
Abstract
Background:
Acupuncture is a popular modality for treating shoulder pain and dysfunction. However, its reproducibility in shoulder-related clinical studies has been inconsistent. Several discrepancies were found between the systematic classical (Jia Yi Jing [JYJ]) and a modern standardized acupuncture text for the location of points on the shoulder girdle.
Objective:
To define the neuroanatomical target of acupoint with respect to the shoulder girdle.
Methods:
Transliteration of the location of shoulder girdle-related acupuncture points from the JYJ. Point locations from the JYJ were compared to the textbook Chinese Acupuncture and Moxibustion. A review of surgical literature, cadaver dissection, and response from electrical stimulation on healthy volunteers was used to propose new neuroanatomical targets for each acupuncture point.
Results:
Acupuncture points of the shoulder girdle corresponded to the following: dorsal scapular, spinal accessory, long thoracic, thoraco-dorsal, suprascapular, axillary, and pectoral nerves.
Conclusions:
The present research verified the relationship between acupuncture points of the shoulder girdle and their corresponding neuroanatomical targets. This information increases the precision of acupuncture point stimulation and aids in the standardization of acupuncture point locations. It is expected to improve the interpretation of acupuncture studies on shoulder rehabilitation and future research design.
INTRODUCTION
Shoulder pain is a prevailing source of pain, affecting an estimated 27% of the population in the United States. 1 Current treatment of shoulder pain includes physical therapy, resting, icing, activity modification, acupuncture, and cortical-steroid injections. 2 A systematic review of the impact of cortical steroids on rotator cuff tendons health and repair found that the cortical steroids impede the healing process on a molecular level while decreasing the strength and flexibility of the tendons from a biomechanical level. 3
A meta-analysis of different treatments for shoulder impingement revealed that combining nonsurgical methods (i.e., acupuncture with exercises) yielded better results than individualized treatment alone, particularly in early stages of shoulder impingement syndrome. 4 Indeed, acupuncture has been a popular modality and treatment option for a variety of shoulder conditions. However, despite its popularity, the efficacy of acupuncture has yielded mixed results over the years. This lack of clinical consistency may be explained by historical emphasis on energetic point function passed down from classical texts, as opposed to specific anatomical targets for each acupuncture point. This lack of precision in acupuncture point location yielded mixed results in clinical trials. 5
The purpose of this study is to standardize the neuroanatomical targets of specific acupuncture points on the shoulder girdle in order to increase the reproducibility of acupuncture. The current study utilizes literature reviews, cadaver dissection, and electrostimulation to verify neuroanatomical targets of these points. With a clear understanding of the precise neuroanatomical targets, the authors suggest that electroacupuncture can be used in the treatment of common shoulder conditions by neuromodulating associated nerves to restore proper scapulothoracic and glenohumeral rhythms.
METHODS
Literature Review
The Systematic Classics (Jia Yi Jing [JYJ]) is regarded as the first complete acupuncture and moxibustion manual dating back to the third century. 6 Acupuncture points associated with the shoulder girdle were compared between the JYJ and the modern traditional Chinese medicine textbook Chinese Acupuncture and Moxibustion (CAM). Any discrepancies in point locations between JYJ and CAM were noted. Anatomical targets for shoulder girdle acupuncture points were determined and updated based on peer-reviewed surgical dissection literature.
Dissection
A single soft embalmed cadaver of an 82-year-old male was used to demonstrate the neuroanatomical structures and relevance of the chosen acupuncture points. The cadaver was fixed with vascular perfusion using a mixture of liquid phenol, 95% ethanol, glycerin, and water.
The cadaver was bequeathed to the University of Toronto through the Department of Anatomy and Surgery. Bioethics approval was obtained through the Human Research Ethics Program (#32018). Dissection was performed between 2015 and 2016.
Electrostimulation
Electrostimulation was performed to verify the neuroanatomical target proposed for each acupuncture point examined in the present study. Ten healthy acupuncturists provided written consent to become volunteers for electrostimulation during a continuing education workshop setting. Electrostimulation was conducted on needles inserted into acupuncture points using Pointer Plus (10 Hz monopolar electrostimulation device produced by Mayfair Medical Supplies, Hong Kong). The size of the needles used was 0.30 × 50 mm. The electrical stimulation was applied to each point at 10 Hz, with the duration of 1 s burst, for a total of five bursts. The elicited sensory and/or motor responses were compared to established reactions of the proposed neuroanatomical target.
RESULTS
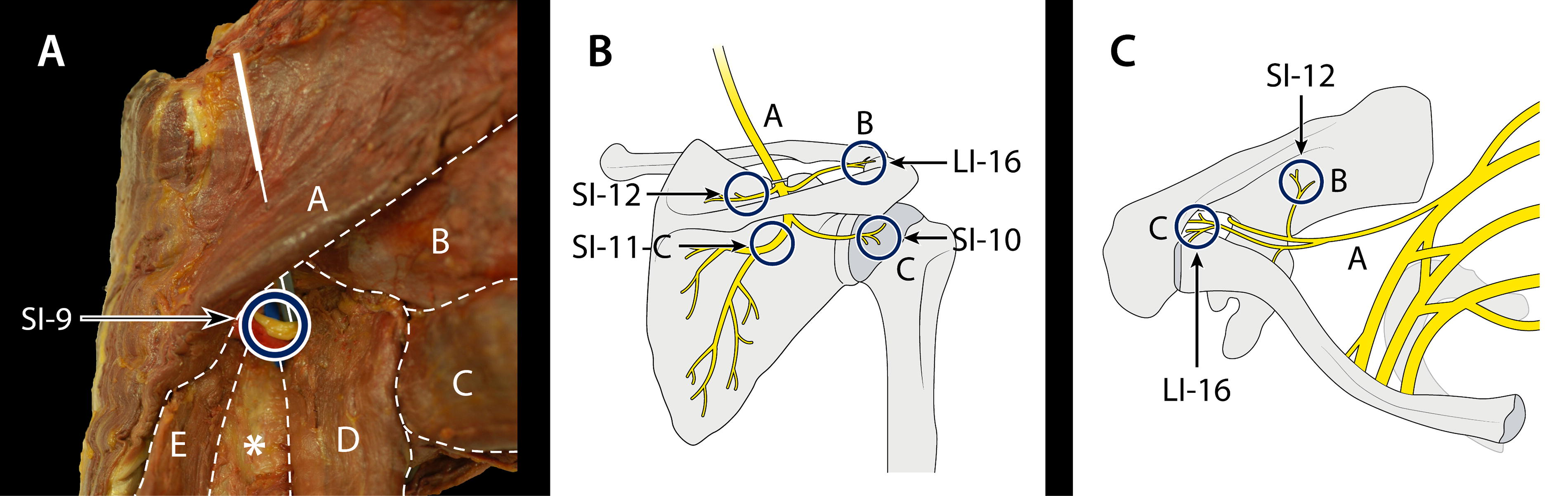
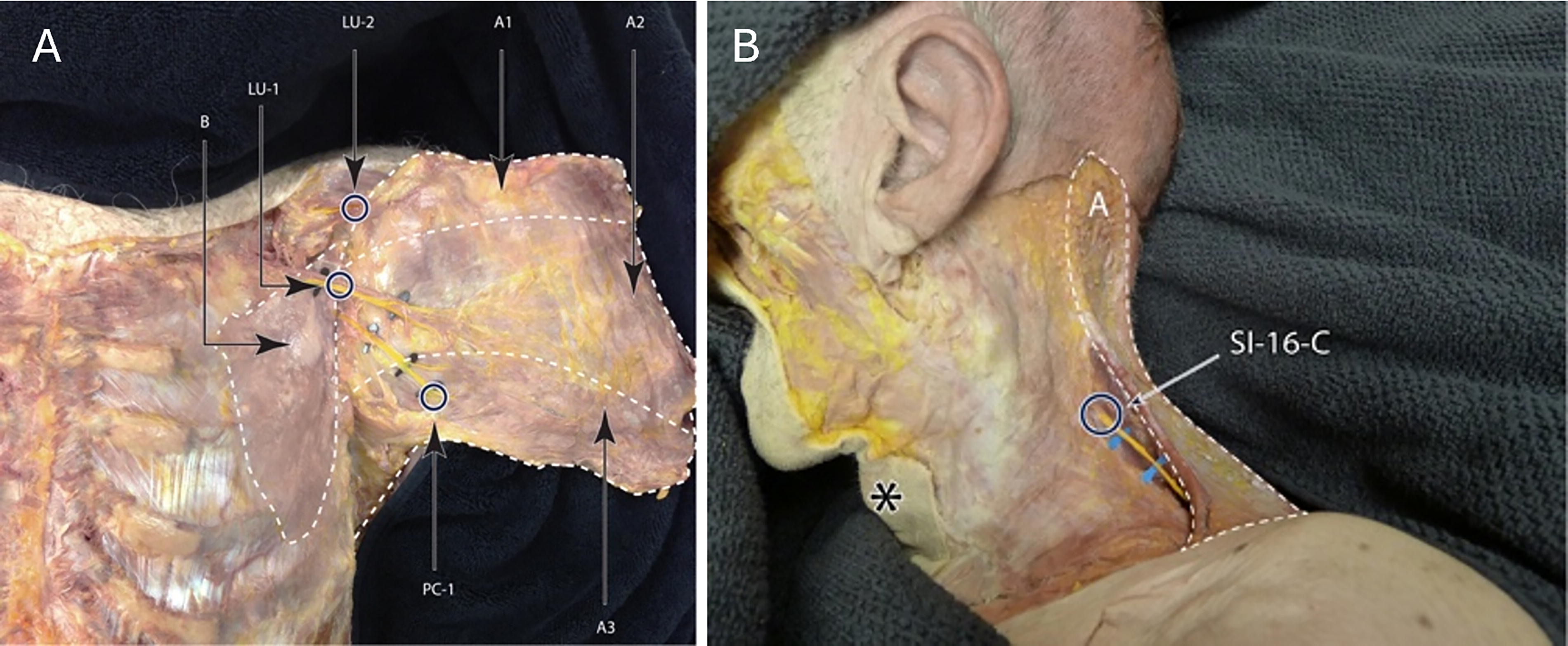
The authors identified inconsistencies of acupuncture point location between the JYJ and CAM. Acupuncture point descriptions provided by the JYJ were transliterated and reinterpreted based on relevant neuroanatomical structures. Some of the reinterpreted structures and point location differ from the modern text, in turn, the point location and its intended neuroanatomical target may be misinterpreted as presented in Table 1. A visual representation of the neuroanatomical targets of the specific acupuncture points of the posterior, superior view of the scapular, and the lateral thoracic wall can be seen in Figures 1 and 2. Figure 3 illustrates acupuncture points of the anterior chest wall and the lateral view of the neck. Supplementary Videos S1, S2, S3 and S4 demonstrate electrical stimulation of acupuncture points, to obtain the expected activation of shoulder girdle muscles based on their respective innervation.
Comparison of Classical (Jia Yin Jing vs. Contemporary Chinese Acupuncture and Moxibustion) Point Location and Relevant Anatomy of the Shoulder Girdle
SI 11-C, SI 16-C, and SI 13-C refer to classical point locations described in JYJ texts, which differ from modern locations in CAM.
CAM, Chinese Acupuncture and Moxibustion; JYJ, M Jia Yi Jing.

DISCUSSION
Suprascapular Nerve
CAM describes SI-12 to be located in the center of the suprascapular fossa directly above SI-11 when the arm is lifted. 7 The contemporary terminology in place of suprascapular fossa is supraspinous fossa. From the SI-12 location described in the JYJ, the authors interpret the small bone landmark to be the superior angle of the scapula. Therefore, the location behind the small bone where a hollow is felt when the arm is raised (interpreted as abduction) would be located within the supraspinous fossa. Thus, the authors propose that the intended neuroanatomical target for SI-12 is the supraspinatus branch of the suprascapular nerve.
CAM provides information on both superficial and deep innervations on SI-12. 7 Although the present authors agree with the deep innervation attributed to the suprascapular nerve, the superficial innervation attributed to the lateral suprascapular nerve and accessory nerve is inaccurate. The suprascapular nerve is not characterized as having lateral branches, only supraspinatus, infraspinatus, and articular branches. The assignment of accessory nerve to SI-12 is also problematic. The spinal accessory nerve (SAN) is located anteriorly to the transverse process at the level of the atlas. 8 It then traverses distally crossing the posterior belly of the digastric muscles. 8 The SAN then penetrates and perforates the sternocleidomastoid (SCM) before exiting the posterior border of the SCM to innervate the anterior border of the trapezius. 8 The trapezius attaches to the spine of the scapula and overlays the supraspinous fossa where SI-12 is located. However, stimulation of the SAN occurs only indirectly through innervation of the trapezius muscle fibers. Therefore, the SAN itself does not traverse into the supraspinous fossa. Hence, it is strongly recommended that the SAN should not be considered a target of SI-12.
CAM describes SI-11 to be on the scapula, in the depression of the center of the subscapular fossa at the level of the fourth thoracic vertebrae. The intended anatomical target would be the belly of the infraspinatus muscle. 7 The description of subscapular fossa is likely to be a translation error, as it is located on the anterior surface of the scapula where the subscapularis muscle is attached. The correct anatomical description would be the infraspinous fossa of the scapula, rather than the subscapular fossa. When the location of SI-11 is compared between CAM and the JYJ, the JYJ excludes longitudinal coordinates such as vertebral levels. Instead, the JYJ describes SI-11 to be behind the big bone. It is the author’s opinion that the big bone described in the JYJ location of SI-11-C is in fact the spine of the scapula. Since no precise longitudinal measurements were given to locate the point relative to the spine of the scapula, the implication is that SI-11-C is located right below the big bone (spine of the scapula).
An anatomical study of the suprascapular nerve described the pathway of the suprascapular nerve to pass through the scapular notch and inferior to the transverse scapular ligament. 9 From there, the suprascapular nerve heads to the base of the scapular spine and curves medially innervating the infraspinatus muscle within 1 cm below the scapular spine.9,10 This pathway, therefore, verifies the big bone described in the JYJ as the scapular spine and the intended neurovascular target for SI-11-C to be the infraspinatus branch of the suprascapular nerve and artery. Electrostimulation applied to the infraspinatus branch of the suprascapular nerve (SI-11-C) produced external rotation of the glenohumeral joint. See Supplementary Video S1.
Dorsal Scapular Nerve
CAM describes the location of SI-13 to be on the medial extremity of the suprascapular fossa, midway between SI-10 and the spinous process of the second thoracic vertebrae. 7 CAM describes the innervation for SI-13 to be a mix of the SAN, a muscular branch of the suprascapular nerve, and a branch of the posterior rami of the second vertebrae.
There is a discrepancy between the point location for SI-13 given by CAM and the location given by the JYJ. According to the JYJ, SI-13-C is located by the center of the bend where a pulsating vessel could be felt. The lack of neurovascular structures that could produce a pulsation on the medial part of the suprascapular/supraspinous fossa suggests that the point may be located off the medial/vertebral border of the scapula instead of being within the supraspinous fossa.
A surgical study of the dorsal scapular nerve indicated that the dorsal scapular nerve originates from the C5 spinal nerve trunk, passing through the middle scalene before traversing posteriorly toward the posterior scalene and serratus posterior superior muscle, innervating the levator scapula and the rhomboid major and minor.11,12 The dorsal scapular nerve was located at an average distance of 1.5 cm medial to the vertebral border of the scapula, where it runs parallel to the dorsal scapular artery along the anterior border of the rhomboid muscles. 11
Considering the literature and the cadaver dissection, it is the present authors’ opinion that the reference to the “middle of the bend” in the JYJ refers to the location where the superior angle meets the medial border of the scapula, and the pulsating vessel refers to the dorsal scapular artery. Thus, the intended neuroanatomical target of SI-13-C is the dorsal scapular neurovascular bundle. This was verified with the use of electric stimulation of the dorsal scapular nerve (SI-13-C), which elicited elevation and retraction of the scapula. See Supplementary Video S2.
Spinal Accessory Nerve
The SI-16 location was described by CAM to be located at the lateral aspect of the neck, posterior to the SCM and Fu Tu (LI-18), on the level of the laryngeal protuberance. 7 The JYJ description of SI-16-C mentions a pulsating vessel as part of its localization instruction that is missing in CAM. It is the authors’ opinion that the pulsating vessel refers to the superficial branch of the transverse cervical artery, which vascularizes the trapezius muscle together with the SAN that innervates the muscle.13,14
The SAN is described to be divided into internal and external branches, with the latter innervating the SCM and trapezius muscles. 15 The external branch travels along the transverse process of the atlas before traveling past the stylohyoid and digastric muscles. 15 The SAN then pierces through the SCM in an anterior-to-posterior direction. As it travels past the posterior cervical triangle, the SAN runs superficially before innervating the trapezius muscle. 15
The cadaver dissection conducted by the present authors illustrates that SI-16-C corresponds to where the SAN enters the anterior border of the trapezius muscle. It is here where the SAN lies superficially before piercing the trapezius muscle. 15 Electrostimulation of the SAN (SI-16-C) elicited elevation, retraction, and depression of the scapula, as shown in Supplementary Video S3.
Pectoral Nerves
Conventional anatomical textbooks divide the pectoral nerve into medial and lateral components.16–18 The medial pectoral nerve innervates the lower aspect of the pectoralis major and pectoralis minor, while the lateral pectoral nerve innervates supplies the upper two-thirds of the pectoralis major muscle.17,18 One dissection study demonstrated that all specimens presented three distinct branches of the pectoral nerve, thereby recommending that the terminology be changed to superior, middle, and inferior pectoral nerves. 16 This group found that the superior and middle pectoral nerves were derived from the lateral pectoral nerve, while the inferior pectoral nerve was equivalent to the medial pectoral nerve. 16 It is the present authors’ finding that these three pectoral nerve branches precisely match LU-2, LU-1, and PC-1, respectively.
The acupuncture point LU-2 was described by CAM to be in the superior lateral part of the anterior thoracic wall, superior to the coracoid process of the scapula, and in the depression of the infraclavicular fossa, 6 cun lateral to the anterior midline. 7 Based on this description, one can infer that the LU-2 is located within the deltopectoral triangle. The classical description of LU-2 is below the great bone, 2 cun beside Qi Hu (ST-13), where a pulsating vessel can be felt, obtained with the arm raised. 7 JYJ emphasizes the need to raise the patient’s arm to facilitate locating LU-2. It is the authors’ opinion that raising the arm with shoulder in flexion accentuates the deltopectoral triangle, which reflects the anatomical borders described above.
The great bone reference in the JYJ corresponds to the clavicle. The subclavian artery travels between the anterior and middle scalene muscles, traversing underneath the clavicle until the lateral border of the first rib where it becomes the axillary artery. 19 Due to the proximity of the axillary artery within the deltopectoral triangle, the pulsation referenced by the JYJ is likely to be the axillary artery. The superior branch of the pectoral nerve arises from the anterior division of the superior trunk at the level of C5-C6. 16 It appears at the inferior border of the clavicle and lateral to the axillary artery.16,18 It then travels straight to innervate the clavicular aspect of the pectoralis major muscle.16,18 Dissection of this area revealed that the path of the superior branch of the pectoral nerve precisely matches the location of LU-2.
According to the JYJ, the location of LU-1 is 2 cun below LU-2, in the depression three ribs space above the nipple, where a pulsating vessel can be felt. 7 It is the authors’ opinion that LU-1 represents the middle branch of the pectoral nerve, which is responsible for innervating the sternal fibers of the pectoralis major.16–18 The pulsating vessel likely refers to the axillary artery. 19 The middle branch of the pectoral nerve crosses the axillary artery and enters through the coracoclavicular fascia. 16 The nerve then moves deep to the pectoralis major, where it runs in close proximity to the branch of the thoracoacromial artery before innervating the sternal aspect of the pectoralis major. 17 The dissection conducted by the present authors traced the course of the middle pectoral nerve to LU-1.
CAM describes PC-1 to be located on the fourth intercostal space, 1 cun lateral to the nipple and 5 cun lateral to the anterior midline. 7 The inferior branch of the pectoral nerve runs medially to the axillary artery, before innervating the pectoralis minor. 16 It traverses along the lateral border of the pectoralis minor before innervating the distal inferior segment of the pectoralis major.16,18 When following the path of the inferior pectoral nerve, one encounters PC-1, suggesting the intended target of PC-1 is the inferior pectoral nerve. This was confirmed by electrostimulation of the superior (LU-2), middle (LU-1), and inferior (PC-1) pectoral nerves, which resulted in elevation, adduction, and depression of the shoulder complex, respectively. See Supplementary Video S4.
Deinhibition
The present authors’ found electrical stimulation of GB-23 activates the long thoracic nerve, which innervates the serratus anterior muscle, while stimulation of the SAN via SI-16-C activates all three divisions of the trapezius. Scapular stabilization is essential for coordinating glenohumeral and scapular-thoracic rhythm. 19 The lack of bony articulation from the scapula to the thorax makes the scapula reliant on the stability of its surrounding muscles. 20 They stabilize the scapula on the thorax and thereby permitting the scapula to glide during movement. 20 Previous studies of patients with shoulder impingement demonstrated decreased activation of the serratus anterior (protraction) and lower trapezius (depression) muscles while having an increased activation of the upper trapezius (elevation) muscle.21–23 The present authors demonstrated that electrostimulation of GB-23 and SI-16-C can create precise scapular movements. Electrical stimulation of these points is expected to improve the stability of the scapula through deinhibition of the serratus anterior and lower trapezius.
Limitations
The four rotator cuff muscles are supraspinatus, infraspinatus, teres minor, and subscapularis. The present authors identified SI-12 and SI-11-C as branches of the suprascapular nerve to the supraspinatus and infraspinatus, respectively. A limitation of this study is that neither JYJ nor CAM described points that directly target the teres minor or subscapularis. However, teres minor is innervated by the axillary nerve. Based on the evidence presented, SI-9 corresponded to the axillary nerve. Therefore, teres minor can be indirectly accessed via electrostimulation of SI-9.
The present authors considered HT-1 as a possible point for targeting the subscapularis, as HT-1 is located within the axilla area where the subscapularis muscle could theoretically be accessed from the anterior surface of the scapula. The modern text CAM describes HT-1 to be located at the center of the axilla on the medial side of the axillary artery. 7 The JYJ mentions that the HT-1 is in between the two sinews next to the pulsating vessel (data not shown). It is the authors’ opinion that the two sinews referenced are the pectoralis major and the latissimus dorsi, which define the axilla and the pulsation to be the axillary artery from the brachial neurovascular plexus. 24 Since the pulsation associated with HT-1 is likely to be the axillary artery, and therefore the neuroanatomical target would be the accompanying brachial plexus, it is unlikely for the intended target to be the subscapularis or its associated innervation.
CONCLUSIONS
Based on the evidence gathered from literature review, cadaver dissection, and electric stimulation, it is evident that acupuncture points on the shoulder girdle region as described by the JYJ are intended to stimulate specific neurovascular bundles. This study revealed three acupuncture points that showed discrepancies with respect to point location when comparisons were made between JYJ and CAM. These three points are SI-11, SI-13, and SI-16. Points and their associated nerves that are responsible for specific planes of shoulder movement such as elevation/depression, abduction/adduction, protraction/retraction, and external rotation have been characterized. A clear understanding of the precise neuroanatomical targets of each acupuncture point is important, as it improves needling specificity, making it possible to confirm that specificity by checking for expected muscle activation using electrostimulation devices. The outcome of this specificity is improvement in interpractitioner reproducibility. These standardized neuroanatomical targets permit accurate comparison of the benefit of the same acupuncture points published by different research groups. Last, it is hoped that the information presented here will facilitate the design of more replicable treatment protocols as well as novel electrotherapeutic devices for shoulder pain and dyskinesia.
AUTHOR DISCLOSURE STATEMENT
The authors have no conflicts of interest to declare.