
Abstract
Background:
Acupuncture and moxibustion (AM) are effective for pain relief and chronic disease management but carry risks of adverse events (AEs). Japan prioritizes AM safety, and Hiroshima University Hospital Kampo Clinical Center (HUHKCC) follows strict professional standards to ensure both safety and efficacy.
Objectives:
The study analyzes AM-related AEs in Japan over the past decade, compares them with HUHKCC practices, and proposes risk mitigation strategies.
Methods:
AM-related AEs from 2013 to 2024 were reviewed using case reports from the Ichushi-Web, CiNii, and Accident Information Data Bank System (AIDBS) databases, alongside data from HUHKCC (October 2023–2024). Patient information and AEs were collected from electronic medical records and a survey of six acupuncturists. Data analysis was performed using bibliometric methods in Excel and BioVenn.
Results:
An analysis of 55 studies and 153 AEs showed a fluctuating trend, with insertion needle technique (INT) accounting for 89.1%. Common AEs included internal injuries (32.7%) and infections (21.8%). AIDBS data indicated 12 AEs annually, with 66% from INT and 33% from moxibustion. Conversely, HUHKCC’s 568 sessions reported no adverse effects; however, side effects such as fatigue or localized pain were reported in 10 cases. One reason for less AEs is that contact needle technique (CNT) was used in 96.8% of sessions.
Conclusions:
Despite Japan’s emphasis on AM safety, AM-related AEs remain consistent. Although effectiveness of each technique requires evaluation, the HUHKCC model, with its focus on CNT, diagnostics, and practitioner training, might effectively mitigate AEs and offer a valuable framework for improving AM safety.
INTRODUCTION
Acupuncture and moxibustion (AM) have significant therapeutic effects in alleviating pain and managing chronic diseases,1–3 employing techniques such as the contact needle technique (CNT), insertion needle technique (INT), and moxibustion. CNT involves gently pressing the needle against the acupoint without penetrating the skin, achieving therapeutic outcomes.4,5 INT requires the insertion of needles into specific acupoints to achieve therapeutic effects, 6 such as acupuncture-induced analgesia. This process operates through complex neural mechanisms, including signal transmission via the ventrolateral funiculus of the spinal cord and the modulation of brain nuclei. 7 Moxibustion involves burning moxa near or on the skin’s surface, 8 activating heat-sensitive immune cells and heat shock proteins through thermal stimulation to produce a warming effect and promote pain relief and immune modulation. 9
Despite their significant therapeutic potential, these techniques are associated with certain adverse events (AEs) due to factors such as the invasiveness of needle insertion and the burning involved in moxibustion. AEs refer to any unfavorable medical occurrences during or after treatment, regardless of causality, and can be classified into two categories: side effects, which are predictable, mild, and often unavoidable physiological reactions such as fatigue or slight hemorrhage, and adverse effects, which refer to unintended medical incidents beyond typical side effects, ranging in severity from mild, unintended effects such as mild or moderate pain to serious incidents such as infections or organ damage. 10 In our analysis of AEs in Japan, we adopt the definitions outlined in the 2020 “Acupuncture Safety Measures Guidelines,” 11 which distinguish side effects from other AEs based on their nature and severity.
Japan places significant emphasis on the safety management of AM. In 1993, it released an infection control guideline, and in conjunction with the 1999 World Health Organization international standards, the “Acupuncture Medical Safety Measures Handbook” was introduced in 2010 to guide accident handling and legal responses. 12 In 2020, this was updated to the “Acupuncture Safety Measures Guidelines” to promote the safety and international standardization of AM. Nevertheless, AEs still occur occasionally.13,14 Globally, numerous adverse effects and side effects have been reported, with the most common being internal organ or tissue injury (e.g., pneumothorax and central nervous system damage),15,16 infections, and cardiovascular or vagus nerve reactions (e.g., changes in heart rate and fainting).17–19 Furthermore, Japan has established a national-level platform for collecting accidents that occurred in consumer life—the Accident Information Data Bank System (AIDBS) (https://www.jikojoho.caa.go.jp/ai-national/), including reports on AM-related AEs. Therefore, reducing the occurrence of AEs is a significant issue to be addressed.
Hiroshima University Hospital Kampo Clinical Center (HUHKCC) also offers AM treatment, primarily using CNT in combination with INT and moxibustion. HUHKCC follows professional operational standards, conducting comprehensive diagnostic evaluations to develop personalized AM treatment plans for patients.
The objectives of this study are (1) to compile data on AM-related AEs in Japan over the past decade, with the aim of identifying key risks and contributing factors, (2) to conduct a comparative analysis with the clinical practices of the HUHKCC, and (3) to provide recommendations for mitigating AM-related AEs.
METHODS
Information Sources and Searching Strategy
This study searched the Ichushi-Web and CiNii databases for case reports related to AM-related AEs published between 2013 and November 2024. Relevant references were also manually retrieved as Supplementary Data. The search strategy combined “acupuncture” and “moxibustion” as intervention types and “adverse events,” “side effects,” “safety,” and “harm” as keywords for study types. Simultaneously, we searched the AIDBS for AE cases registered between 2013 and November 2024 using the keywords “acupuncture” and “moxibustion.”
Inclusion and Exclusion Criteria
The inclusion criteria were case reports and case series studies published in Japan related to any type of acupuncture or moxibustion, involving AEs following acupuncture, electroacupuncture, or moxibustion treatments. The exclusion criteria included studies unrelated to AEs, non-case reports (such as reviews and randomized controlled trials), studies with incomplete or unclear data, duplicate studies, and studies that did not explicitly specify the AM treatments used. The same exclusion criteria were applied to the reports in the AIDBS.
Data Collection Methods at HUHKCC
This study included patients who received AM treatment at HUHKCC between October 1, 2023, and October 31, 2024. Basic patient information (gender and age), AM treatment methods, disease types, and whether any AEs occurred during or after treatment were collected through the electronic medical record system. Meanwhile, a questionnaire survey was conducted among 6 acupuncturists at the HUHKCC, covering their work experience, the number of patients they see per week, the occurrence of side effects during AM treatment, and their evaluation of treatment effectiveness.
Data Analysis
This study employs bibliometric analysis to assess the publication trends of AM-related AEs case reports and conducts a descriptive analysis to summarize the case distribution, temporal trends, and types of AEs. Data analysis was performed using Excel and BioVenn software to generate charts and tables for visual presentation.
RESULTS
Results of Data Collection and Screening
Figure 1 outlines the process of data collection and screening from three distinct sources: academic research databases, AIDBS, and HUHKCC.

Data collection and screening processes. AEs, adverse events; AIDBS, Accident Information Data Bank System; AM, acupuncture and moxibustion; HUHKCC, Hiroshima University Hospital Kampo Clinical Center.
A total of 231 records were identified through searches in Ichushi-Web (n = 197) and CiNii (n = 34). An additional 67 references were manually retrieved as Supplementary Data. After screening, 170 records unrelated to AEs, 40 non-case reports or case series, 5 records with incomplete or unclear AEs, 20 duplicates, and 8 studies without specific AM treatments were excluded. Ultimately, 55 studies met the inclusion criteria. A total of 410 AM-related AEs registered between January 2013 and November 2024 were reviewed. Following the exclusion of 68 unrelated records, 68 non-case reports or case series, 119 cases with incomplete or unclear data, and 2 cases without explicitly specified AM treatments, 153 cases were included for analysis. Among 84 patients who received treatment at HUHKCC between October 2023 and October 2024, 5 patients were excluded as they did not undergo acupuncture or moxibustion treatments. Therefore, 79 patients and a total of 568 treatment sessions were included in the analysis.
Literature Results on AM-Related AEs
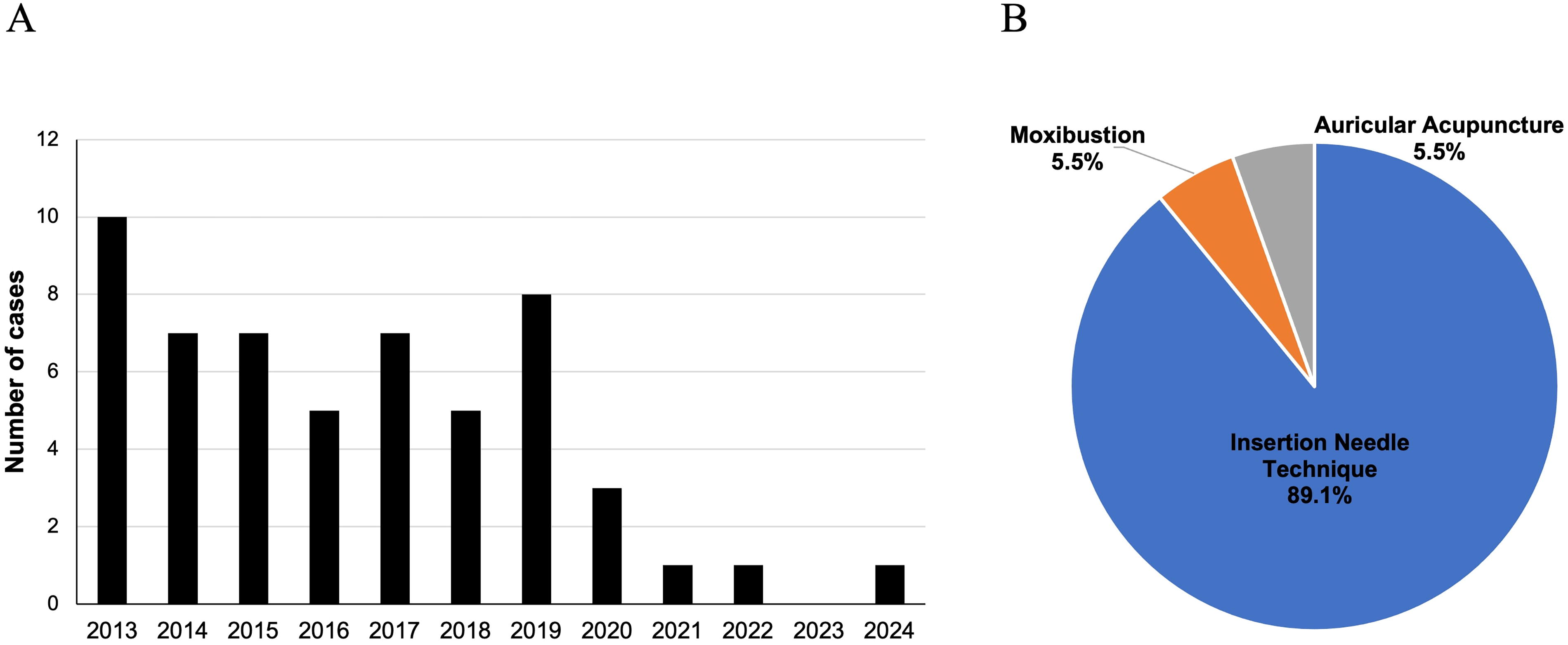
Statistics from 2013 to 2024 indicate a fluctuating trend in the number of publications and reported cases of AM-related AEs, with a notable decline in publication numbers since 2020 (Fig. 2A). Classification by treatment modality (Fig. 2B) shows that INT was the primary method associated with AEs, accounting for 89.1%. In contrast, moxibustion and auricular acupuncture accounted for only 5.5% each. The types and frequencies of adverse effects are presented in Table 1. The most common AE was internal organ or tissue injury (32.7%), followed by infections (21.8%). Events involving broken acupuncture needle accounted for 16.4%, while skin disorders made up 9.1%. Nerve injury and moxibustion burns accounted for 7.3% and 5.5%, respectively.
The Types and Frequencies of Adverse Effects
AIDBS Results on AM-Related AEs
Among the 153 AM-related AEs registered in the AIDBS between 2013 and 2024, the annual number of AEs remained relatively stable, with an average of ∼12 cases per year (Fig. 3A). The distribution of AEs by AM technique (Fig. 3B) shows that INT accounted for the majority, with 101 cases (66.0%). In comparison, moxibustion-related AEs represented 33.3% of the total, while non-insertion needle techniques accounted for only 0.7%. A classification of adverse effects and side effects (Table 2) reveals that adverse effects comprised 61.4% of all cases, with moxibustion contributing to 54.3% of these adverse effects. Internal organ or tissue injury was reported in 23.4% of the total AEs. In addition, side effects accounted for 38.6% of all AEs, with local side effects making up a significant proportion (81.4%) of the total side effects.

The Types and Frequencies of Adverse Effects and Side Effects
Comparison of AIDBS and HUHKCC Results on AM-Related AEs
From October 1, 2023, to October 31, 2024, a total of 13 AM-related AEs were registered in the AIDBS. Among these, acupuncture-related cases accounted for 77%, while moxibustion-related cases accounted for 23%. Adverse effects related to acupuncture included nerve injury (22.2%) and internal organ or tissue injury (11.1%). All reported side effects were localized. Moxibustion-related AEs (23%) were exclusively burns (as shown in Table 3).
AIDBS Reported AM-Related Adverse Effects and Side Effects (October 1, 2023–October 31, 2024)
In the same year, the results of HUHKCC (Fig. 4A) showed that 79 patients received AM treatment, with a total of 568 sessions. The treatment mainly focused on pain and neurological diseases. Based on the judgments of doctors and acupuncturists, as well as patients’ self-reported improvements, effectiveness was observed in 480 out of 568 treatment sessions, resulting in an effectiveness rate of 84.5%. The primary approach was combined therapy, with CNT being the most widely used in AM treatment at HUHKCC, accounting for 96.8% (550 sessions). Moxibustion was also commonly used in combination with acupuncture, accounting for 96.7% (549 sessions). INT still accounted for a certain proportion, 68.8% (391 sessions). AEs analysis revealed no adverse reactions, only side effects, with local and systemic side effects each accounting for 50%. The classification of side effects revealed that fatigue was reported in 3 cases. Localized pain and malaise at the needle insertion site were each reported in 2 cases. Other side effects included itching after acupuncture, scintillating scotoma, and localized numbness after needle insertion, with each occurring in 1 case (Fig. 4B).

The questionnaire results in Table 4 showed that acupuncturists had 1–5 years of experience, and patients’ main complaints consisted of musculoskeletal and mental and behavioral disorders. CNT was a commonly used technique. Fatigue was considered the most common side effect. All acupuncturists agreed that CNT had significant therapeutic effects during the treatment process.
Acupuncturist Questionnaire Survey at HUHKCC
DISCUSSION
AEs Associated with INT
From 2013 to 2024, no literature specifically reported on side effects, while 55 papers related to AEs. Due to the limited sample size, we were unable to analyze the trends and causes of AEs based on these data. INT is the primary treatment leading to AEs (Fig. 2B), with internal organ or tissue injury and infection being the most common (Table 1).
To understand the trends in AEs, we analyzed the AEs reported in AIDBS. The results (Fig. 3A) indicate that the annual number of reported cases has remained stable at ∼12 cases per year. This suggests that the actual incidence of AM-related AEs has not significantly decreased. While the promotion of the “Acupuncture Safety Measures Guidelines” may help mitigate AEs to some extent, its impact appears to be limited. Thus, it is crucial to develop new strategies to effectively reduce the occurrence of AEs.
Similar to Figure 2B, Figure 3B also indicates that INT is the primary AM treatment leading to AEs. Consistent with Table 1, Table 2 also shows that the most common AEs involve internal organ or tissue injury. According to reports, the main causes of these injuries are attributed to improper operation and needle selection.20–22
In addition, we analyzed the proportion of adverse effects and side effects in the AIDBS data. As shown in Table 2, adverse effects accounted for 61.4% of AEs, while side effects account for 38.6%. This finding highlights that adverse effects constitute a significant proportion of AM-related AEs, emphasizing the importance of strategies to mitigate them effectively.
AEs Associated with Moxibustion
The results in Table 2 show that the proportion of AEs caused by moxibustion is also relatively high. Reported causes of moxibustion-related AEs include inadequate distance between moxa and skin, excessive treatment duration, and practitioners’ lack of proficiency. 23 Establishing appropriate treatment durations, maintaining an optimal distance between the moxa and skin, and conducting regular training for practitioners can help reduce the occurrence of moxibustion-related AEs.
It is also noteworthy that most of the reported cases involve burn incidents caused by moxibustion. Moxibustion treatment often results in suppuration and scarring, which are generally perceived by patients as AEs. However, acupuncturists often consider these outcomes as normal effects of the treatment. 24
AEs Associated with Patients’ Perception
As discussed in “Introduction,” the actual incidence rate of AM-related AEs has not significantly decreased. This result may be related to patients’ perception. For instance, from the perspective of traditional medicine, temporary symptoms are often seen as natural responses of the body to acupuncture rather than as side effects. This phenomenon is referred to as the Healing Crisis, and such reactions typically subside within a few days. 25 However, if patients perceive these natural post-acupuncture responses as side effects or even adverse effects and report them themselves, this could be one of the reasons why the occurrence of AEs remains stable. 26
The AM Treatment Model at HUHKCC
We analyzed AEs reported by HUHKCC and AIDBS from October 1, 2023, to October 31, 2024.
As shown in Table 3, the AIDBS reported a total of 9 cases of adverse effects and 4 cases of side effects related to AM treatment. In contrast, HUHKCC recorded no adverse effects. The side effects observed at HUHKCC were predominantly mild, with 10 instances noted, the most common being fatigue.
Due to the lack of data on the total number of treatments in the AIDBS and its focus on case counts rather than treatment frequencies, a precise comparison of side effects was not feasible. Therefore, our analysis focused exclusively on comparing the reported adverse effects between the two datasets.
According to reports from the United States, China, Germany, Britain, Korea, and other countries, the incidence of AEs in acupuncture treatments ranges from 0.671% to 11.4%.10,27–29 In comparison, the HUHKCC reported no adverse effects, achieving a treatment effectiveness rate of 84.5% across 568 AM treatments, with only 10 instances of minor side effects, indicating a very low risk. These findings suggest that the HUHKCC model warrants further attention and consideration.
HUHKCC primarily utilizes a combination of CNT, moxibustion, and INT, with a particular emphasis on prioritizing CNT. For INT, a superficial insertion method is applied, with a depth of ∼4–10 mm, while avoiding direct stimulation of high-risk areas such as the chest, abdomen, and spine. During moxibustion therapy, the sensation of heat at acupoints can vary depending on the specific location being treated. As a result, acupuncturists carefully monitor the patient’s perception of warmth throughout the procedure. To ensure safety, the moxa is typically extinguished after ∼60–70% of it has burned, before being applied to other treatment areas.
In addition, at HUHKCC, physicians and acupuncturists work as a cohesive team to evaluate and treat patients, ensuring more effective prevention of AEs. Through this multidisciplinary collaboration, they share patient information, align their goals, and develop a unified treatment approach. The HUHKCC conducts a comprehensive evaluation of patients’ physical and mental states—including their constitution, symptoms, and other factors—through pulse diagnosis, abdominal diagnosis, and tongue diagnosis (guided by the theoretical foundation of Kampo Medicine: The First Step Toward Classical Formulas), as well as in-depth communication with patients. This comprehensive approach enables the creation of personalized treatment plans, significantly reducing the risk of safety issues caused by mismatched therapies.
In addition, HUHKCC has implemented a systematic training and evaluation program for acupuncturists. This program includes comprehensive education in the fundamentals of Kampo medicine, hands-on training in AM techniques, and regular assessments of diagnostic skills (including the four diagnostic methods), theoretical knowledge, and practical proficiency. This rigorous training and management system effectively enhances acupuncturists’ professional competencies, further reducing the likelihood of AEs. The promotion of HUHKCC model could play a pivotal role in reducing AEs and serve as a valuable reference for improving the safety of AM practices.
CONCLUSIONS
This study analyzed AM-related AEs in Japan from 2013 to 2024, identifying the INT as the primary cause, particularly for internal organ injuries and infections. Moxibustion-related burns were also notable risks. Despite the implementation of safety guidelines, the incidence of AEs has not significantly declined. However, HUHKCC reported only minor side effects in AM treatments, demonstrating that its model, characterized by comprehensive diagnostics, prioritization of low-risk techniques such as contact needle therapy, personalized treatment plans, and systematic acupuncturist training, can effectively minimize AEs. Although this model has demonstrated its effectiveness, its application remains limited by the representation of the data and the sample size. Future research should expand the dataset to further refine and enhance the implementation and dissemination of this model.
Footnotes
ACKNOWLEGMENTS
The authors thank all contributors for their efforts in data collection and analysis. They also extend their sincere gratitude to all acupuncturists in HUHKCC for their valuable assistance in completing the questionnaire.
AUTHORS’ CONTRIBUTIONS
Conceptualization: Y.J. Methodology: H.L. Investigation: Y.U. and K.H. Data curation: Y.Y. and Y.W. Writing—original draft: Y.J. Writing—review and editing: K.O.-O. and Y.T. Supervision: K.O.-O.
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this review.