or postpartum depression. 15 Recent reviews16–19 concluded that additional evidence is required to determine the role that auriculotherapy may play in perioperative pain management, especially because of the limited number of randomized, placebo-controlled studies demonstrating its effectiveness and the fact that placebo-controlled studies often report no difference between active and placebo treatment.20,21 Furthermore, significant confounding variables prevent validation of the usefulness of auriculotherapy, including the fact that (1) the ear points chosen for a given indication may vary; (2) despite efforts to standardize a universal ear acupuncture chart, different ear acupuncture charts still exist according to country. 22 (3) More recently, authors have proposed different approaches to locate each ear point using a sectogram and point zero as a center of symmetry 23 or using a segmentogram and the corpus callosum; 24 (4) different modes of treatment have been proposed, including needles, 12 lasers, 25 magnetic sticking, 13 and electrostimulation. 15
The current study was designed to assess the role that auriculotherapy may play in reducing the postoperative need for opioids and providing longer lasting analgesia in patients undergoing unilateral rotator cuff surgery under general anesthesia. The study was based on the use of Alimi’s ear cartography 24 and the use of cryogenic “needle” (Fig. 1). In this study, the use of Auriculotherapy was combined with a single interscalene block. The hypothesis was that auriculotherapy could prolong the effects of a single interscalene block and therefore reduce the postoperative requirement for opioids.
METHODS
The protocol was reviewed and approved by the Institutional Review Board (IRB) of the University of Pittsburgh Human Research Protection Office (STUDY18050099) and written informed consent was obtained from all subjects participating in the trial. The trial was registered prior to patient enrollment at http://clinicaltrials.gov (NCT03860259) with Jacques E. Chelly as the principal investigator.
This was a prospective, randomized, placebo-controlled trial conducted at the University of Pittsburgh Medical Center (UPMC) Shadyside and Montefiore hospitals. It included two phases. Phase I comprised the first five postoperative days corresponding to the opioid prescription as written by the surgeons. During this phase, opioid consumption and pain were recorded. Phase II included postoperative days 14, 30, 60, and 90, during which pain and patient satisfaction were recorded.
Recruitment
Patients were recruited in the preoperative holding area of UPMC Shadyside or UPMC Montefiore on the day of surgery. Each patient who agreed to participate signed an IRB-approved informed consent form and was randomized to receive either an active auriculotherapy treatment (AT group) or a placebo auriculotherapy treatment (P group) immediately following surgery in the recovery room. Prior to signing the informed consent, each patient was informed that the treatment might cause possible side effects including local feelings of ear warmth, tingling, local erythema, local edema, blistering, and formation of scabs at one or multiple points. The randomization sequence was determined using computer-generated random numbers. Each patient was made aware at the time of consent and throughout the study that they could choose to withdraw from the study at any time.
Inclusion Criteria
Patients aged 18 years and older undergoing ambulatory rotator cuff repair and who gave consent to have an interscalene block performed prior to transfer to the operating room were eligible for study inclusion.
Exclusion Criteria
Patients with chronic pain requiring daily opioid use, history of opioid use disorder, or contraindications for an interscalene block, including allergy to local anesthetics and anatomical malformation that may interfere with the performance of the nerve block, were excluded. Raynaud’s disease and peripheral vascular disease diagnosis were also criteria for exclusion.
Treatment Groups
Auriculotherapy was performed using cryopunctor (Matauris, Maison Alfort, France) composed of an injector connected to a canister of compressed nitrous oxide gas. (Cryoalfa Europe Ltd., Radebeul, Germany). The cryopunctor is presented in Figure 1. The treatment consisted of nine points on the ipsilateral ear of the surgery. The location of these points was based on Alimi’ cartography and the use of a segmentogram with the corpus callosum as the center of symmetry. 24 The segmentogram for the lateral and the medial aspect of the ear is presented in Figure 2. For the lateral aspect of the ear, the position of each point is described by two coordinates, a letter ranging from “a to k” and a number ranging from “0 to 20.” For the medial aspect of the ear, the position of each point is described by two coordinates, a letter ranging from “A to K” and a number ranging from “0 to XX.” The specific points used for AT included Ω2 (the master point for the mesoderm; A4), the shoulder sensory point (D11); six points involved in the pain pathway at the level of the brainstem and the spine (stellar ganglion [F10]; C7 root, both sensory [C11]) and motor (CXI); sensory master point (SMP; D17); and the reticular master point ([RMP, H13]), thalamus (G14), and ACTH (I17). Figure 3 shows the points treated on the lateral (8 points) and on the medial (1 point) aspect of the ear.
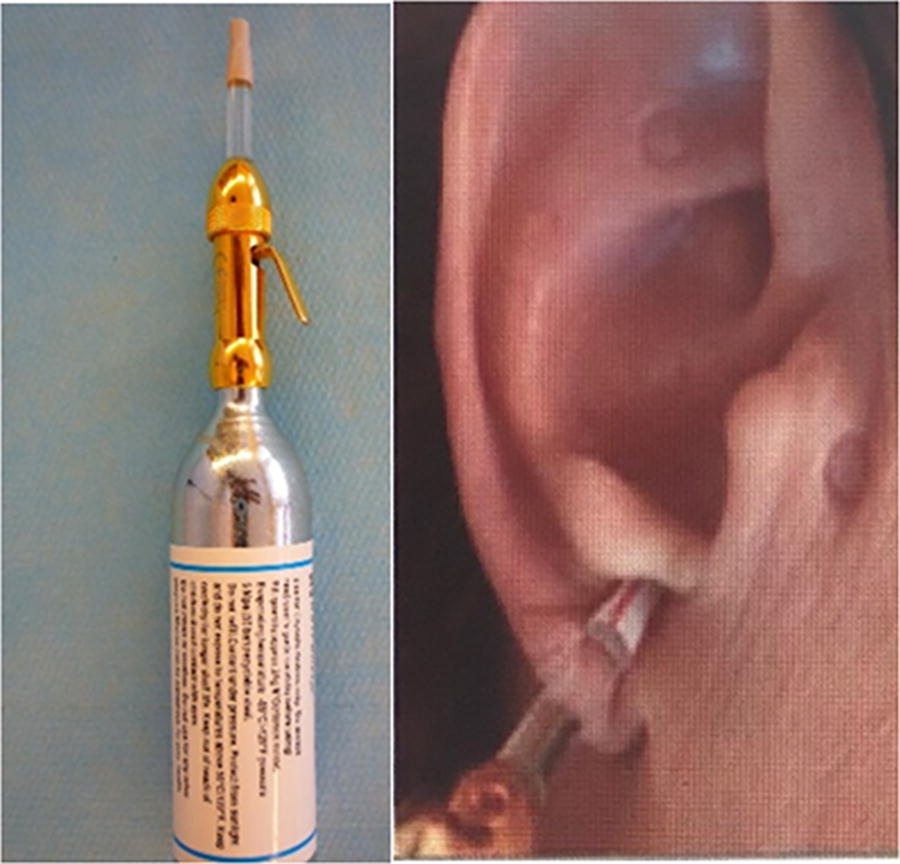
Cryopunctor composed of an injector connected to a nitrous oxide canister.
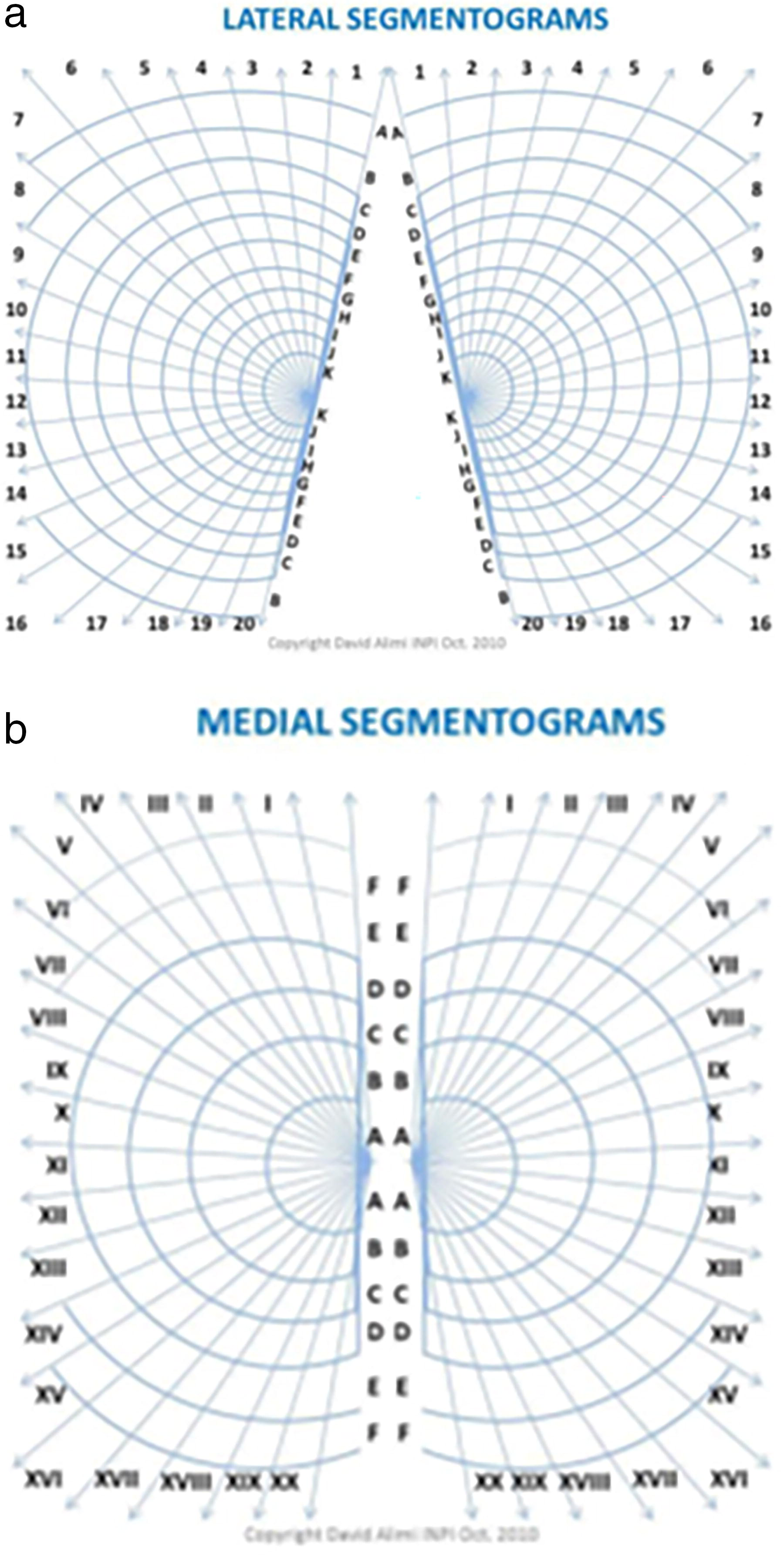
David Alimi’s segmentogram with the corpus callosum as the center of symmetry. Representation of Alimi’s segmentograms of the lateral aspect of the ear with each point located by a letter “a to k” and a number from “0 (corpus callosum) to 20”
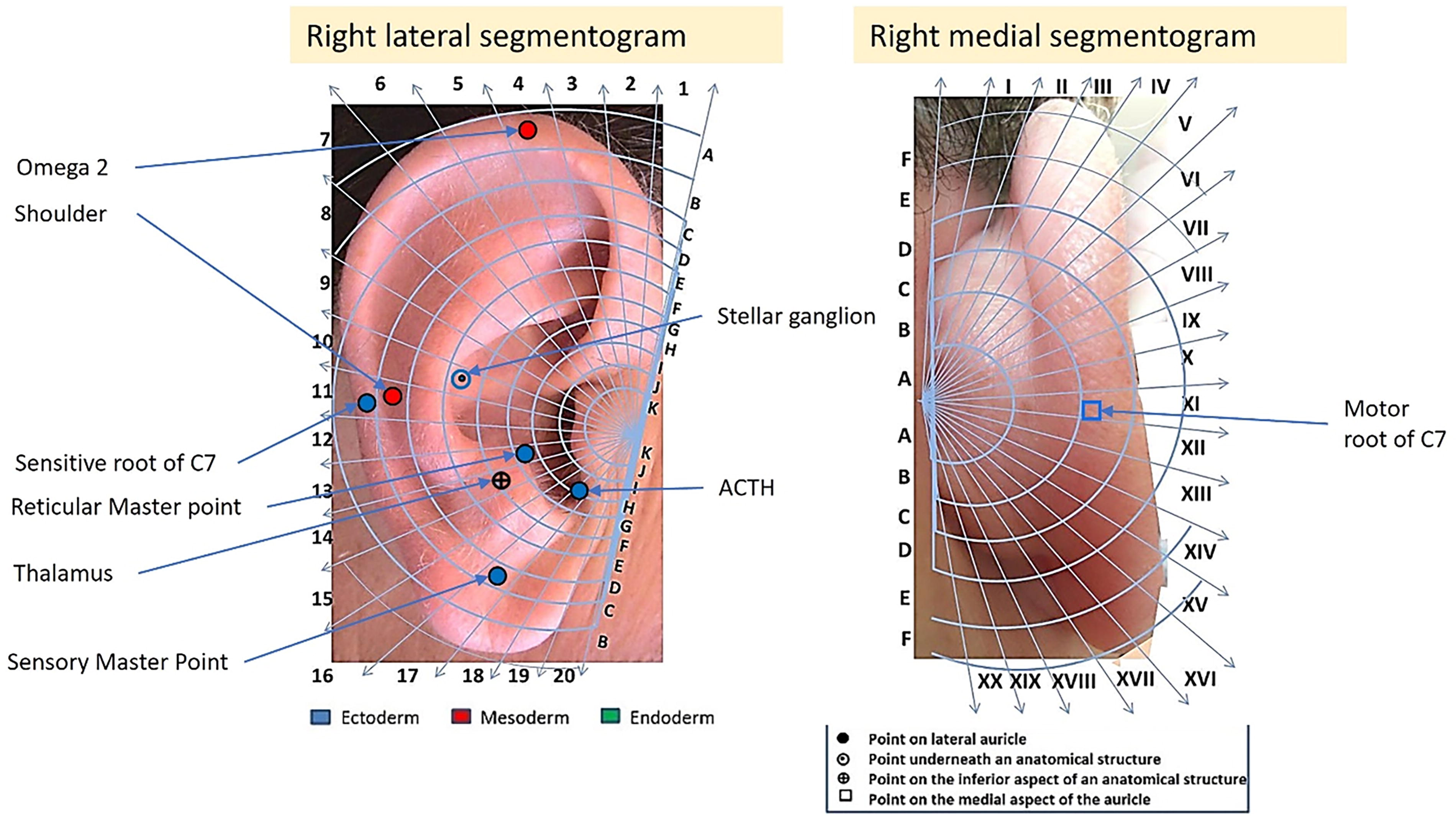
Presentation of the point used for the treatment on the lateral aspect of the ear (8 points) and the medial aspect of the ear (1 point). These points included Ω2 (the master point for the mesoderm; A4), the shoulder sensory point (D11); six points involved in the pain pathway (stellar ganglion (F10); C7 root, both sensory (C11) and motor (CXI); sensory master point (SMP; D17); and the reticular master point (RMP, H13), thalamus (G14), and ACTH (I17).
According to the randomization, each patient received either an active treatment (AT) or a placebo/inactive treatment (P). AT comprised delivery of a two-second burst of nitric oxide gas from the compressed nitrous oxide gas canister (defined as a cryogenic “needle” treatment) at the level of each ear point, whereas the placebo treatment comprised delivery of a two-second jet using an empty canister at the level of each point. Both treatments generated the same noise at the time of administration.
Anesthesia and Postoperative Analgesia
Prior to transfer to the operating room, an interscalene block (12 mL of bupivacaine 0.5%) using ultrasound was performed on each patient. The surgery was performed under general anesthesia. Except for the trained research staff who performed the auriculotherapy treatment, the patient, the health care team (anesthesiology team, recovery room nurses, surgeons, and acute pain team), and research coordinator collecting data were blinded to the patient’s treatment group allocation.
At the time of discharge from the hospital, each patient received a five-day opioid prescription from the surgical team. Each patient was instructed to take acetaminophen and ibuprofen for mild to moderate pain and opioids for pain rated as severe (scale: 0–3 = mild pain; 4–6 = moderate pain; 7–10 = severe pain). Each patient was provided with a diary and instructed to complete it on postoperative days 1, 2, 3, 4, and 5 and return it after completion. Furthermore, each patient was called by a research coordinator blinded to the treatment received by the patient on postoperative day 14, 30, 60, and 90 after the surgery. He/she conducted a satisfaction survey.
Data Collection and Outcome Measures
Primary outcome
All patients were asked to record their daily opioid consumption in their diary. The primary outcome was defined as total opioid consumption between postoperative days 1 and 5, expressed as the area under the curve using a trapezoid approach. Opioid consumption was expressed as oral morphine equivalent ([OME] in mg; with 1 mg of oxycodone PO equivalent to 1.5 mg of morphine, 1 mg of hydromorphone IV equivalent to 21 mg of PO morphine, and 1 mg of tramadol equivalent to 0.10 mg of morphine).
Secondary outcome
Each patient was also asked to record his/her overall pain at rest and during movement over a 24 h period using a verbal analogue scale (0 = no pain to 10 = worst possible pain) in his/her diary from postoperative days 1 to 5, at 14 days, and at one, two, and three months. From days 1 to 5, pain was expressed as the area under the curve using a trapezoid approach. In addition, patient satisfaction related to pain management (0 = very dissatisfied to 6 = very satisfied) was recorded daily by the patient on postoperative days 1, 2, 3, 4, 5, 14 days, 30, 60, and 90 days. Functional recovery was evaluated using the 12-Item Short-Form Health Survey (SF-12) completed prior to surgery and at 90 days following the surgery. The number of patients from each group readmitted to the hospital for pain was also recorded, as were the time to discharge from the recovery room and the time to discharge from the hospital.
Statistical Analysis
Data were analyzed using a modified intend-to-treat analysis. 26 Initial power analysis calculation was based on our prior experience and accounted for 10% of patients not returning their diary as loss of follow-up. We estimated that under these conditions, a total of 50 patients would provide 80% power using a nonpaired one tail T-test to determine the significance of the difference between the two groups. Alpha was set as 0.05. Data are expressed as mean ± standard deviation.
RESULTS
A total of 50 patients signed informed consent forms. Among them, 10 did not return a completed pain diary to report their postoperative pain scores and opioid consumption. Another patient assigned to the P group was excluded because it was found postoperatively that the patient had a history of chronic opioid use. Consequently, 39 patients (20 patients in the auriculotherapy group and 19 patients in the placebo group) were included in the final analysis. Figure 4 presents a flow chart of the patients who provided signed informed consent. Table 1 shows the demographic characteristics of patients included in the final analysis for both groups (age, gender, height, weight, body mass index, and racial distribution).

Study flow chart for all patients who provided signed informed consent.
Demographics of the Auriculotherapy and Placebo Groups (Subjects Involved in the Final Analysis)
Age (mean ± SD), gender (male/female), height (mean ± SD), weight (mean ± SD), body mass index (BMI, mean ± SD), and race distribution (percentages).
Phase I
Primary end point
The use of AT was associated with a significant 35% overall reduction in opioid consumption over the five-day postoperative opioid prescription period compared with P: 62 mg ± 46 OME mg, versus 96 mg ± 67 OME mg, respectively, p = 0.0307.
Secondary end points
Twenty percent of patients in the AT group versus 11% in the P group did not use any opioids over the five-day study period (corresponding to the postoperative prescription of opioids).
Pain at rest was similar in both groups at the time of discharge from the hospital, (0.45 ± 0.76 AT group vs. 0.89 ± 1.91 P group; p = 0.1707) and on the first postoperative day (5.75 ± 3.32 AT group vs. 6.17 ± 3.01 P group p = 0.3446). No difference in pain (using the area under the curve from postoperative day 1 to day 5) was recorded at rest (0.65 ± 7.48 vs. 15.47 ± 9.99 in the AT group vs. the P group, respectively; p = 0.4752) and during movement (21.08 ± 8.62 vs. 24.97 ± 11.29 in the AT group vs. the P group, respectively; p = 0.0827).
At the time of discharge from the hospital, no patients reported any local sensation at the level of the ear such as warmth or tingling, and no local erythema or local edema was recorded. Furthermore, no blistering or development of scabs was reported after discharge from the hospital.
Phase II
At postoperative day 14, pain at rest was similar in both groups, but pain with movement was significantly lower in the AT group versus the P group (4.47 ± 2.12 vs. 5.84 ± 2.39; p = 0.0394), suggesting a long-lasting analgesic effect from the auriculotherapy. Figure 5 shows pain at rest, and Figure 6 shows pain with movement, on postoperative days 14, 30, 60, and 90.
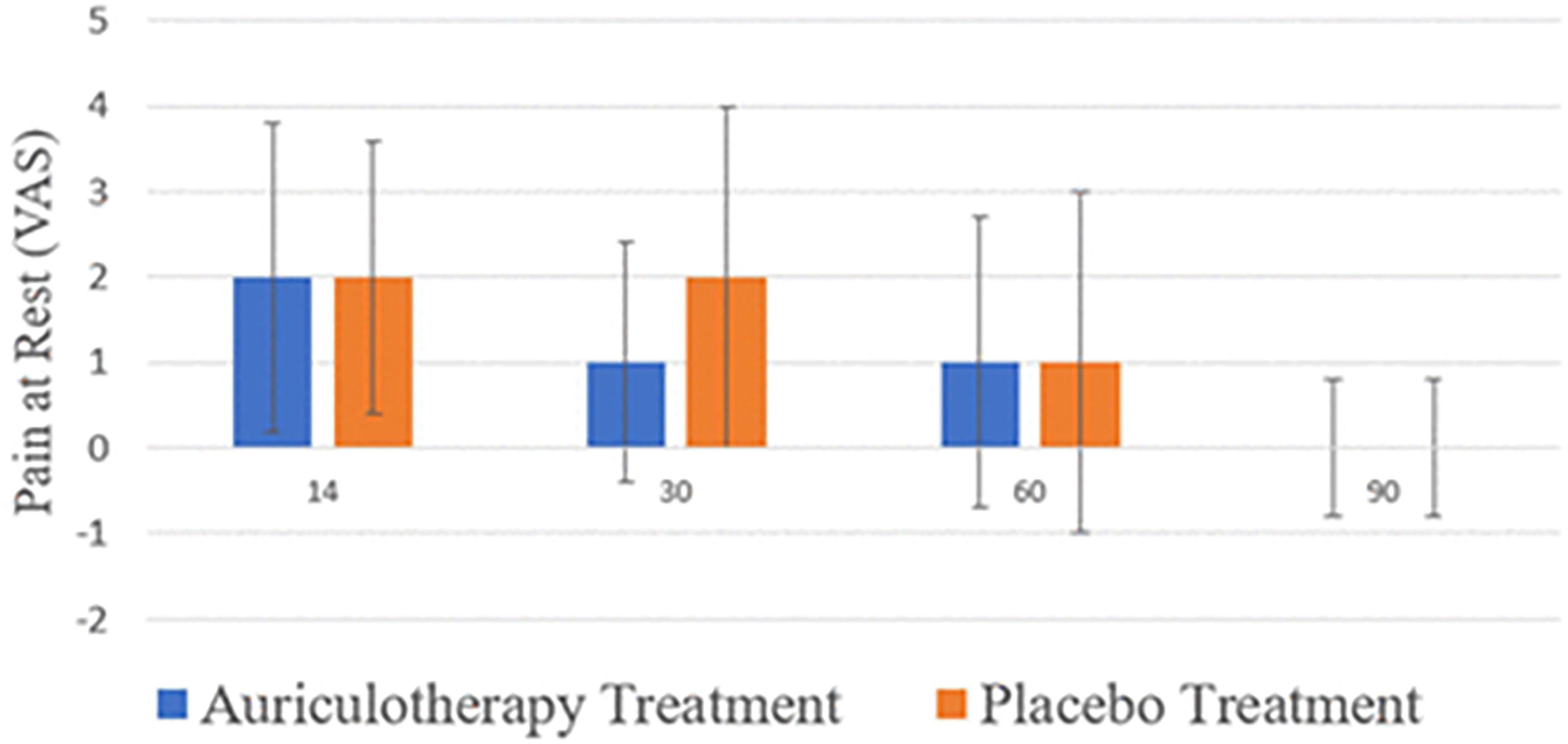
Pain scores using a verbal analogue scale (VAS; 0–10) at rest (mean ± SD) on days 14, 30, 60, and 90 after discharge from the hospital. SD, standard deviation.

Pain scores using a verbal analogue scale (VAS; 0–10) with movement (mean ± SD) on day 14 (*p = 0.0394) and days 30, 60, and 90 after discharge from the hospital.
No difference between groups was recorded with respect to nonopioid analgesic consumption over the study period (acetaminophen: 5956 ± 5882 mg in the AT group vs. 4438 ± 4066 mg in the P group, p = 0.1786; ibuprofen 1370 ± 2386 mg in the AT group vs. 8785 ± 1577 mg in the P group, p = 0.185).
No differences between groups were recorded with respect to either discharge time from the recovery room (67.2 ± 34.1 min vs. 59.5 ± 25.7 min, AT group vs. P group, respectively; p = 0.222) or time to discharge from the hospital (148.0 ± 47.4 min vs. 140.1 ± 32.1 min, AT group vs. P group, respectively; p = 0.286).
Overall patient satisfaction with pain treatment was found to be similar in both the AT and P groups, except on day 90 when patients in the AT group reported being more satisfied than those in the P group. Table 2 reports patient satisfaction scores throughout the study period. Lastly, functional recovery, assessed using the SF-12, was similar in both groups over the study period. No patient was reported as being readmitted to the hospital due to pain during the study period.
Overall Patient Satisfaction (Scale 0–6) with Pain Management in the Auriculotherapy and Placebo Groups
p < 0.05.
DISCUSSION
Theoretically, each ear point exists in two configurations, either physiological or pathological. Depending on the region of the ear, each point, which can also be referred to as a Merkel disc, is characterized by a specific electrodermal resistance that can be detected a specific finder device. Each point receives constant input from the periphery and the brain. In pathological conditions, it is possible to record an increase in electrodermal skin resistance and a tenderness to local pressure. Auriculotherapy irrespective of the technique used to treat the ear points (needles, 2 sec burst of pressured nitrous oxide gas, laser or acupressure) produces a “microlesion” of the nerve terminal branch present at the level of a specific ear point. This microlesion leads to a specific nerve stimulation which is transmitted to a specific area of the brain. The brain responds by reconfiguring the ear point into its original physiological conformation.
Originally, cryogenic therapy was developed to be used by general practitioners, plastic surgeons, and podiatrists to treat very superficial skin lesions. It is based on the release of nitrous oxide stored at high pressure in a canister. Dr. David Alimi developed a specific device, referred to as the cryopunctor, that allows delivery of a very precise amount of high-pressure gas, resulting in a very localized freeze, resulting a very small lesion on the surface of the skin. The US Food and Drug Administration has cleared the use of cryotherapy to treat skin lesion and considers cryogenic devices as class II devices, a classification similar to that given to acupuncture needles. The use of cryogenic “needles” has several advantages. One is that the technique can be used on children and adults, even those with needle phobia. Also, the effects produced by a cryogenic treatment last longer than those resulting from the application of simple acupuncture needles and are comparable to those resulting from the use of semipermanent acupuncture needles, without the risk of needles possibly falling into the ear canal and injuring the tympanic membrane.
This randomized, placebo-controlled study is the first study reporting the used of the cryogenic needles for Auriculotherapy. This study demonstrates that the use of cryogenic needles for AT based on Dr. David Alimi’s cartography 24 allows for a 35% reduction in opioid requirement in opioid-naïve patients following ambulatory rotator cuff surgery with a preoperative interscalene block. Furthermore, 20% of patients in the treatment group did not use any opioids postoperatively versus 11% in the placebo group. This suggests that auriculotherapy may be a technique of interest to limit or even eliminate the postoperative use of opioids following rotator cuff surgery. This study also provide insight on the use of a nonpharmacological approach for the postoperative management of pain following rotator cuff surgery. Thus, previous data reporting the “effectiveness” of auriculotherapy in the treatment of postoperative pain have been based on the use of acupuncture needles,10,11 neurostimulation, 12 magnets, 13 and lasers. 25 There is no evidence showing that these techniques are equivalent. The cryogenic needle developed by Alimi is less traumatic than an acupuncture needle. Its effects seem to be similar to those produced by semipermanent needles. 27 The use of cryogenic needles also provide an original opportunity to use the same ear points for placebo treatment. Prior to the introduction of cryogenic needles, placebo ear points were different from the ear points chosen for active treatment. Choosing other ear points for the placebo treatment may have resulted in producing an “active placebo treatment” and may explain why no difference between active and placebo treatments had previously been reported.
Dr. Alimi’s cartography 24 was initially presented to and accepted by the World Federation of Chinese Medicine and presented at the World Congress of Chinese Medicine on September 3, 2011. It is based on the use of a segmentogram with the corpus callosum as the center of symmetry. It contains 189 points on the lateral aspect of the ear and 89 points on the internal aspect of the ear. The cartography is side-specific, meaning that the representation of the right ear includes the point of the liver, whereas the left side includes the point of the pancreas. The proposed cartography has been validated by magnetic resonance imaging studies, including studies validating the point of the thumb28,29,30,31 and the knee.30,31
The ear points chosen for the treatment protocol were based on the principles of the French ‘school’ of auriculotherapy, led by Dr. Alimi, which promotes choosing ear points based of the physiopathology of the condition being treated. In the case of this study, this meant that the points chosen to treat postoperative pain included the master point for the mesoderm (tissue of origin for the musculoskeletal system), the site of the surgery, and points involved in the pain pathway and inflammation. 31 Such an approach is different from the one used in Chinese acupuncture, which is based on the use of ear points according to meridians and energy (Yan Qi and Yin Qi). 8 The patients included in the study did not have any prior experience with auriculotherapy or more specifically, with cryogenic needles. Therefore, they did not know what to expect from an active or placebo treatment. As stated before, the empty canister used in our placebo treatment produced a noise similar to the one produced by the full canister. Furthermore, it is critical to understand that the treatment was performed while the patient was in the recovery room recovering from anesthesia. This specific environment comprised a powerful condition to assure that the patient was also blinded. By the time the patient recovered from anesthesia and was ready to be discharged, no one had reported any treatment-related side effects. From this, it is possible to conclude that it was most unlikely for the patient to recognize his/her randomization to either the active or placebo treatment group, especially in the absence of any report of blisters or scabs.
In this study, the percentage of patients who did not return their diaries was twice as high as expected (20% vs. 10% original estimate used for the power calculation). This may have been related to a lack of closer interaction between each patient and the research team. To prevent this, we started using an electronic diary (REDCap). Such an approach allows us to verify that the patient has completed the day-to-day requirement and facilitates improved communication with the patient.
CONCLUSION
This randomized, placebo-controlled study based on the use of cryogenic needles, a neurophysiopathologist-based treatment, and Dr. Alimi’s cartography suggests that auriculotherapy performed prior to surgery reduces postoperative opioid requirement and pain with movement for at least 14 days in patients undergoing rotator cuff surgery.
Footnotes
ACKNOWLEDGMENT
The authors would like to thank Christine Burr for editing the article.
AUTHORS’ CONTRIBUTIONS
J.E.C.: Substantial contributions to the conception or design of the study, drafting the work, final approval of the version to be published, and agreement to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. S.L.O.: Substantial contributions to the conception or design of the study, drafting the work, final approval of the version to be published, and agreement to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. M.W.R.: Substantial contributions to the conception or design of the study, drafting the work, final approval of the version to be published, and agreement to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Y.J.G.: Substantial contributions to the conception or design of the study, drafting the work, final approval of the version to be published, and agreement to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. A.L.M.: Substantial contributions to the acquisition, analysis, or interpretation of data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; and agreement to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. D.A.: Substantial contributions to the design of the study, analysis and interpretation of data for the work, drafting the work or revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. S.K.S.: Substantial contributions to the analysis and interpretation of data for the work and revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. K.M.V.: Substantial contributions to the analysis and interpretation of data for the work and revising it critically for important intellectual content, final approval of the version to be published, and agreement to be accountable for all aspects of the work to ensure that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
DATA AVAILABILITY STATEMENT
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.