
Abstract
Objective:
To report on our experience treating patients in an academic medical acupuncture practice in a rural setting and set the stage for future research.
Methods:
Our healthcare systems electronic medical record was queried for all patients seen in the general internal medicine clinic for acupuncture since the service was first offered. Data on demographics, medical diagnoses were extracted and anonymized. Diagnoses were grouped by their ICD–10 codes. Zip code was collected to help ask the question whether distance or socioeconomic and education status had an impact on use of this service. Data was analyzed using standard descriptive and analytics methods.
Results:
A total of 200 patients over a 7 year period for a total of 1534 visits. Average number of visits was 7.75, age 66 yrs old and were 63.8 % female. The majority of patients terminal degree was High School, had a median income of $82 K and the and a median distance travel of 34 miles. The lower the terminal degree the greater distance travelled. The top three diagnostic categories were musculoskeletal, mental health and neurologic. Pain was the secondary complaint in 27.4% of cases.
Conclusions:
Acupuncture appears to be an acceptable therapeutic option for rural patients. This is evidenced by the willingness-to-travel, the broad range of problems being addressed and the wide socioeconomic profile taking advantage of the service.
INTRODUCTION
Rural communities often have less access to care and worse health outcomes. About one in five US residents—nearly 60 million people—live in rural areas, covering 97% of the nation’s land mass. Here rural is defined as regions of low population density, limited institutional resources, and long distances and travel times needed to access those resources. 1 Rural United States is also home to disproportionate shares of the elderly, chronically ill, and those suffering from opioid abuse disorder.2,3 Much of the research on rural health disparities examines those between rural and urban communities, rather the those within rural communities themselves. Yet there is evidence that disparities within the rural setting is a growing problem. 4 It should be noted that rural populations vary considerably depending on where they are in the country. What they all share in common is low population density and limited access to healthcare resources.
Acupuncture is a technique in which practitioners stimulate specific points on the body—most often by inserting thin needles through the skin, to promote healing and improve function. It emphasizes the whole person’s health. The range of problems treated is as wide as other healthcare frameworks, such as allopathic and osteopathic medicine but is most commonly used for injury, musculoskeletal (MSK) issues, and cerebrovascular issues such as stroke. 5 Acupuncture is used widely throughout the world yet in the United States access to this care is limited. 6
Though the number of total licensed acupuncturists has increased 257% since 1998, the overall acupuncturist density in the United States is low 11.63 acupuncturists per 100,000 (total number of licensed acupuncturists: 37,886, divided by the total population: 325,719,178 at the start of 2018). By contrast, there are 67.2 primary care providers/100,000 and 247.5 physicians/100,000 in 2021 (www.aamc.org). There were 20 states with an acupuncturist density of more than 10 per 100,000 population. 7 Hawaii (52.82) was the highest, followed by Oregon (34.88), Vermont (30.79), California (30.69), and then New Mexico (30.27). Of these, only Vermont is considered a majority rural state (www.census.gov, 2018).
Acupuncture is an effective therapeutic option for many common conditions presenting in primary care.8,9 This is especially true for problems that often are inadequately treated by standard allopathic care. These conditions include chronic pain, depression, various MSK injuries, and visceral hypersensitivity syndromes such as fibromyalgia or irritable bowel syndrome. In the case of chronic pain, there is evidence that persons living in rural areas may be more likely to have chronic pain and less likely to use nonmedication treatments than those in urban areas. 10 Mental health (MH) issues also seem more prevalent in rural settings though less studied.11,12
Acupuncture is also very portable, safe, and requires minimal logistical support perhaps making it an ideal resource to address rural healthcare needs. However, acupuncture is often considered external to mainstream medical care and patients who seek it out often have to go outside the standard medical system to gain access. 13 This is despite the persistent interest in whole person care 14 and the growing body of evidence supporting the effectiveness of acupuncture and the science behind it.15–24 This disconnect often leads to fractured care with different clinicians being unaware of what other therapies or treatments their patients are receiving.
There are several potential barriers to implementing an acupuncture practice at an academic medical center. These can include lack of knowledge in the patient population, lack of knowledge in hospital administration, hospital culture, financial/insurance concerns, and logistical reasons such as finding a qualified practitioner among others.
The purpose of this study is to report on our experience treating patients in an academic medical acupuncture practice in a rural setting and set the stage for future research.
METHODS
Dartmouth-Hitchcock Medical Center (DHMC) is situated in the Upper Valley of the Connecticut river, on the border between Vermont and New Hampshire. It serves a primarily rural population drawing equally from both states. The acupuncture practice was set up as one afternoon per week embedded within the hospital-based general medicine clinic. Patients could be referred for acupuncture both from within the clinic, from outside the clinic, or could self-refer. Once referred, the patients would undergo an intake medical and acupuncture evaluation. The purpose of this was to (1) be sure the patient was first being appropriately managed from an allopathic perspective. For example, if a patient presented with fatigue and depression and no one had checked a TSH or had low back pain and had not been tried on NSAIDs or physical therapy, (2) assess how amenable or not someone would be to acupuncture, (3) check if the patient was appropriately managed from an allopathic perspective, then a history and physical from a TCM/CCM perspective was performed to determine a preliminary diagnosis and an acupuncture therapeutic plan.
The patient would then be scheduled for initial 4–6 weekly appointments. This was felt to be enough sessions to determine if acupuncture was going to have any benefit while at the same time creating a stopping point if it was not helping. If it was helping, then treatment would continue for as long as the patient was benefitting. Intervals between visits were extended for stable patients until a stable maintenance interval was determined.
DHMC uses EPIC™ as its electronic health record (EHR). The records of all patients who received acupuncture in the general internal medicine practice were pulled using Epic queries. Data on their demographics and medical diagnoses were extracted and anonymized. International Classification of Diseases, 10th Revision (ICD-10) codes were grouped by their top grouping level, for example, diseases of the Musculoskeletal (MSK) system M00-M99. In addition, they were categorized if “pain” was part of their diagnosis. In addition, zip code was collected to help ask the question of whether distance or socioeconomic and education status had an impact on the use of this service.
Data were analyzed using standard descriptive and analytics methods, including t-test, ANOVA, linear regression for continuous variables, and tools such as Chi-squared, Mantel–Hansel, and Fisher’s exact tests for categorical variables. JMP 17 (www.jmp.com a SAS product) software was used for the analysis.
This project was approved by the DHMC internal review board.
RESULTS
The population served by DHMC and the clinic is relatively homogenous ethnically and older. It is very diverse with regards to economic and educational status (Table 1). The sample had a somewhat higher percentage of high school graduation as their terminal degree than the nationally (42% vs 28% www.census.gov 2022). Median income was also slightly higher than the national average ($82K vs $75K). Nationally the average travel time to work was 27.6 min in 2019. The average distance to a hospital has been reported as 4.4 mi (urban), 5.6 mi (suburban), 10.5 mi rural. 25 Our population averaged 35 miles to the clinic. In our population, the lower the patients’ educational achievement, the further they traveled for the service (Fig. 1).
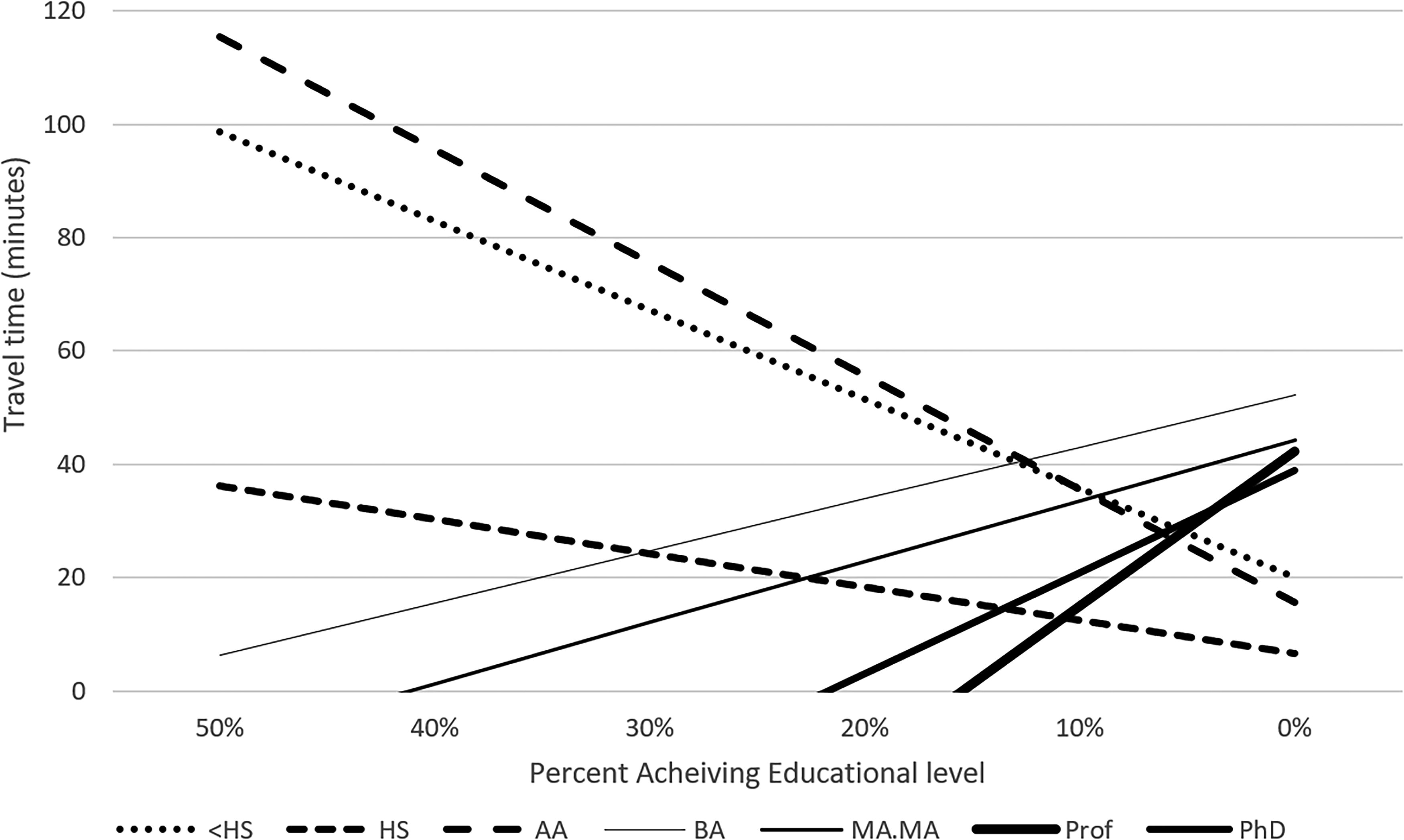
Proportion of patients willing to travel as measured by time cost, as a function of the educational level achieved.
Demographics
AA, associate of arts; BA, bachelor of arts; HS, High School; MA, Masters of Arts; MS, Masters of Science.
The age distribution by clinical category is seen in Figure 2.
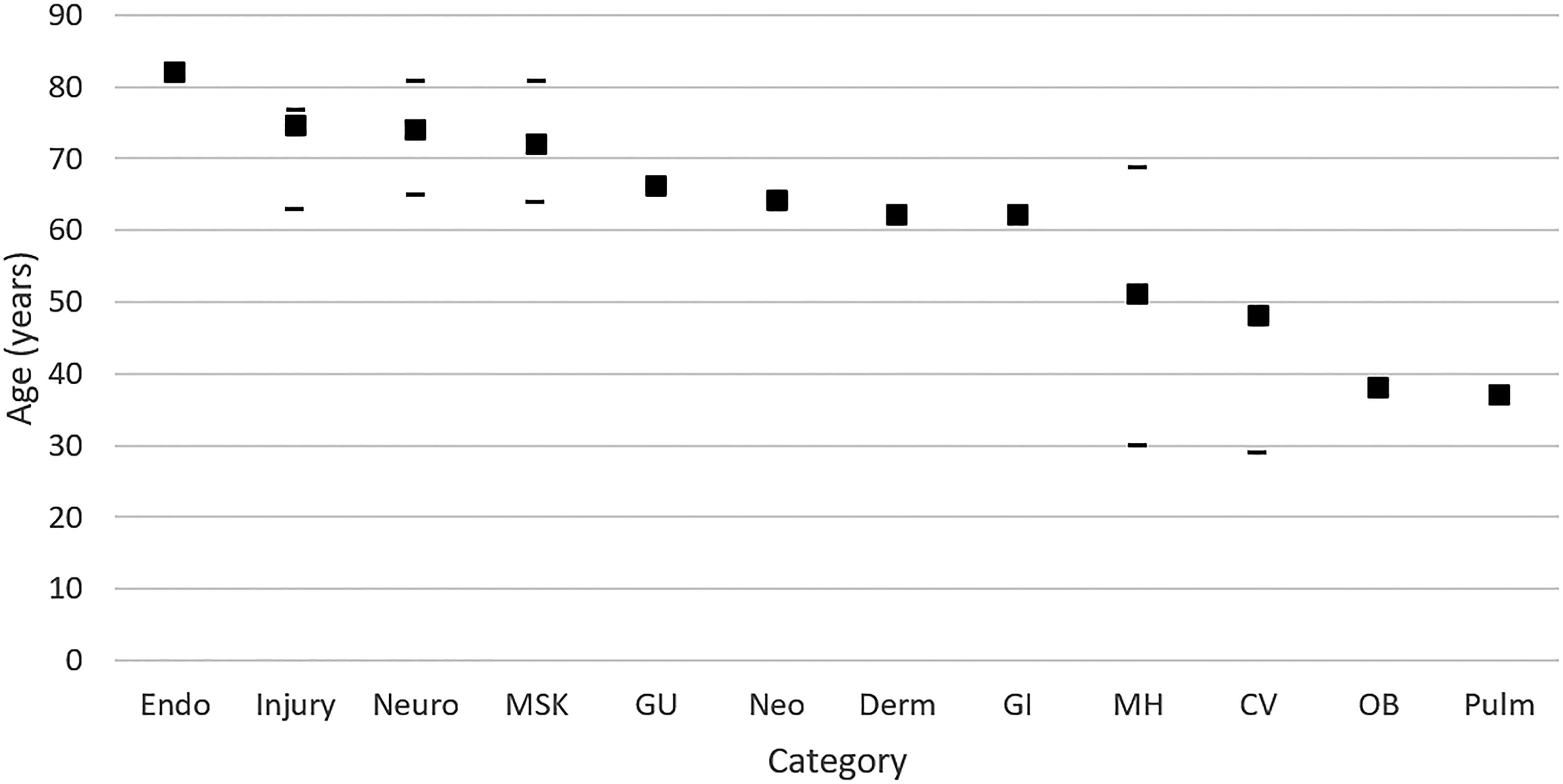
The mean and interquartile range of ages within their presenting clinical category. MH, mental health; MSK, musculoskeletal; Neuro, neurological; Pulm, pulmonary.
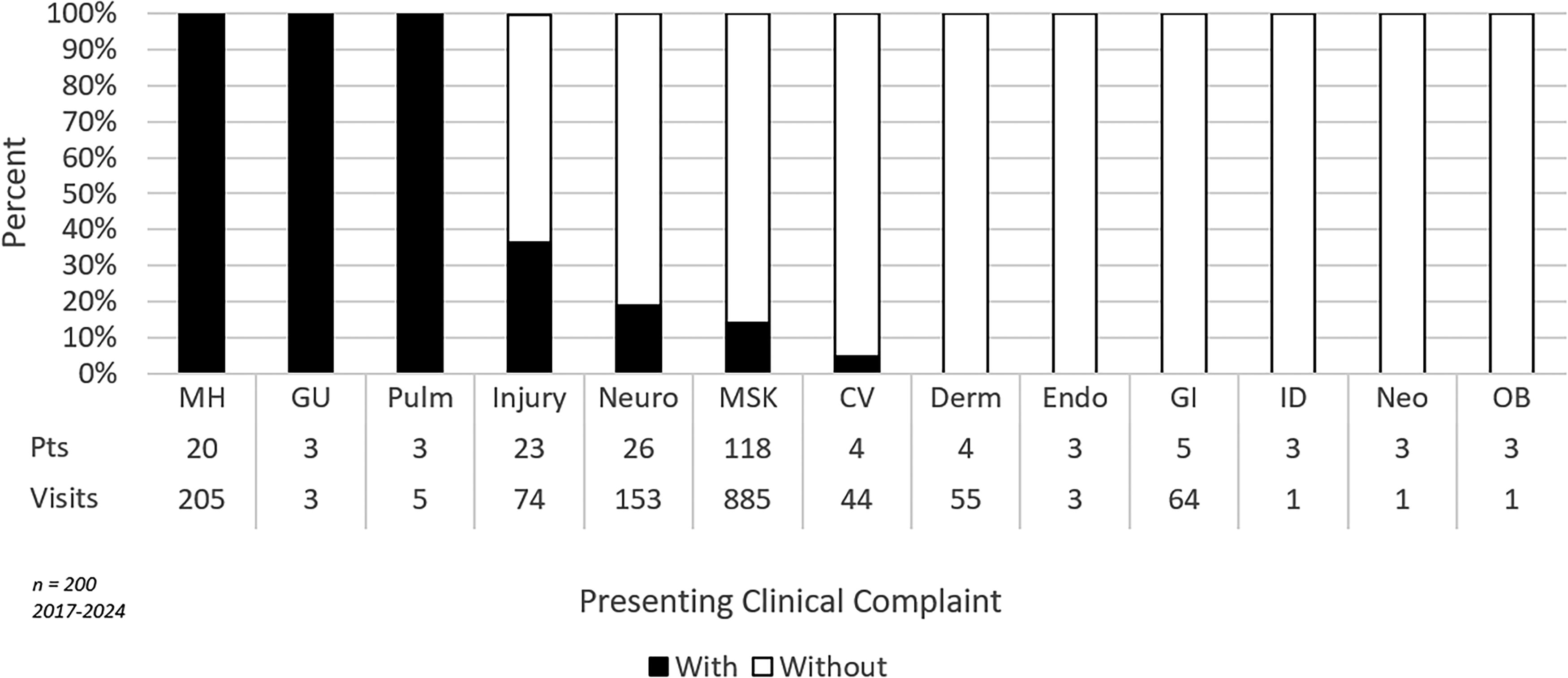
When examining the reasons patients presented, the three main concerns were MSK (57.6%), mental health (MH) (13.3%) and neurological (Neuro) (10%) in nature. Pain itself was the secondary complaint in 27.4% of cases, with MSK (85.6%) and Neuro (12.6%) explaining most (Fig. 3). Low back pain, hip and leg pain, and chronic pain syndromes were the most common specific diagnoses associated with pain. With regard to gender (Fig. 4), men and women were approximately equally likely to present with MSK problems. Men were more likely to present with CV, Neuro, or direct injury. Women more likely to present with gastrointestinal (GI), MH, and all other categories (Fig. 5).
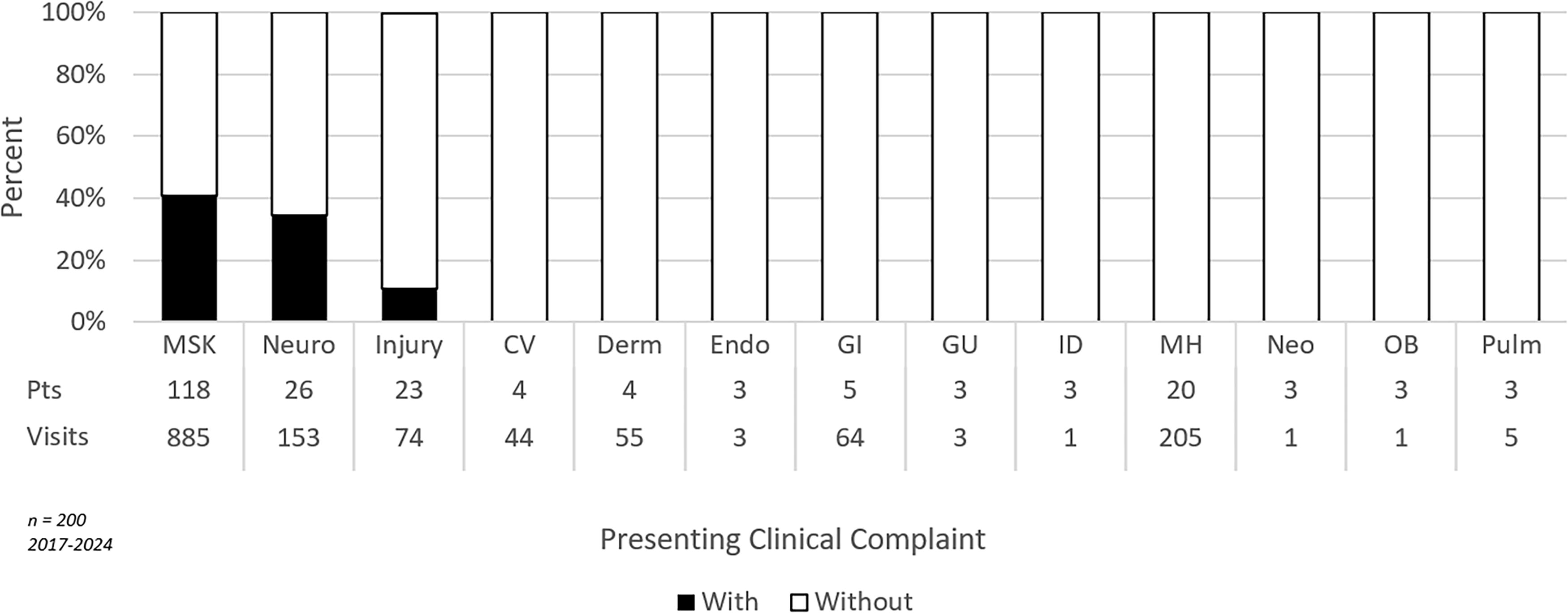
Percentage of patients presenting with pain within their presenting clinical category. MH, mental health; MSK, musculoskeletal; Neuro, neurological; Pulm, pulmonary.
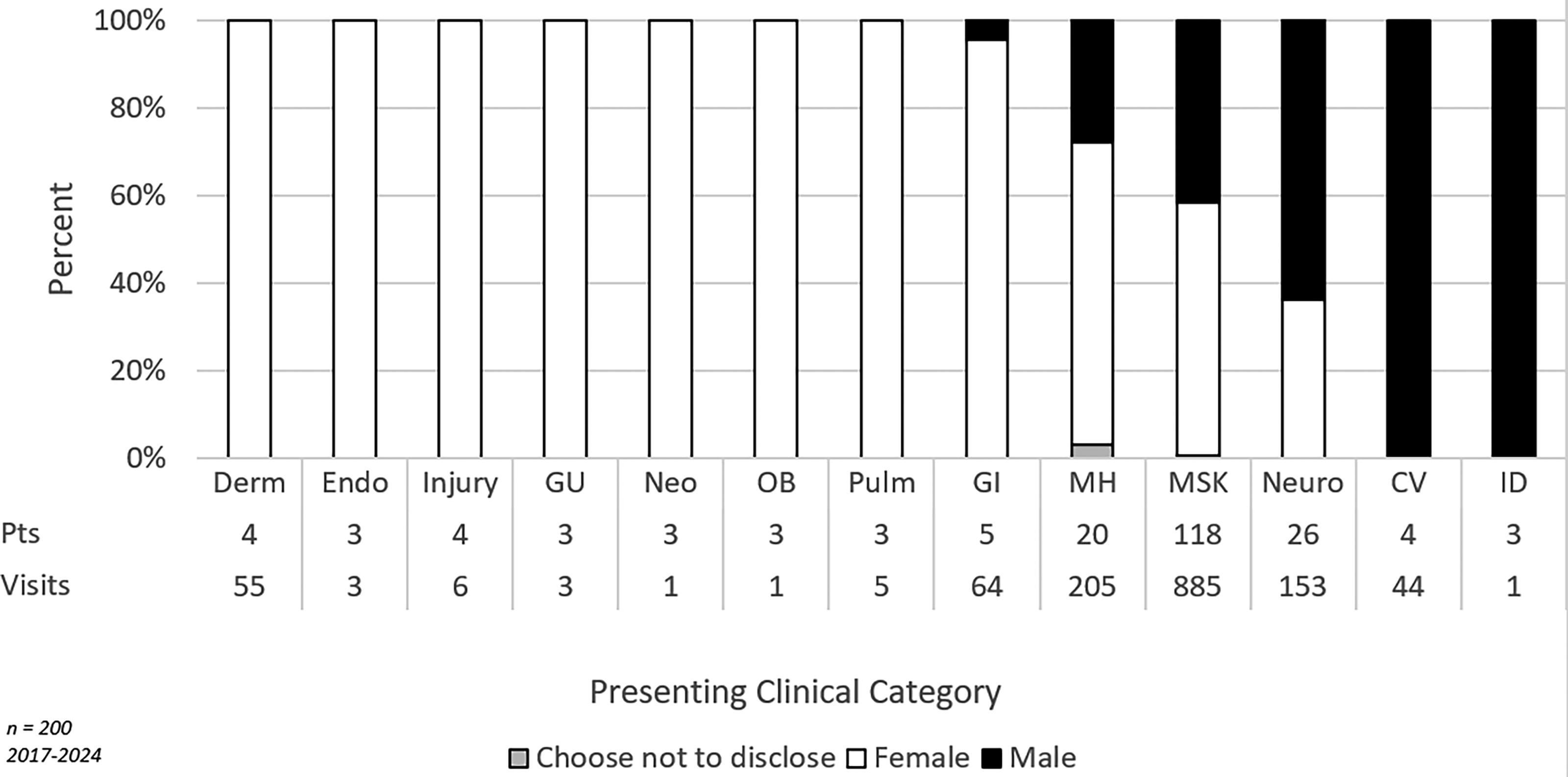
Percentage of male and female patients presenting within their presenting clinical category. MH, mental health; MSK, musculoskeletal; Neuro, neurological; Pulm, pulmonary.
Percentage of patients presenting mental health concerns within their presenting clinical category. MH, mental health; MSK, musculoskeletal; Neuro, neurological; Pulm, pulmonary.
With regard to those who presented with only an MH concern, the largest categories were stress (42%), adjustment-related insomnia (34%), and anxiety disorder (15%). genitourinary (GU) and pulmonary were the non-MH categories most associated with MH concerns (Fig. 5).
With regard to travel time, there was no difference between travel time with regard to MH being their primary concern. However, patients were significantly more willing to travel if they were in pain (39 min with pain vs 34 min without pain, p = 0.0002). Patients with MH as their primary concerns were more likely to have higher incomes ($120K vs $83K, p < .0001), whereas patients with pain were more likely to have lower income ($79K vs $88K, p < .0001).
Pain did not make any distinction with regard to age in this group. However, those who suffered MH concerns were statistically younger (57.4 years vs 68 years, p < 0.0001) (Figs. 6 and 7).
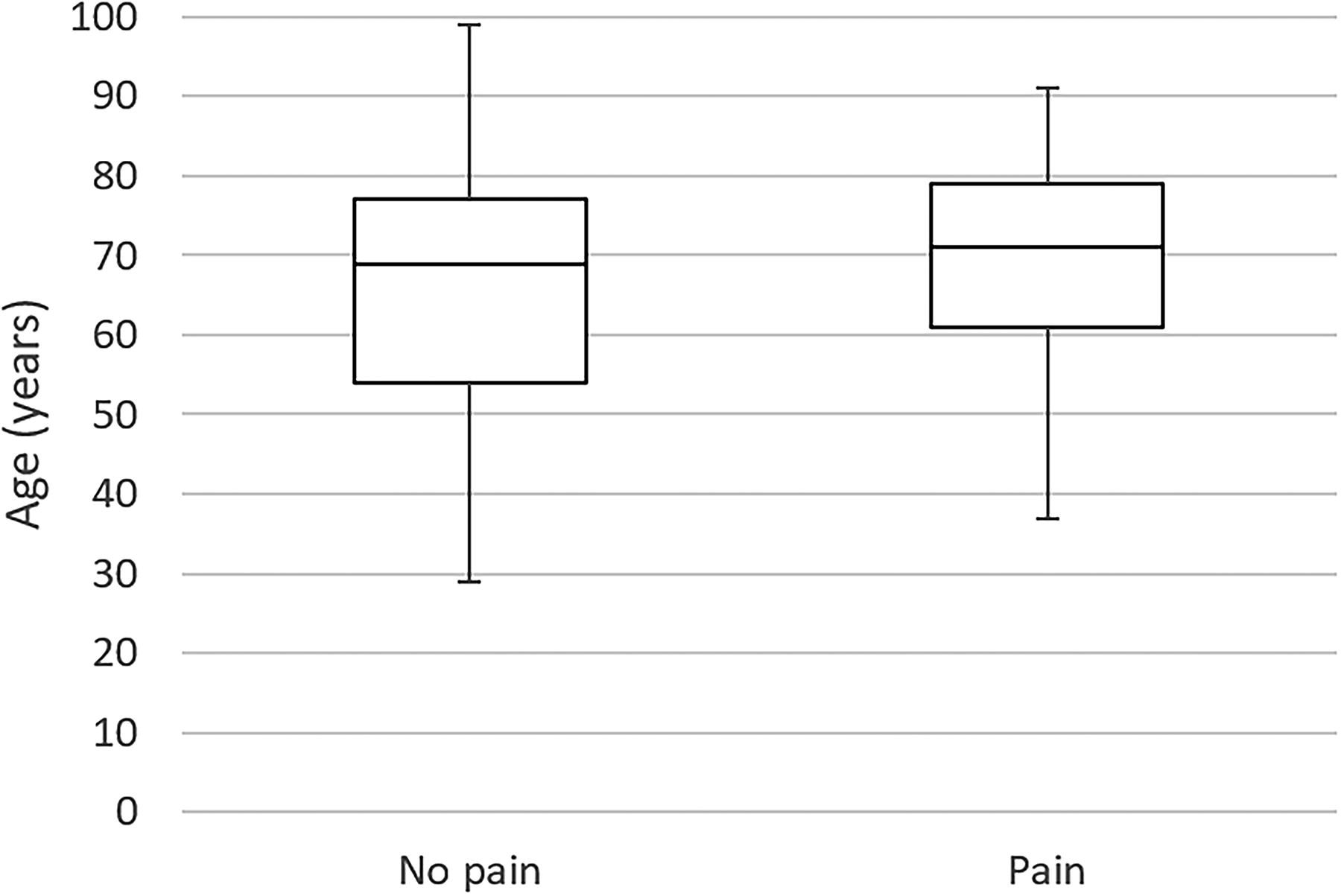
Age distributions of patients presenting with or without pain.
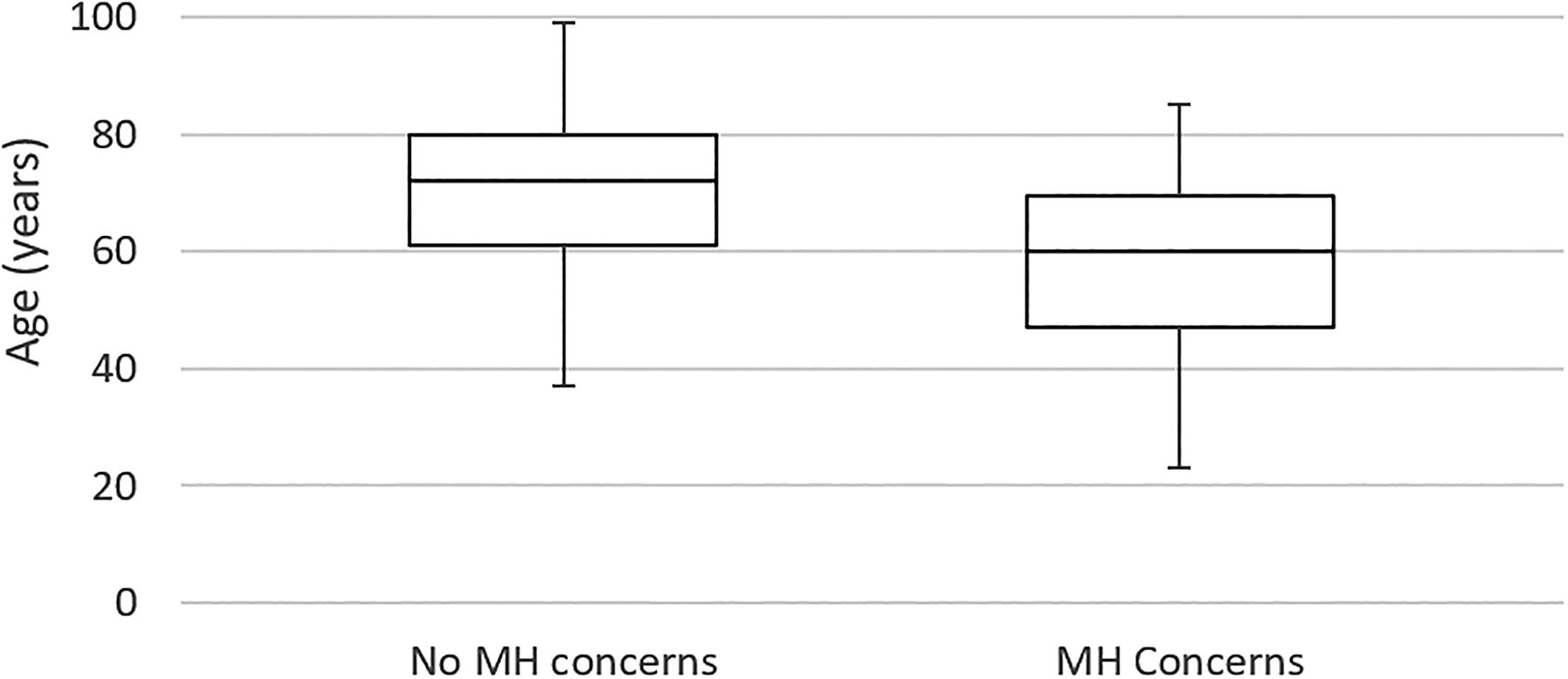
Age distributions of patients presenting with or without mental health concerns. MH, mental health.
DISCUSSION
Acupuncture appears to be an acceptable therapeutic option for patients and many clinicians in this rural setting. This is evidenced by the willingness to travel, the broad range of problems being addressed, and the wide socioeconomic profile taking advantage of the service.
As might be expected, pain and MH concerns were common complaints that overlapped with many organ systems.
Pain is a problem that involves the physical, emotional, and attentional. Its treatment thus lends itself to a whole person approach. The opioid crisis has hit rural communities particularly hard. Finding resources to address this pain pandemic is challenging and no one approach will solve the challenge. Mind–body medicine and acupuncture are well suited to help not just treat the immediate problems of pain but move people along a path toward wellness. Unfortunately, fully trained acupuncturists are scarce. That said, taking the Veterans Adminsistration (VA) as a model, tools like Battlefield Acupuncture (BFA) can be easily replicated and distributed to fill some of these gaps.
Age was a greater driver of differing use profiles than either gender or income or education.
MH was also a big driver across the board, and patients would travel greater distances for help in this domain. The general public seems more aware of acupuncture’s role in treating MH issues than the clinical establishment. This is probably related to a tacit understanding that physical pain and emotional pain are not fully separable. That being said, while self-referrals to this clinic have steadily risen since the opening of the service, so have physician referrals except for a drop during the COVID-19 pandemic, which picked up again in 2021 and currently accounts for >30% of the referrals.
Surprisingly, patients with further travel, and usually less income and education in a rural setting, were more willing as measured by willingness-to-pay to take advantage of the service. Equal use by all socioeconomic levels implies greater demand by the less well-off.
Limitations
The chief limitation of this study is that it is a retrospective descriptive study rather than one that explores effectiveness, limiting the questions that can be asked to the fields available in the preexisting dataset. It relies on administrative data pulled from the hospital EHR. EHR administrative data have well-known limitations in this context as it is designed for billing, not research.
CONCLUSION
Acupuncture is a viable and acceptable healthcare modality in the rural setting. This article was meant to be descriptive and help set the stage for future work. Some important questions that the field of acupuncture needs to answer to gain broader acceptance are what is the effectiveness of acupuncture for these presenting clinical concerns, what are the patient characteristics that may point to using acupuncture relative to other modes of care, and testing acupuncture’s role in high priority rural concerns such as substance abuse disorder.
Footnotes
AUTHORS’ CONTRIBUTIONS
J.E.S. was responsible for conceptualization, methodology, data validation, formal analysis, investigation/data collection, data curation and management, and writing the article. No funding was sought for this article.
AUTHOR DISCLOSURE STATEMENT
The author has no conflict of interest with this project. While he is the primary medical acupuncturist in this practice, he has no financial interest as the practice is owned by the hospital and the performance of the clinic does not influence his hospital-based salary. He has no intellectual property interest in the acupuncture clinic.
FUNDING INFORMATION
There were no external funding sources.