
Abstract
Background:
This study aimed to investigate the effects of an integrated acupuncture (IA) protocol on blood pressure (BP), depression, anxiety, stress scores, and heart rate variability (HRV) in hypertensive patients.
Methods:
The study was a pilot randomized controlled trial with three arms: IA (acupuncture combined with yoga and naturopathy), sham acupuncture (sham acupuncture combined with yoga and naturopathy), and naturopathy/yoga alone. Sixty participants (20 in each group), of age 30–60 with borderline or stage I hypertension, received respective interventions for 10 days and were followed up for 1 month. BP measurements, depression, anxiety, and stress scores, as well as HRV parameters, were assessed at baseline, after the 10-day intervention, and at 1-month follow-up.
Results:
After 10 days, all groups exhibited a decrease in systolic and diastolic BP, though not statistically significant. However, after 1 month, there was a significant increase in both systolic and diastolic BP across all groups. Depression, anxiety, and stress scores showed nonsignificant reductions after the 10-day intervention, with mixed trends at follow-up. HRV analysis revealed significant increases in SDNN values across all groups and significant changes in LF/HF values.
Discussion:
In conclusion, the 10-day intervention led to slight, non-significant reductions in BP and improvements in depression, anxiety, and stress across all groups, but these effects were not sustained. HRV analysis showed significant improvements in SDNN values and notable changes in low frequency (LF)/high frequency (HF) ratios, suggesting potential autonomic benefits. Limitations of this study, such as the short intervention duration and small sample size, could be the reason for inconclusive results, indicating the need for well-powered randomized controlled trials.
Keywords
INTRODUCTION
Hypertension is a widespread systemic disease that affects more than 31% of the world’s population. 1 This number is expected to grow exponentially considering the global increase in the aging population and increased exposure to lifestyle-related risk factors. 2 Further, elevated blood pressure (BP) is regarded as an independent risk factor for cardiovascular diseases, cerebrovascular diseases, and chronic kidney diseases. 2 Hypertension affects both men and women equally and is especially prevalent in low- and middle-income countries. 1 In addition to the pharmacological interventions, numerous non-pharmacological approaches like dietary changes, physical activity, sun exposure, and yoga have been shown to be beneficial in the management of hypertension.
Acupuncture, a traditional Chinese medicine modality, is increasingly becoming popular as an alternative medicine approach in the management of various lifestyle disorders. However, the role of acupuncture in lowering BP remains inconclusive.3,4 Though certain studies indicate potential benefits of acupuncture for hypertension,5,6 a substantial body of evidence indicates limited or negligible efficacy in reducing BP.4,7
Acupuncture is widely used in India as an integrated therapy along with yoga and naturopathy, one of the official indigenous systems of medicine in India. 8 Except for neuromuscular conditions, the use of acupuncture as a stand-alone practice for lifestyle disorders (diabetes mellitus, hypertension, obesity, metabolic syndrome) is seldom practiced in Indian clinical settings. In these settings acupuncture is always used along with other yoga and naturopathy modalities like hydrotherapy, diet therapy, ozone therapy, yoga therapy, heliotherapy, and mud therapy. However, globally, acupuncture is also used as a stand-alone regimen alongside conventional therapies for lifestyle disorders.9–11 Therefore, it will be interesting to see which approach—acupuncture integrated with naturopathy and yoga (NY) or NY alone—has a better impact on hypertension.
The current study uses a pilot randomized control trial design to investigate whether acupuncture combined with yoga and naturopathy interventions, yoga, and naturopathy interventions as a stand-alone therapy, or sham acupuncture (SA) combined with yoga and naturopathy interventions is effective in lowering BP and influencing other clinical parameters associated with hypertension in patients with borderline and stage I hypertension.
MATERIALS AND METHODS
Study Setting and Ethical Consideration
The study was conducted between May and August 2022 at a private yoga and naturopathy medical college and was approved by the Institutional Ethical Committee of the institute (F.No. 12/SHMCNYS-IEC/P51/2021-2022). The study was registered as a clinical trial in the Clinical Trial Registry of India (CTRI/2022/04/041743). All the participants signed an informed consent form before participating in the study.
Study Design and Study Participants
This was a pilot, randomized, placebo-controlled trial with three arms. There were a total of 84 participants who were evaluated for eligibility; 20 of them failed to meet the eligibility requirements, and four of them had concurrent medical conditions, which resulted in their elimination. The remaining 60 participants were randomly assigned to the integrated acupuncture (IA) group (n = 20), the SA group (n = 20), and the NY group (n = 20) using a computer-generated randomization method. The detailed trial profile is depicted in Figure 1.

CONSORT flowchart of the study. IAG, Integrated acupuncture group; SAG, Sham acupuncture group; NYG, Naturopathy and Yoga group.
Inclusion criteria
The study included both male and female participants of age between 30 and 60 who had been diagnosed with borderline or stage I hypertension. Patients with stage II or secondary hypertension, a history of coronary artery bypass graft (CABG) surgery, angina pectoris, psychotic medication, acupuncture treatment within the past 3 months, and pregnant or lactating women were excluded. This study adhered to the Consolidated Standards of Reporting Trials guideline.
Interventions
All the enrolled participants received standard yoga and naturopathy interventions for 10 days, irrespective of their medication status as an inpatient in the study setting. The detailed protocol of yoga and naturopathy interventions is outlined in (Supplementary Table). In addition to the yoga and naturopathy therapy, the participants from IA received 10 sittings of acupuncture therapy (30 min daily). Acupuncture sites were selected based on TCM principles after a comprehensive case history and pulse diagnosis. We punctured ST36 (the distal point), LIV2 (to relieve liver yang excess), LIV3 (the physiological hypotension point), KI3, HT7 (the Yuan source points for the kidney and heart), and SP9 (to control the function of the spleen). The detailed criteria on point selection are reported as per the Standards for Reporting Interventions in Clinical Trials of Acupuncture guidelines in Table 1.
Description of Treatment Regimen as per STRICTA Guidelines

The SA group received SA in addition to the yoga and naturopathy protocols. The SA included needling at (i) 1–2 cm below ST-36, (ii) a point on the forearm midway between the medial epicondyle of the humerus and wrist crease, and (iii) a point midway between the axilla and elbow on the medial side. The sham points were selected on the basis of previous studies, which suggests these are inert points.5,12 These points were needled for 10 days for 30 min daily, similar to the IA group. The NY group received yoga and naturopathy treatment alone, which was common in all three groups (Supplementary Table). All the participants were followed up for 1 month after the intervention, where they were advised to follow basic lifestyle modifications such as yoga, a low-sodium diet, proper sleep, and sun exposure.
Education of acupuncture practitioners
Acupuncture and SA was administered by licensed yoga and naturopathy physicians with a bachelor’s degree in yoga and naturopathy and more than 8 years of experience in acupuncture teaching and clinical practice.
Outcome Measures
A change in BP was considered the primary outcome measure. The BP was measured in the sitting position on the left hand using a digital sphygmomanometer (Omron HEM-7124, Gurgaon, India). The other secondary outcome measures included the following:
Quality of life (QoL): The SF-12, a 12-item quality of life instrument, was used to measure the changes in QoL of the participants, which assessed both the physical and mental health-related QoL. 13
Depression, anxiety, and stress scale (DASS)-21: A 21-item DASS-21 scale was used to measure the symptoms of stress, anxiety, and depression among the study participants. 14
Heart rate variability (HRV) indices: HRV indices are measured using a Digital Physiograph machine (Recorders Medicar Systems Pvt Limited, India). A Digital Physiograph machine measures HRV by recording and analyzing the time intervals between consecutive heartbeats, known as inter-beat intervals or R-R intervals. Electrodes are placed on the skin to detect the electrical activity of the heart. These electrodes are usually positioned according to standard ECG (electrocardiogram) placement guidelines. The machine captures the electrical signals produced by the heart, specifically focusing on the R-waves, which are the prominent upward spikes in the ECG waveform corresponding to ventricular depolarization.
We collected time-domain indices such as SDNN (standard deviation of NN intervals expressed in milliseconds), RMSSD (root mean square of successive RR interval differences in milliseconds), NN50 (successive RR intervals that differ by more than 50 milliseconds in milliseconds), and pNN50 (percentage of successive RR intervals that differ by more than 50 milliseconds in %) of HRV. The frequency domain measures included in the study were VLF power (relative power of very-low frequency band [0.0033–0.04 Hz] expressed in percent), LF power (relative power of low frequency band [0.04–0.15 Hz] expressed in percent), HF power (relative power of high frequency band [0.15–0.4 Hz] expressed in percent), and LF/HF (ratio of LF-to-HF power expressed in percent.
LF is influenced by both sympathetic and parasympathetic activity but mainly reflects baroreflex activity and can indicate sympathetic activity when considered with HF and the LF/HF ratio. HF is primarily associated with parasympathetic (vagal) activity and reflects respiratory sinus arrhythmia. VLF’s physiological mechanisms are less understood but involve factors like thermoregulation and the renin-angiotensin system, potentially reflecting some parasympathetic activity. RMSSD is a time-domain measure indicating short-term heart rate variability and is a reliable indicator of parasympathetic activity, commonly used to assess vagal tone. 15
Except for HRV indices, which were measured at the baseline (before intervention), and at day 10 (after intervention), all the other outcome measures were assessed at baseline, day 10 and after 1 month from the day of discharge.
Data Analysis
Statistical analysis of the data was performed using SPSS software version. Data were tested for normality using the Shapiro–Wilk test. The Kruskal–Wallis test was used to assess the effects of interventions on systolic and diastolic BP, depression score, anxiety score, stress score, SF-12 body score, and SF-12 mental score. An independent-samples median test was used to identify the effect of intervention on heart rate variability.
RESULTS
No adverse events were reported by participants in any of the three groups. Overall, the majority of participants in each group were in menopause, with a smaller proportion in active menstruation and very few in peri-menopause. The basic demographic details are presented in Table 2.
Baseline Demographic Characteristics of the Study Participants

HTN, Hypertension.
Effect on BP
All three groups exhibited a decrease in systolic BP after 10 days of intervention, although this reduction was not statistically significant (p = 0.303). However, there was a significant increase in systolic BP in all groups after 1 month of intervention (p = 0.041) compared with the levels observed at day 10. This increase was more pronounced in the SA group compared with the NY group and IA group.
Similarly, all three groups experienced a decrease in diastolic after 10 days of intervention, though this decrease was not statistically significant (p = 0.065). However, there was a significant increase in diastolic BP in all groups after 1 month of follow-up (p = 0.001) compared with the levels observed at day 10 of the intervention. This increase was more significant in the SA group compared with the IA group and NY group.
Effect on Depression, Anxiety, and Stress Scores
All three groups exhibited a visible decrease in depression scores following the 10-day intervention, though these reductions were not statistically significant (p = 0.776). At follow-up, both the NY group and the IA group showed an increase in depression scores, while the SA group demonstrated a reduction compared with day 10 scores, though not statistically significant.
Similarly, all three groups showed reductions in anxiety scores after the 10-day intervention, which were not statistically significant (p = 0.895). At follow-up, both the IA and SA groups showed further decreases in anxiety scores, while the NY group exhibited an increase compared with day 10 scores, though not statistically significant.
In terms of stress scores, all three groups experienced reductions after the 10-day intervention, none of which were statistically significant (p = 0.857). At follow-up, both the IA and SA groups demonstrated further decreases, while the NY group showed an increase. However, none of these changes reached statistical significance (p = 0.222).
Effect on SF 12 Physical and Mental Scores
All three groups demonstrated an increase in physical scores after the 10-day intervention, but this increase was not statistically significant (p = 0.063). However, by the end of the follow-up period, a reduction in physical scores was observed in all groups compared with the day 10 values, though the reduction was not significant (p = 0.140). Similarly, all three groups showed an increase in mental scores after the 10-day intervention, but this increase was not statistically significant (p = 0.585). By the end of the follow-up period, a reduction in mental scores was observed in all groups compared with the day 10 values, though the reduction was not significant (p = 0.140). The detailed results are tabulated in Table 3.
Table Outlining the Effect of Intervention on Outcome Variables Across the Three Groups
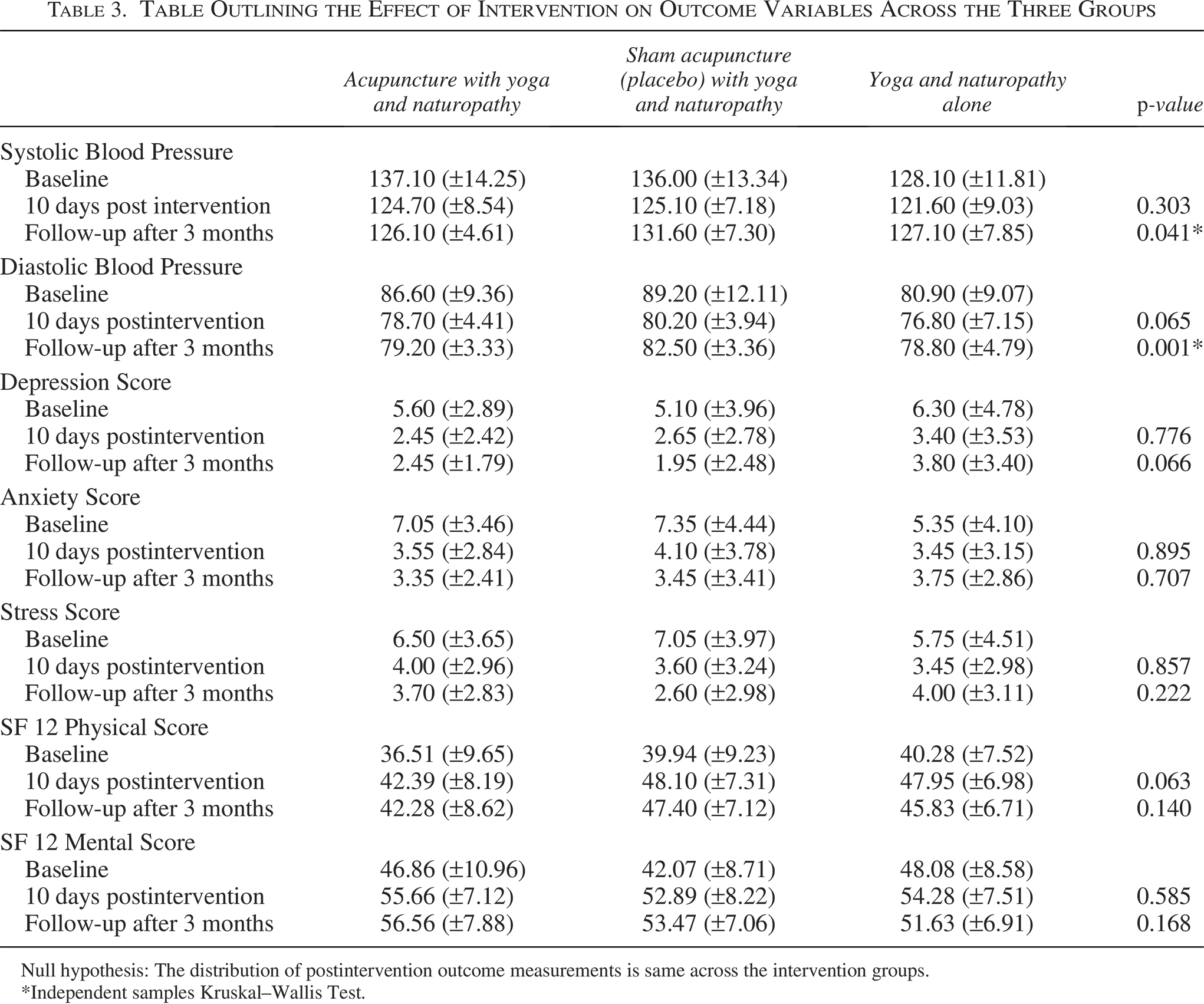
Null hypothesis: The distribution of postintervention outcome measurements is same across the intervention groups.
*Independent samples Kruskal–Wallis Test.
Effect on HRV
A significant increase in the SDNN values was observed in all the three groups (p = 0.041) at the end of 10 days of intervention. Significant reduction in LF/HF values was observed in the SA group and the NY group and statistically significant increase in the values was found in the IA group (p = 0.022) by the end of 10 days of intervention. Other parameters of HRV did not show any significant change during the study. The detailed results are tabulated in Table 4.
Effect of Intervention on Heart Rate Variability across the Three Groups
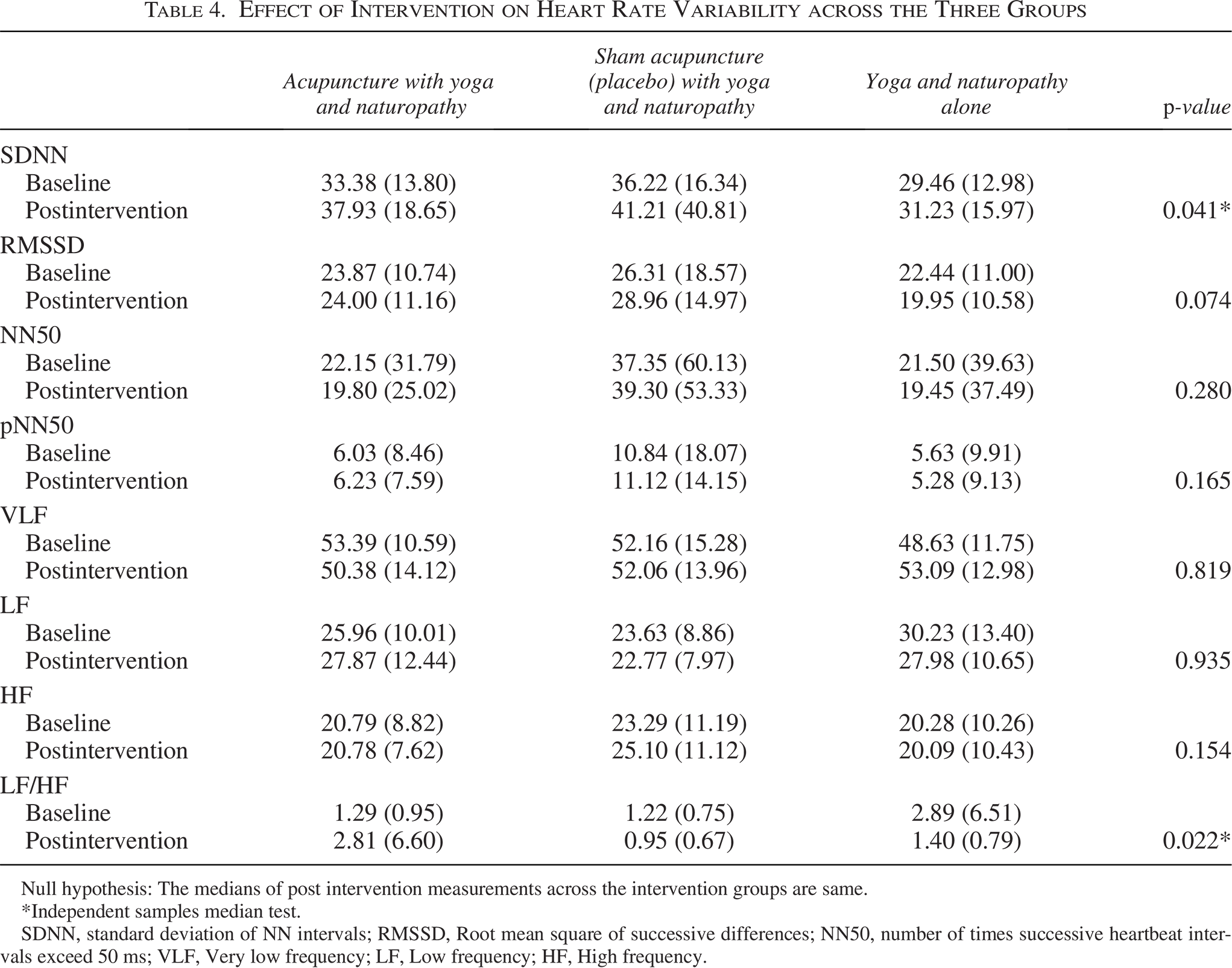
Null hypothesis: The medians of post intervention measurements across the intervention groups are same.
*Independent samples median test.
SDNN, standard deviation of NN intervals; RMSSD, Root mean square of successive differences; NN50, number of times successive heartbeat intervals exceed 50 ms; VLF, Very low frequency; LF, Low frequency; HF, High frequency.
DISCUSSION
This study investigated the role of acupuncture, as practiced in India, through a randomized controlled design consisting of three groups. Patients in the SA group were found to have been under pharmacotherapy for BP control for a longer period compared with the other groups, followed by the IA group and the NY group. The IA group had the highest percentage of medication tapering, followed by the SA and NY groups. This suggests that IA may play a superior role in managing hypertension and reducing the need for pharmacotherapy compared with other approaches. This finding is in agreement with an earlier systematic review, which suggests that acupuncture may be equally effective as antihypertensive medications. 11 Nevertheless, the limited sample size and shorter follow-up limit the conclusiveness of this inference.
The study reveals intriguing patterns in intervention effects on systolic and diastolic BP among the three groups. Initially, all groups showed reduced BP after the 10-day intervention, suggesting potential efficacy. However, these reductions were not statistically significant, indicating chance effects. Notably, after 1 month, there was a significant increase in BP across all groups, raising questions about intervention sustainability.
The disparity in BP changes between groups suggests intervention type may influence outcomes, emphasizing the need for tailored management strategies. The inconclusive role of acupuncture in reducing BP, as noted in a previous systematic review, 4 adds context to the findings of this study. This observation underscores the complexity of evaluating the effectiveness of acupuncture in clinical settings and highlights the need for further research to elucidate its true impact on BP regulation.
The study also investigated the role of IA in alleviating stress, anxiety, and depression among hypertensive participants. The observed trends in depression, anxiety, and stress scores among the three intervention groups provide valuable insights into the potential effects of naturopathy, yoga, and acupuncture on mental well-being. Despite the absence of statistically significant reductions, the visible decreases across all groups suggest some initial efficacy of the interventions in addressing these psychological outcomes.
However, upon follow-up, divergent trends emerged among the intervention groups, where a significant increase in mental health parameters was observed. Given the higher prevalence of mental health issues among patients with hypertension, 16 the findings of this study, although inconclusive, shed light on the possibility of using IA as a holistic intervention for mental health alleviation.
The study yielded notable findings regarding HRV parameters across the intervention groups. A significant increase in SDNN values was observed in all three groups at the end of the 10-day intervention period, indicating a positive effect on overall HRV. An increase in SDNN indicates superior cardiac function, better coping with stress, and heightened functional ability. 17 Furthermore, significant changes in LF/HF values were observed among the intervention groups. While the SA group and the NY group showed a significant reduction in LF/HF values, indicative of a shift towards parasympathetic dominance, the IA group exhibited a statistically significant increase in LF/HF values. This suggests a potential modulation of autonomic nervous system activity in response to the different interventions. Nevertheless, these findings are consistent with previous research demonstrating acupuncture’s modulation of LF/HF values. 18
Majority of the participants in this study (80%) were in menopause. This distribution is significant when considering the relationship between menopausal status and hypertension. 19 The predominance of menopausal participants across all groups suggests a potential underlying factor influencing BP changes observed during the intervention. The slight, nonsignificant reductions in BP after the 10-day intervention might be attributed to the short duration, which may not be sufficient to observe substantial cardiovascular benefits, particularly in a population already at higher risk due to menopausal status.
This study represents the first investigation into the role of IA practice, as conducted in India, on hypertension patients. While the trial could not definitively determine which of the three approaches—acupuncture integrated with NY, SA with NY, or NY alone—was most effective in addressing hypertension, it did identify some statistically nonsignificant benefits of all these three practices in improving BP, mental health indices, and HRV indices.
However, the findings from this study should be interpreted with caution due to substantial methodological limitations. Despite clinically meaningful changes observed in variables such as BP, mental health indices, and HRV, statistical significance was not achieved in the majority of the examined variables. The lack of statistical significance may be attributed to various factors, including the relatively short duration of the intervention and the sample size.
In addition, individual variability in response to the interventions could have contributed to the nonsignificant findings. Therefore, the results from this study can only be considered as preliminary evidence, warranting adequately powered, well-designed randomized controlled trials. Furthermore, it should be noted that a 10-day intervention plan may not be sufficient to fully ascertain the real impact of the interventions investigated in this study, positioning it more as a feasibility study. Nevertheless, this study provides insights into the immediate, short-term effects of the three different types of integrative medicine practices.
CONCLUSION
The findings of the present study suggest that acupuncture and NY combined or alone may play a role in modulating HRV, BP, and mental health among patients with hypertension. However, the methodological limitations in this study warrant further investigation in these domains.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No Interests to disclose.
FUNDING INFORMATION
No funding was received for this article.