
Abstract
Background:
Low anterior resection syndrome (LARS) comprises a series of bowel symptoms after low anterior resection for rectal cancer that seriously decrease the patients’ quality of life. Current treatments for LARS include antidiarrheal medications, pelvic floor muscle exercises, biofeedback training, and transanal irrigation, all of which lack high-quality supporting evidence or have low patient acceptance. Acupuncture has been found to have a therapeutic effect on LARS; however, further research is warranted because the available clinical studies have small sample sizes and different acupuncture treatment protocols and durations of treatment. This study is designed to investigate the effectiveness and safety of electroacupuncture in clinical settings.
Methods:
This is a multicenter, prospective, observational, comparative study of data obtained from a registry platform. Patients are classified into electroacupuncture and non-electroacupuncture exposure groups based on whether they receive electroacupuncture treatment or not, and the exposure dose is categorised in accordance with the timing and frequency of electroacupuncture treatment. The bowel function and quality of life will be compared between the two groups during a 6-month follow-up period. Propensity score matching and the inverse probability of weighting method will be used to reduce the risk of bias and control confounding factors.
Discussion:
This prospective, observational, comparative study aims to evaluate the effectiveness and safety of electroacupuncture at BL33, BL35, and SP6 in improving the defecation function of patients with LARS, and to explore the dose-response relationship of electroacupuncture and defecation function. The results of this study will provide support for further research.
INTRODUCTION
Low anterior resection syndrome (LARS) refers to a series of intestinal symptoms that develop after anterior resection for rectal cancer. 1 The incidence of severe LARS after anal sphincter-preserving surgery for rectal cancer is 44% (95% confidence interval 40%–48%). 2 The symptoms of LARS are most prominent in the early postoperative period and generally become stable after 1–2 years; 3 however, a considerable proportion of patients with LARS may have lifelong symptoms, which seriously decreases their quality of life. 4
Among the main treatments currently applied for LARS, medication and dietary modifications have limited effects. Pelvic floor rehabilitation, including muscle exercise techniques and biofeedback training, has been associated with improvements in LARS scores, 5 but requires adherence by the patient. Neuromodulation techniques have only been used to treat LARS in a few studies with small sample sizes. 5 Transanal irrigation, although effective in patients with constipation and incomplete evacuation, takes approximately 45 min to empty the irrigation solution in one sitting 6 and is not suitable for patients with faecal incontinence.
A few clinical studies have suggested that acupuncture may have a certain effect on LARS. Ren et al. 7 designed a randomized controlled trial with 30 patients in each group and found that acupuncture plus biofeedback therapy was superior to biofeedback therapy alone. Zhao et al. 8 designed a three-armed randomised controlled trial with 40 patients in each group and found that combined acupuncture plus biofeedback therapy plus levator ani muscle training was superior to acupuncture plus levator ani muscle training and levator ani muscle training alone. In addition, several small-sample, single-arm studies have suggested that acupuncture plays a role in relieving the symptoms of LARS.9–11 However, the existing clinical studies have used different acupoints and durations of treatment.
OBJECTIVES
The purpose of this study is to compile data from the perspective of improving defecation function in LARS patients after anal preservation surgery for rectal cancer. Thus, to observe the effectiveness and safety of electroacupuncture in treating LARS, and to explore the dose-response relationship of electroacupuncture exposure and defecation function.
STUDY DESIGN
This study protocol is written in accordance with the STROBE guidelines. This is a prospective, multicentre, longitudinal, observational, cohort study that is being carried out with the help of the International Acupuncture Case Registration Platform.
SETTING
The study is being conducted at the Institute of Basic Research in Clinical Medicine, China Academy of Chinese Medical Sciences, Guang’anmen Hospital of China Academy of Traditional Chinese Medicine, Cancer Hospital of the Chinese Academy of Medical Sciences, Beijing Hospital of Traditional Chinese Medicine, and Wang Jing Hospital of the CACMS.
The study cohort comprises patients with LARS after sphincter-preserving surgery for rectal cancer and without protective ileostomy. The patients’ characteristics, treatments, and outcome indicators are recorded during a 6-month follow-up period. The first patient was enrolled on 22nd December 2023. The expected recruitment deadline is 31st December 2026. Patients are divided into the basic treatment group (non-electroacupuncture group) and the electroacupuncture plus basic treatment group (electroacupuncture group) in accordance with whether they receive electroacupuncture treatment or not. The improvement in defecation function, improvement in quality of life, and safety of the treatment will be compared between the two groups.
PARTICIPANTS
Diagnostic Criteria
The diagnostic criteria for inclusion in this study are in accordance with the international consensus 1 in which LARS is defined as having at least one of the following eight symptoms after rectal resection with the anal sphincter preserved: variable, unpredictable bowel function; altered stool consistency; increased stool frequency; repeated painful stools; emptying difficulties; urgency; incontinence; soiling. Results in at least one of these consequences: toileting dependence; preoccupation with bowel function; bowel dissatisfaction; strategies and compromises made to adjust to changes; impact on mental and emotional well-being; impact on social and daily activities; impact on relationships, and intimacy; impact on roles, commitments, and responsibilities. LARS is suspected if a patient develops at least one of these bowel symptoms after undergoing anterior rectal resection, and the diagnosis is confirmed if the evaluation fails to reveal other aetiologies.
Inclusion Criteria
Pathologic diagnosis of rectal cancer after anterior resection and without preventive ostomy.
Age 18–75 years.
Compliance with the LARS diagnosis and a LARS scale score of ≥21 points.
Expected survival time of ≥6 months.
Provision of written informed consent.
Exclusion Criteria
Abnormal defecation caused by drugs, infections, or other diseases (e.g., irritable bowel syndrome, radiation enteritis, and central nervous system injury).
Coagulation dysfunction or severe systemic disease.
Concomitant anastomotic stenosis, anastomotic leakage, anastomotic bleeding, intestinal perforation, and other postoperative complications or local tumour recurrence. Multiple primary bowel cancers or those who have received neoadjuvant therapy.
Intellectual disability or psychiatric history that renders the patient unable to cooperate.
Participation in another clinical trial.
Loss to Follow-up
Participants who fail to complete the follow-up visits will be recorded as lost to follow-up.
Sources and Methods of Patient Selection
Participant screening is being implemented in outpatient or inpatient settings by clinical oncological specialists with at least 2 years of independent outpatient experience. Patients are being recruited through hospital posters and online posters.
VARIABLES
Outcomes
Primary outcomes
Proportion of patients with reduced defecation dysfunction as judged by the LARS score after 1 month of follow-up (LARS scale scores of 21–29 are considered to indicate mild disease, while scores of 30–42 are considered to indicate severe disease).
Proportion of reductions from baseline in the average daily number of bowel movements based on a 3-day stool diary (assessed after 1 month of follow-up).
Secondary outcomes
Course of treatment required for treatment to be effective (i.e., for the LARS score assessment to change from severe to mild, or from mild to normal).
Between-group comparisons of the changes from baseline values in the LARS scores at 1, 3, and 6 months after enrolment.
Between-group comparison of the changes in the Faecal Incontinence Patients’ Quality of Life Scale (FIQL) from baseline to 1, 3, and 6 months after enrolment.
Comparison between the two groups in the number of bowel movements per day (assessed each day after enrolment for 1 month).
Value of the changes from baseline in the mean visual analogue scale (VAS) score per bowel movement based on a 3-day stool diary (assessed at 1 month after enrolment).
Change from baseline in the mean urgency level of each bowel movement score based on a 3-day stool diary (assessed at 1 month after enrolment).
Change from baseline in the percentage of missed stools based on the 3-day stool diary (assessed at 1 month after enrolment).
Blood counts, tumour marker concentrations, and local recurrence rate during treatment and follow-up.
Safety evaluation based on the incidence of adverse events or treatment-related adverse reactions during the study period.
Exposures
The patients are divided into the exposure (electroacupuncture) and control (non-electroacupuncture) groups. Participants are enrolled and assigned to receive treatments by clinical doctors based on each patient’s condition and personal choice. The exposure dose of electroacupuncture is defined according to the total number of acupuncture sessions within 1 month as: low (≤4 sessions), medium (5–8 sessions), or high (≥9 sessions).
The electroacupuncture points are bilateral BL33, BL35, and SP6. The acupoints are routinely sterilized. BL33 is located about 1 cm outside and above the third post-sacral foramen, and a 0.30 mm × 75 mm or 0.35 mm × 75 mm needle is inserted obliquely inward at an angle of about 60–75 degrees downward toward the third post-sacral foramen to a depth of about 70 mm. At BL35, a 0.30 mm × 75 mm needle is inserted perpendicular to the skin to a depth of about 60–70 mm. At SP6, a 0.30 mm × 40 mm needle is inserted perpendicular to the skin to a depth of about 25–30 mm (observation of flexion of the patient’s big toe or the patient’s report of sensory stimulation of the sole of the foot). The bilateral BL33 and BL35 points are connected to one set of electrodes with a current frequency of 10 Hz in a continuous wave for 20 min each time; the stimulation intensity ranges from 3 to 6.5 mA and will be set as high as tolerated by the patient. Electroacupuncture treatment is scheduled to be performed three to five times in the first week, and two to three times per week in the second to fourth weeks.
Potential Confounders
The treatment methods that may be used in the study are listed below. The dietary guidelines and pelvic floor muscle training instructions are printed on a take-home note for each patient.
Dietary guidance: patients are instructed to avoid spicy and stimulating foods that produce gas (e.g., onions and soya beans) and to avoid drinking wine. Patients with constipation and defecation urgency can supplement their dietary fibre appropriately. Pelvic floor muscle training: patients are instructed to do Kegel exercises for pelvic floor muscle training for 15–20 min per day. This involves repeatedly alternating between tightening the pelvic floor muscles for 5–10 sec and then relaxing the pelvic floor muscles for 10 sec. Patients may take antidiarrheal agents such as lamosetron, loperamide, or colesevelam hydrochloride. Combined treatments: patients who need chemotherapy during the treatment period will receive electroacupuncture treatment during the chemotherapy period and record the chemotherapy regimen. Patients must stop electroacupuncture during radiotherapy but continue to attend follow-up visits at each scheduled timepoint. If other diseases (e.g. influenza and diarrhea) occur suddenly during the treatment and other drugs need to be added, these should be used under the guidance of a doctor.
DATA COLLECTION AND MEASUREMENT
Patient Information
The general data collected by the clinician at baseline are as follows: sex, date of birth, height, weight, ethnicity, and medical history (e.g., diabetes mellitus, hypertension, and coronary artery disease), family history, allergy history, oncological history (TNM stage of the tumor), pathological type of rectal cancer, surgical procedure, the location of the primary tumor from the anal margin, whether the patient is currently receiving chemotherapy or radiotherapy, and traditional Chinese medicine diagnosis including tongue and pulse assessments.
Therapeutic Measures
The patients are asked to report the use of LARS-related interventions, such as dietary modifications and the frequency and duration of Kegel exercises. The attending clinician searches the medical records at baseline and at 1, 3, and 6 months after enrolment to identify the dates on which electroacupuncture was performed and any prescribed medicines.
Treatment of Comorbidities
The name, dose, frequency, and start and end dates of treatments are recorded for any comorbidities and all treatment modalities (e.g., chemotherapy and oral medications) received by the patient during the observation period. These data will be derived from the medical records at baseline and at 1, 3, and 6 months after enrolment.
Bowel Function
The LARS-specific scale 12 targets the five most important clinical symptoms, namely urgency, frequency, clustering, incontinence for flatus, and incontinence for liquid stools. The maximum score is 42. The LARS scale is reported by the patient at each follow-up timepoint: baseline and 1, 3, and 6 months after enrolment.
The defecation characteristics are evaluated using the Bristol stool classification (1–7 points) and recorded in a stool diary. 13 The urgency of defecation is recorded as 0 (no urgency), 1 (slight urgency), 2 (moderate urgency), 3 (strong urgency), or 4 (strong urgency with stool leakage). The pain associated with defecation is recorded using the VAS score as 0 (no pain), 1–3 (mild pain), 4–6 (moderate pain), 7–10 (severe pain), or 10 (unbearable pain). The patients record these indicators of bowel function daily for 1 month from the date of enrolment.
Quality of Life
The quality of life is measured using the FIQL, which consists of 29 questions in four areas: lifestyle changes, coping/behavioral limitations, frustration/self-perception, and social embarrassment. 14 The Chinese version of the FIQL has good reliability and validity. 15 The FIQL is reported by the patient at each follow-up timepoint: baseline and 1, 3, and 6 months after enrolment.
Tumor-Related Prognosis
Routine blood tests results, blood biochemical test results, concentrations of tumor markers (carcinoembryonic antigen and glycan antigen), and the local recurrence rate are recorded at baseline and 3 and 6 months after enrolment.
BIAS
To reduce bias, we formulated a study manual and standard operating procedure for each process. All researchers will receive training regarding the study protocol, use of the data platform, electroacupuncture operation, and handling and recording of adverse events. All researchers will have the necessary qualifications and experience to conduct the research operations in accordance with the regulations.
SAMPLE SIZE
Our sample size calculations are based on a previous study in which the electroacupuncture group comprised 6 patients with mild LARS and 19 patients with severe LARS before treatment. 16 After 4 weeks, the LARS score was normal in 11 patients, mild in 10 patients, and severe in 4 patients. 16 The LARS score reduction rate after 4 weeks of treatment was 60%–84% in the electroacupuncture group and 20%–40% in the non-electroacupuncture group. 16 Combined with the previous clinical observations of the research group, it is conservatively estimated that the disease reduction rate in the present study will be 56% in the electroacupuncture group and 33% in the non-electroacupuncture group. The required sample size estimated using the PASS software Rate of Two Independent Samples Tests for Two Proportions with a 1:1 ratio in the two groups, unilateral α = 0.025, and 1-β = 0.80, was a total of 140 participants. Assuming a 15% loss-to-follow-up rate, the actual sample size should be no less than 164 participants.
STATISTICAL METHODS FOR ASSESSING PRIMARY AND SECONDARY OUTCOMES
Continuous variables conforming to normal distribution will be shown as the mean ± standard deviation, while non-normally distributed continuous variables will be expressed as the median and interquartile range. Data normality will be judged using the Shapiro-Wilk test and QQ plots. Categorical data will be expressed as percentages. Differences in baseline data between the two groups will be compared using the two independent samples t-test, rank sum test, or chi-squared test.
Propensity score matching and the inverse probability of weighting method will be used to equalize multiple confounders in the treatment and control groups without changing the sample size. Logistic regression will be used to compare the incidence of the primary outcome between the electroacupuncture and non-electroacupuncture groups. Between-group comparisons of the proportions of patients with a reduction in the disease severity at follow-up timepoints and changes from the baseline FIQL and LARS scores will be analyzed using repeated-measures analysis of variance, and the effect of electroacupuncture will be estimated using the generalized estimating equation. Between-group comparisons of the changes from baseline in the measures recorded in the 3-day stool diary in the two groups at 1 month after enrolment will be made using the two-independent-samples t-test or rank-sum test, with the electroacupuncture effect estimated by multiple linear regression. Categorical variables will be evaluated using the chi-squared test and included in the ordered multicategorical regression model for effect estimation. A mixed-effects model will be constructed to plot the exposure-response relationship between the number of electroacupuncture treatments and the daily number of defecations; the timepoint of measurement, number of treatments, and confounding factors will be used as fixed variables, the study center and individual differences will be used as random factors, and the average daily defecation data recorded in the stool diary will be used as the dependent variable.
All data analyses and model building will be processed using R 4.2.1, SPSS 20 software, with p < 0.05 taken to denote a significant difference. Subgroup analyses will be constructed separately by stratifying the analysis in accordance with the LARS severity, whether radiotherapy is administered during follow-up, distance from the surgical anastomosis to the anal verge, and tumor stage.
The full analysis set will be evaluated. The data of participants who are enrolled and complete at least one follow-up will be included in the statistical analysis, even if the participants withdraw from the trial due to adverse reactions in the later stage and only experience part of the trial process. Missing data will be filled in by multiple imputation or by carry-over of last observations.
FREQUENCY AND PLANS FOR AUDITING RESEARCH CONDUCT
There will be three-level quality control during the research. A quality control group within the research group will conduct self-inspection, the grant holding institution will carry out supervision, and the project sponsor will set up a team of experts to conduct quality inspection.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval has been obtained from the Institute of Basic Research in Clinical Medicine, China Academy of Chinese Medical Sciences Ethics (P23012/PJ12, P24022-PJ22). All modifications will be reported to the ethical committee. Findings will be: (1) reported to funding sources, institutions, and hospitals supporting the study; (2) presented at local, national, and international conferences; and (3) disseminated in peer-reviewed publications. Written, informed consent to participate will be obtained from all participants.
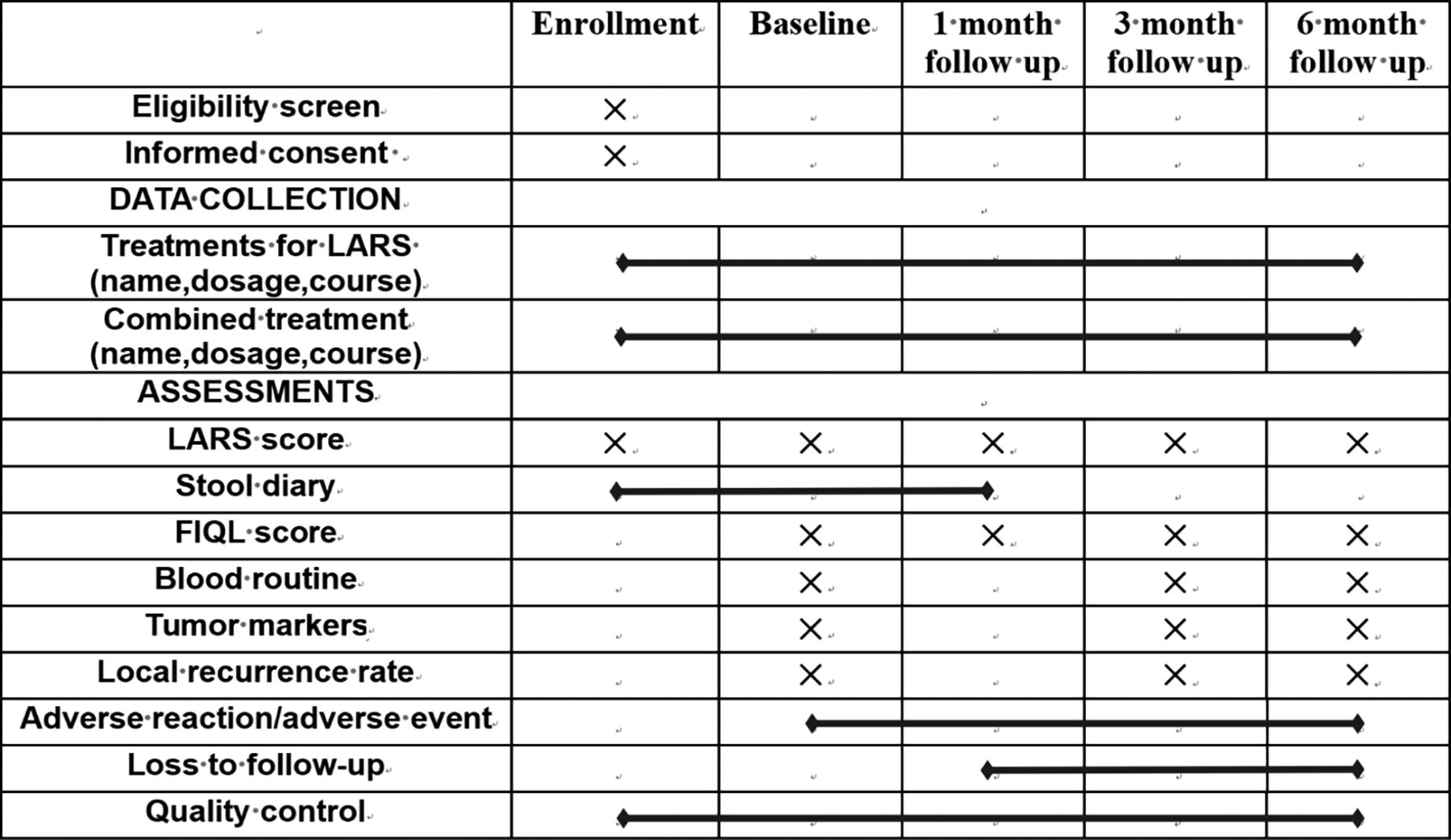
PARTICIPANT TIMELINE
DISCUSSION
Previous studies have shown the efficacy of acupuncture in treating pelvic floor disorders and gastrointestinal disorders.17–19 In contrast, fewer studies have focused on the possible role of acupuncture in treating LARS. The two common situations in anorectal-preserving surgery for low rectal cancer are simple anastomosis or concurrent prophylactic stoma creation (after which the surgeon waits for the anastomosis to heal and then performs stoma reduction surgery). Prophylactic stoma creation may reduce the risk of postoperative anastomotic leakage/fistula, but is more likely to result in LARS due to colonic atrophy. Nutritional deficiencies can affect the intestinal plexus and lead to dysbiosis of the colonic ecology or epithelial changes in the terminal ileum itself. 20 Considering the different pathogenesis of these two situations, only patients with LARS who did not have a protective stoma created intraoperatively are being included in the proposed study. A prospective cohort study will be performed to evaluate the effectiveness, advantages, and safety of electroacupuncture in real-world scenarios. Although randomisation and blinding are not being performed in this proposed study, propensity score matching and the inverse probability of weighting method will be used to reduce the risk of bias and control confounding factors.
AUTHORS’ CONTRIBUTIONS
J.L., H.C.: Conceptualization. J.L.: Funding acquisition. J.L., H.C., J.X., F.W., Y.L.: Resources. J.L., H.C., L.H.: Supervision. M.W., H.L.: Project administration. M.W.: Writing—original draft. H.L., W.H.: Writing—review and editing. X.C., X.W., W.H.: Investigation.
Footnotes
ACKNOWLEDGMENTS
The authors thank Kelly Zammit, BVSc, from Liwen Bianji (Edanz) (www.liwenbianji.cn/), for editing the English text of a draft of this article.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
This research was funded by Capital’s Funds for Health Improvement and Research (NO.2024-2-4301) and Innovative Engineering Project of China Academy Of Chinese Medical Sciences, Case Registration Study on Real World Efficacy Evaluation of Traditional Chinese Medicine (CI2021A05408). The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the article; or in the decision to publish the results.