
Abstract
Tobacco use disorder is the leading cause of preventable death and disability in the United States, with one in five Americans currently smoking cigarettes. Only two non-nicotine medications are FDA approved for treating tobacco use disorder, and advances in drug discovery are profoundly outpaced by the morbidity and mortality caused by tobacco dependence. Drug repurposing may provide an approach for addressing this health hazard, offering hope to tobacco users attempting to quit who have failed existing therapies. The focus of this review is to evaluate the potential role of apomorphine (APO) in treating tobacco dependence. Previously described in the literature as a non-specific dopamine agonist effective in treating Parkinson's disease and erectile dysfunction, APO's dopaminergic targeting activity may be effective in counteracting the modified response arising from tobacco use. Here, the literature describing APO's activity is reviewed and presented in the context of known nicotine-induced response in neurotransmitter systems. Based on these data, whether APO may be an effective smoking cessation agent by ameliorating a tobacco user's anhedonic state is critically appraised, along with withdrawal symptoms and the chemical reinforcement associated with drug-seeking behaviors.
Current Tobacco Use Disorder Treatments
Tobacco use disorder is a leading cause of preventable death worldwide, and tobacco cessation is the most effective way to prevent or reduce morbidity and mortality related to tobacco use. The success rate for a smoking cessation attempt without counseling or pharmacologic therapy is 4–7%. 1,2 Nicotine replacement therapy (NRT) increases the smoking abstinence rate to 7–11%. 3,4 Long-term smoking abstinence rates are 9–11% with bupropion and 13–25% with varenicline. 5 –7 Bupropion and varenicline are the only two drugs brought to market for the treatment of tobacco use disorder in the last two decades. Recent efforts in assessing the effects of combining varenicline and bupropion 8 –10 or varenicline and NRTs 11,12 have shown improved cessation rates, but more than half of smokers relapse back to smoking after 6 months. Immunotherapy is an alternative approach to treating tobacco dependence, but it has demonstrated variable efficacy. 13,14 Given the limitations of currently available therapies, a compelling case is made for repurposing existing drugs for the treatment of tobacco dependence. Here, a review is provided of the existing scientific literature of apomorphine (APO), and the evidence to consider its use in the treatment of tobacco dependence is outlined.
Clinical History of Apo
APO is an aporphine derivative dopaminergic agonist with an extensive and varied history of medical application. Here, a short synopsis is provided of several studies and applications involving APO. It was first synthesized in 1845, and was reported to possess expectorant activity when given orally in small doses. 15 It was also briefly used to control restlessness in full-term childbirth. 16 Later, APO was given as a central acting emetic agent for treating poisoning or removal of foreign bodies in the esophagus. 17 The first research report describing APO for addiction management was released in 1899, and indicated a remarkable effect in controlling delirium tremens during alcoholism treatment. 18 Forty years later, a report detailed the elimination of alcohol cravings following APO administration. 19 In this case series, 42.5% of the 500 alcoholic patients studied reported abstinence after 5 years of treatment with APO. 20 Similar studies were performed between 1953 and 1977, and employed sub-emetic dosing intravenously (IV). Unfortunately, poor study design in these early studies led to variable patient treatment, 21 –26 and the lack of appropriate controls limits the ability to draw robust conclusions on APO's effectiveness in treating alcoholism. In 1972, investigators administered APO sublingually (SL) at a sub-emetic dose of 6 mg for 4–7 days to 51 physically healthy alcoholic war veterans. Ninety percent of these subjects reported drug craving relief. 23 Further exploration with APO subcutaneous injections in subjects with opiate and barbiturate dependence resulted in craving reduction. 17,24,26 In addition, APO has recently been shown in adult rats to possess a therapeutic potential against ethanol-induced neurotoxicity. 27 Despite these early successes, the use of APO for drug addiction treatment was not adopted. The presence of impurities in early preparations, 28 the recognition of two stereoisomers with opposing biological activity, 29 and the lack of regulation and appropriate controls contributed to an unreliability of results and an inability to translate findings into standard clinical care.
One of the first commercial and clinical uses of APO was to treat erectile dysfunction. During a study evaluating APO for treatment of alcoholism, the occurrence of spontaneous erections after 4–11 tablets was reported in 30–55% of subjects. 23 This led TAP Pharmaceutical/Abbot Laboratories to develop a SL APO form of the drug, prove its efficacy for erectile dysfunction (ED), and enter the European market in 2001 as Uprima. 30 In a parallel application, APO was also explored in women suffering sexual dysfunction in Argentina 31 and Italy, 32 but no product was brought to market. Five years after TAP's market launch, an observational cohort study using prescription event monitoring of prescribed APO in England questioned APO's overall efficacy, reporting 64.7% of patients stopped using APO because it was not effective for ED. Additionally, that study reported the most frequent adverse events associated with APO use were headache and nausea, effects most prominent in the first month and decreasing substantively over time. 33 As a result, the marketing permission was withdrawn for Ixense, 34 and the lack of a request for marketing renewal for Uprima 35 resulted in the commercial products being removed from the market in 2006.
While the clinical use of APO to treat sexual dysfunction was discontinued, its clinical application for the treatment of Parkinson's disease (PD) was advanced. The effectiveness of APO in the treatment of PD was first observed by Schwab in 1951, 36 and was confirmed by Castaigne et al. 20 years later. 37 The anti-parkinsonism activity was observed in the APO R enantiomer, which is a dopaminergic agonist, but absent in the S enantiomer, which appears to have an opposite dopaminergic antagonistic effect. 29 Fifty years after it was reported to exert an anti-parkinsonian effect, APO was submitted for formal approval to the Food and Drug Administration (FDA). 38 APO was approved in the United States in 2004 and released under the brand Apokyn for rescue subcutaneous (SC) injections or continuous delivery. APO SC remains the most effective dopamine agonist available for the treatment of PD.
Throughout its 170-year life, APO has been studied and prescribed for the treatment of widely diverse medical conditions, including its current clinical use for the treatment of PD. The remainder of this article reviews a series of studies that collectively suggest APO should be evaluated for repurposing as a tobacco dependence treatment therapeutic.
Apo for Tobacco Use Disorder: Neuromolecular Evidence
While the early clinical studies of APO for the treatment of drug abuse might suggest potential utility for treating tobacco use disorder, the overall lack of rigor in study design prevented these findings from being generalized in this way. An increasing body of neuromolecular and model organism research, however, is lending mechanistic support for APO's ability to impact addiction-related processes and potentially treat tobacco use disorder. APO has been shown to target the dopaminergic system directly, which plays a key role in the development and maintenance of drug dependency and addiction. As the following studies suggest, APO's potential for treating tobacco use disorder may lie in its ability to stabilize the nicotine-induced changes to dopamine signaling while also addressing the system hypersensitivity occurring during withdrawal (Fig. 1).
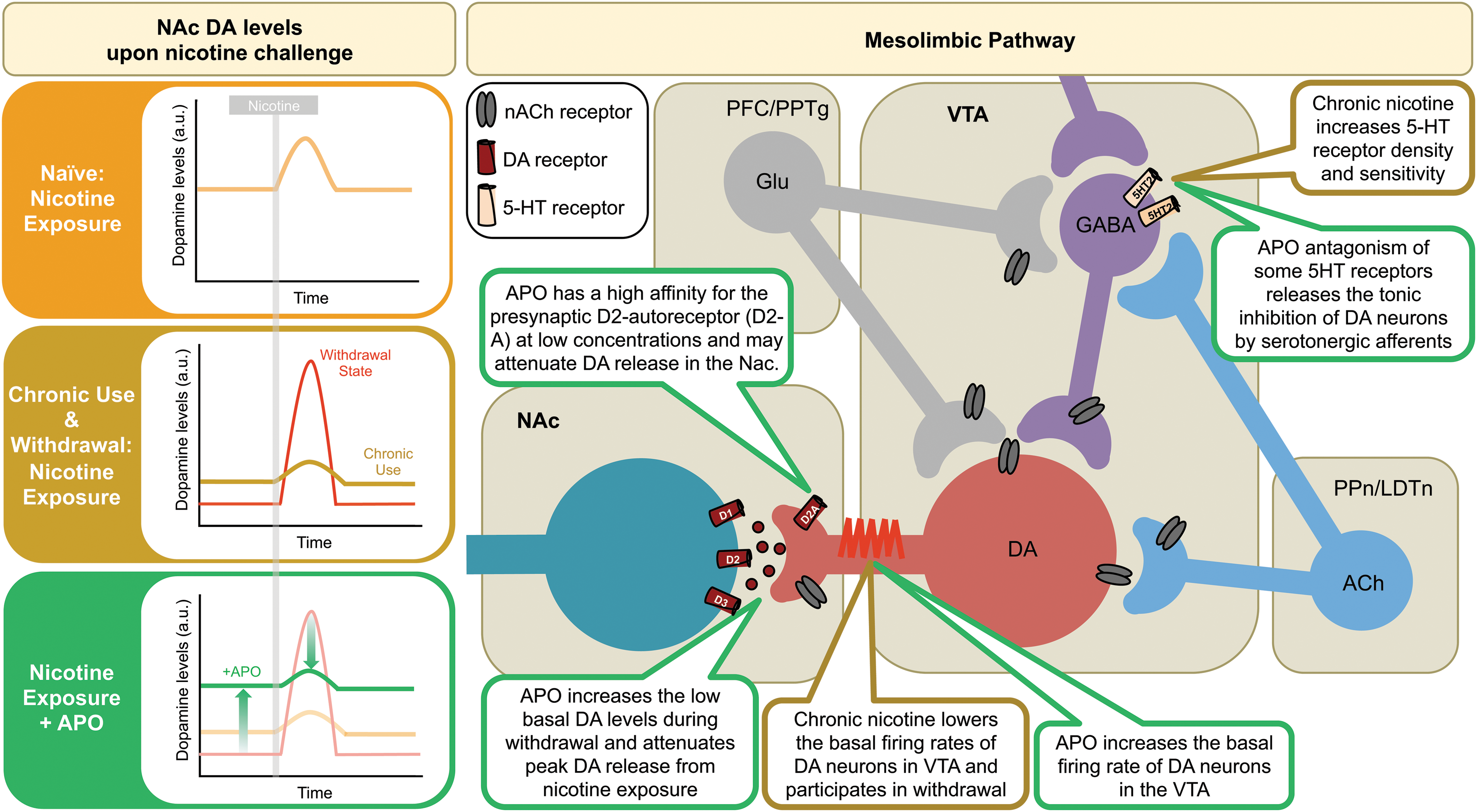
Acute and chronic nicotine exposures induce modified dopaminergic signaling within the mesolimbic pathway. At several points, apomorphine (APO) exposure results in a potentially corrective effect on the modified dopamine response, suggesting a potential therapeutic role for smoking cessation and nicotine withdrawal treatment.
Apo and the Dopaminergic System
The dopaminergic system mediates the rewarding effects of drugs of abuse, is intricately involved in the biological effects of nicotine, and has been extensively studied in the context of addiction. The system includes five dopamine receptors (Fig. 2), of which APO exerts varied levels of agonistic effects (Table 1). One study showed that acute nicotine exposure increases the average firing rate and burst firing of dopamine neurons in vivo, 39 and increases basal dopamine concentrations in the ventral tegmental area (VTA) and nucleus accumbens (NAc; Fig. 1), 40 considered important behavior reinforcement signals in rat and human models of nicotine dependence. 41 Tyrosine hydroxylase (TH) is an enzyme necessary for dopamine precursor synthesis, and TH-positive neuron firing patterns are increased upon nicotine challenge, also highlighting nicotine-induced changes to dopamine signaling.

Indirect Neuromolecular Evidence Supporting APO Repurposing for Tobacco Use Disorder
APO, apomorphine; +, agonist; –, antagonist; ?, activity in receptor unknown.
The first suggestion that dopaminergic agonists such as APO could be used to reduce drug cravings came with experiments demonstrating the importance of the VTA neurons in nicotine dependence under acute challenge. Following initial nicotine exposure, a majority of midbrain VTA dopamine neurons increase firing rates. 42 A study performed almost three decades ago showed that administration of 50–500 μg/kg of nicotine to rats produced a dose-related increase in the firing rate of ventral tegmental dopamine cells (A10) that was three times larger than the effect in the substantia nigra pars compacta dopamine cells (A9). 43 This study also demonstrated that APO administration (1 mg/kg IV) inhibited the activity of both types of dopamine cells after nicotine exposure. Furthermore, addition of haloperidol 44 and Zetilodin 43 (both DRD2 antagonists) reversed APO-induced inhibition of nicotine-induced activity to pre-APO activity values.
When compared with similar acute experimental conditions, chronic nicotine-treated mice show a decreased release of dopamine in the NAc 45,46 (Fig. 1) and have lower tonic and phasic dopamine release. 47 This observation is supported by in vivo brain slices of primates after self-administrated chronic nicotine exposure (650 μg/mL) for 8 months, demonstrating a decrease of the basal firing rate of dopamine neurons. 48 The overall decline in dopamine function is suspected to be responsible for the motivational deficits or anhedonic states in multiple drug dependencies. 49 These changes in dopaminergic transmission have also been linked in the rat model to differences between the aversive and rewarding properties of nicotine. Decreases in the VTA dopamine neuron activity observed to last 3–6 weeks post-exposure in rats is reversed by acute APO administration (20 μg/kg IV; Fig. 1). 50 Similarly, the APO effect in rescuing VTA dopamine cell population activity was also observed after prolonged cocaine, amphetamine, and ethanol exposure in the same model. 50 Increasing basal dopamine signal levels with APO may resemble the observed clinical benefit of physical exertion, which increases dopamine levels and reduces cigarette craving. 51 A functional magnetic resonance imaging study of a Chinese smoker suggests that activation of the mesolimbic dopamine pathway through self-expanding activities such as “falling in love” attenuate cigarette cue reactivity by creating an aroused affect. 52 This may suggest stimulation of the same reward pathway associated with self-expansion experiences, through the use of APO, can also help lessen reactivity to nicotine cravings.
Data from studies reporting on the effect of other dopamine agonists to address nicotine-induced changes may provide corollary evidence suggesting value in APO for treatment of tobacco use disorder. One study observed that administration of quinpirole, a DRD2 selective agonist, reversed the modified TH-positive neuron firing patterns observed after nicotine exposure (Fig. 1). 53 DRD3 also mediates responses to addictive drugs and polymorphisms in this gene having been significantly associated with nicotine dependence in European-American smokers, 54 as well as with packs per day and heaviness of smoking. 55 Co-activation of DRD2 and DRD3 with pramipexole attenuates nicotine withdrawal signs. 56 Use of a DRD3 agonist to counteract the rewarding response to addictive drugs is further supported by a methamphetamine-enhanced brain stimulating reward study, which showed that partial DRD3 agonist BP-897 reduced methamphetamine's rewarding effect. 57 While these studies support the use of a dopamine receptor agonist to block the effects of addictive drugs, addiction is a complex process, and at least one study suggested DRD3 selective antagonism could disrupt drug-seeking reinstatement cues. 58 Overall, however, inferences drawn from the parallel effects of APO on the DRD2 and DRD3 receptors suggest that APO may be beneficial in correcting nicotine-induced alterations of dopamine levels in smokers.
Several studies have linked genetic changes in the DRD4 receptor with smoking and smoking cessation treatment outcomes. Variations in DRD4 have been shown to affect a response to bupropion, 59 the status of smoking in a Caucasian population, 60 as well as the relationship between the intent to quit and smoking levels in adolescents. 61 However, how these genetic variants influence receptor activation (or inhibition) is not well characterized, making it difficult to understand the influence of APO in this context. Antagonism of DRD4 by L-745,870 has been shown to reduce reinstatement of nicotine-seeking behavior significantly. While APO is an agonist of this receptor, it has been shown that DRD4 agonism did not induce or alter nicotine-seeking behavior, 62 suggesting APO should not induce contrary effects at this receptor if used to treat tobacco use disorder. As for the DRD5 receptor, only one study has reported a significant association with nicotine dependence in highly nicotine dependent subjects. 63 SKF81297 (DRD1 and DRD5 receptor agonist) at 0.32 mg/kg reduced overall somatic signs of nicotine withdrawal (e.g., teeth-chattering/chews), while a 10-fold lower dose of 0.032 mg/kg did not. 56 This suggests an impetus for using a DRD5 agonist to mitigate nicotine withdrawal symptoms.
Preclinical behavioral models also suggest a possible role of APO for the treatment of tobacco use disorder. A novel larval zebrafish locomotor activation assay with established predictive clinical validity 64 was used to evaluate medications for nicotine-induced locomotion blockade. 65 Eight medications, including APO (1 μM), attenuated the nicotine response. Simultaneous administration of APO and varenicline improved the locomotion blockade, suggesting a potential use in alterative treatment strategies with lower doses of combined medications. 65 It must be noted that four decades ago, APO was shown to decrease the locomotor-stimulating effects of ethanol in rats with small doses (0.03–0.25 mg/kg administered intraperitoneally [IP]). 66 This is thought to be mediated through presynaptic DRD2 receptor activation at these low doses. Additionally, the synergism observed in the larval zebrafish locomotor model between varenicline and APO may very well be due to the fact that varenicline can increase DRD2 and DRD3 availability. 67
The compendium of data across multiple studies suggests APO may be capable of restoring the modified DA signaling, including restoration of the basal low tonic DA levels to normal levels and the modulation of firing patterns of cell populations that play a role in neuronal signaling associated with drug reinforcement.
Apo and Serotonergic Signaling
APO is primarily a dopaminergic targeting compound that accounts for many of the potential values as a tobacco use disorder medication. However, APO also possesses established activity against serotonergic receptors, which can act on dopamine neurons. While the specific effects of APO on the serotonergic system is less well defined, there are some findings that could suggest advantages in addressing the multifocal landscape of effects associated with tobacco use disorder. To this end, the existing literature on APO's interactions with the serotonergic system is briefly summarized.
APO targets four serotonergic (5-HT) receptors (Fig. 1), including 5-HT2A and 5-HT2C, which are postulated to modulate nicotine withdrawal. The 5-HT2A receptor is prominent in the striatum, in the NAc, 68 and in both dopaminergic and non-dopaminergic VTA neurons. 69,70 Cessation of repeated nicotine administration results in increased sensitivity to 5-HT2 receptor systems and decreased 5-HT turnover, which are phenomena implicated in nicotine withdrawal. 71 It has been shown that 5-HT2A located in post-synaptic dopamine neurons may play a permissive role in the sensitizing effects of nicotine. 72 In addition, nicotine withdrawal evokes an increase in the number of 5-HT2A receptors in VTA and a reduction in in the 5-HT2A receptor transcript level as an auto-regulatory response to the increased receptor density in the hippocampus and VTA. 73 APO is a 5-HT2A antagonist, which may attenuate the nicotine withdrawal effects associated 5-HT2A sensitivity and provide a novel approach to preventing nicotine-seeking reinforcement cues. This theory, however, is partially contradicted by an observed decrease in the reinforcement effects of nicotine in rats when 1-(2,5-dimethoxy-4-iodophenyl)-2-aminopropane (mixed agonist of 5-HT2A/C) is administered. 74
The 5-HT2C receptor is located on both VTA GABAergic and dopaminergic neurons. 75 During nicotine withdrawal, there is attenuation of mRNA editing of 5-HT2C receptor in the hippocampus, resulting in a population of less edited (and thus more active) receptors. APO is a 5-HT2C receptor antagonist. One study demonstrated that 5-HT2C receptor antagonist SB242084 increased basal firing rates of dopamine neurons in the VTA, suggesting a tonic dopaminergic inhibition of serotonergic afferents. 76 In the context of the hypo-dopaminergic state present in a patient during withdrawal, this may represent a second path to increase the dopamine neuron activity and alleviate the anhedonic state. However, much like 5-HT2A, the role of this receptor in tobacco use disorder is complex. Conversely, 5-HT2C stimulation may also be beneficial, as activation of this receptor by Ro 60-0175 77 and lorcaserin 78 in rats reduces the dopamine released in NAc and the frontal cortex, provoking a reduction in nicotine self-administration and hyperactivity. APO modifying effects on serotonergic signaling may influence dopamine-mediated nicotine response, but require considerable more study before drawing conclusions regarding the advantages or disadvantages with regards to treatment of tobacco use disorder.
APO and Nicotine Withdrawal
Nicotine withdrawal manifests as a collection of emotional and somatic symptoms that emerge a few hours after nicotine abstinence in individuals who are chronically exposed. The most common symptoms of withdrawal include irritability, frustration, insomnia, anxiety, and depression. Symptoms typically peak within the first week of abstinence and taper off in the following 3–4 weeks. 79 Nicotine withdrawal has been observed in rats at 2 and 7 days after the termination of a constant 14-day infusion of nicotine. 45 Significantly lower basal dopamine levels are observed in the NAc of mice for at least 5 days after a 25-day self-administered nicotine infusion. 80 This latent hypo-dopaminergic state is thought to cause anhedonia during withdrawal. 81 Also, during abstinence, a single nicotine exposure amplifies the number of dopamine pulses within a burst resulting in a stronger effect than that observed during chronic nicotine exposure (Fig. 1). 47 Such observations may explain why the majority of people who attempt to quit smoking unaided by pharmacologic agents relapse within the first 2 weeks. 82
Several studies have reported findings suggesting that APO ameliorates some of the physiological symptoms associated with withdrawal. APO (20–200 ng) injected alongside nicotine directly to the ventral hippocampus blocked the anxiogenic response induced by nicotine in rats. 83 This study aimed to determine the anti-anxiogenic properties of APO after it was reported earlier that systemic administration (0.5 mg/kg IV) to rats induces an anxiolytic-like effect measured by open-arm time, specifically through the DRD2 receptor subtype. 84 Even though evidence exists that co-activation of DRD1- and DRD2-like receptors can reinstate cocaine-seeking behavior in rats, 85 APO (1 and 5 μg) or a mixture of SKF82958 (DRD1-like receptor agonist) and quinpirole (DRD2-like receptor agonist) has been shown to attenuate a morphine withdrawal–induced startle response. 86 Similarly, APO was shown to relieve nicotine withdrawal–induced startle and morphine withdrawal–conditioned place aversion. 86 Nonetheless, while reports attribute a potential valuable effect of APO for tobacco use disorder treatment, a limitation in these in vivo studies is the use of supra-therapeutic concentrations of 0.03–1 mg/kg (human therapeutic plasma levels are beneath 100 ng/mL). In addition, direct injections to brain regions range in the micrograms when human therapeutic levels in the brain are estimated to be a tenth of those reported in plasma. Thus, in order for APO to be validated as a tobacco use disorder treatment, its efficacy needs to be assessed within currently approved physiologic doses in humans.
Apo and Weight Loss
Weight gain is a well-recognized consequence of smoking cessation. Smokers gain an average of 5–10 pounds in the months following smoking cessation, 87,88 with heavier and more dependent smokers gaining more weight. 89 –91 Mean weight gain after smoking cessation may be as much as 13 pounds at 1 year 92 and 21 pounds over 5 years. 93 One of the reasons that individuals initiate smoking and continue to smoke is the perception that smoking helps them control their body weight. 94 –99 Actual weight gain following smoking abstinence has also been associated with subsequent relapse to smoking. 100 In a large population-based study, 52% of women and 32% of men with a previous quit attempt reported that weight gain was one of the reasons for relapse. 101 The impact of sex on smoking abstinence outcomes has been mixed, 102 –107 with some data suggesting that women may be less likely than men are to be successful in maintaining smoking abstinence. 102,106,108,109 However, both male and females smokers have weight concerns. In a prospective evaluation of a large sample of smokers, 47% of female smokers and 22% of male smokers were classified as having weight concerns. 95 Medications attenuating weight gain after smoking cessation could play a significant role in the clinical treatment of weight-concerned smokers.
Like other DRD1 and DRD2 agonists, APO decreases food intake and body weight in rats treated twice a day with a high dose. This anorexigenic effect lasts for 4 days in streptozotocin-induced diabetic rats and wild-type rats after APO administration. 110 APO treatment (2 mg/kg and 4 mg/kg IP) decreases food intake in a dose-dependent manner for a 5-day period in rats. 111 Recently, the mechanism for such an anorexic effect was demonstrated to be driven by dopaminergic neurons that also express the ghrelin receptor, GHSR1a. Ghrelin is a peptide produced in the gastrointestinal tract that acts in the hypothalamus to increase hunger and acid secretion in the stomach for food intake. In cells co-expressing the GHSR1a and DRD2 receptors and treated with cabergoline (DRD2 agonist), a dose-dependent suppression of food intake occurred. This was dependent on GHSR1a and DRD2 allosteric interactions as shown by fluorescence resonance energy transfer assays. Antagonism of the anorexigenic effect of cabergoline by JMV2959 (GSHR1a neutral antagonist) is not dependent on endogenous ghrelin but on the presence of GHSR1a, illustrating the physiological relevance of GHSR1a and DRD2 interactions. 112 Of note, it has also been shown that pharmacological blockade of GHR-Rs with JMV2959 blocks nicotine-induced locomotion, 113 the induction of conditioned place preference by nicotine, and dopamine overflow within the NAc. 114 Thus, the use of APO may target a behavioral change in food intake during smoking cessation using the interaction between ghrelin receptors and dopaminergic pathways. However, this effect may be dependent on the dose of APO prescribed. Current APO doses used for PD are approximately 10–50 times lower than concentrations used in these experiments.
Apo Administration and Therapeutic Delivery
APO requires parenteral administration for the current treatment of advanced PD due to the pharmacokinetic challenges of 1.7% bioavailability after oral administration following first-pass hepatic metabolism. 115 Currently approved doses for DA-deficient PD patients via the SC route target 2–6 mg/dose within a 20 mg daily threshold. Based on experimental pharmacological data in wild-type rhesus monkeys treated with positron emission tomography radioligands, such doses yield approximately 20–50% of DRD2/DRD3 receptor occupancy. A disadvantage of this approach is the appearance of SC nodules and ulcers 116 at the injection site in up to 10% of patients after long-term use. 117 Rectal administration has showed a mean bioavailability between 14.7% and 40.2%, but is not a practical method for smoking cessation treatment. Intranasal administration may be promising due to similar pharmacokinetics to the subcutaneous approach. Recently, a randomized placebo controlled Phase IIa study demonstrated the safe absorption of APO through the nasal route with peak plasma concentration at 2–7 min. 118
APO is also rapidly absorbed sublingually, reaching a peak plasma concentration (C max) in 30–60 min. In vitro plasma protein binding estimates that APO is primarily protein bound (approximately 90% to albumin), and maximum concentrations in cerebrospinal fluid are <10% of maximum plasma concentrations. APO possesses a half-life of 40 min with total elimination occurring in 5 h. Bioavailability of SL APO is estimated to be 16–18% of that reached SC. 119 This SL approach opens a broad variety of possible interventions. First, it may embody a novel approach for smoking cessation that targets cravings, and during an episode of relapse may mitigate the chemical reinstatement cues. Second, based on the synergism described in previous sections, it can be used concomitantly with other currently approved therapies, such as varenicline, addressing multiple aspects of the pathophysiology of withdrawal and addiction preservation.
The pharmaceutical company Cynapsus holds a patent for a thin-film SL delivery method (APL-130277), and has demonstrated a pharmacokinetic profile that compared favorably to injected APO with a mean T max of 25 min and good tolerability. This company aims to compare the pharmacokinetic profile of APL-130277 to SC APO in healthy subjects and further move to prove the efficacy of this less invasive method in PD patients. 120 This approach has shown favorable results managing off episodes (reemergence of PD symptoms after long-term Levodopa use) in a small Phase 2 study of PD patients, and the company is pursuing Phase III trials. 121 If the potential of APO is proven to have smoking cessation efficacy, this SL thin-film delivery method has the potential for high adherence in smokers. To maintain specific plasma levels of APO to raise DA levels in the central nervous system and prevent reinforcement cues, the interventions could be controlled by the smoker to target the cravings experienced during withdrawal.
Side Effects of Apo
Before significant effort is made to evaluate APO for repurposing for the treatment of tobacco use disorder, its side-effect profile needs to be understood and weighed against possible future patient use and benefit. Fortunately, throughout APO's long history of use, safety and side-effect data have been captured and well documented.
The most common side effects known to be caused by SC APO are yawning, dizziness, and nausea, which decrease with long-term use. 38 Tolerance can be prevented by ensuring a 4 h delay between each dose. Some of the most common side effects, such as nausea, have been safely prevented with a peripheral DRD2 receptor antagonist such as domperidone. 122 In addition, QTc prolongation, orthostatic hypotension, and cardiac events have been reported. However, recent evidence from an in vivo canine model with 1 mg/kg IV administration of APO over 10 min showed neither prolongation of the QT interval nor induced Torsade de Pointes. These data suggest that APO may possess a wide margin of cardiovascular safety contrary to common side-effect reports and warnings. 123
Important to the idea of using APO for smoking cessation, the only reports of potential liability for addiction and psychosis occurred in the context of high-dose combined therapeutic use and/or long-term consumption. Two case studies examined the effects of simultaneous injection of levodopa with APO and long-term APO monotherapy inciting potential addiction and psychosis in five patients. In these cases, patients were on high-dose APO regimens and proceeded to self-escalate dosing, resulting in psychosexual disorders. 124,125 The highest risk for APO-induced psychosis is in a small number of patients characterized by self-medication and addiction to dopaminergic drugs. 126,127 This raises the possibility, albeit rare, that high-dose APO use could elicit a liability for addiction and would need to be carefully monitored in any repurposed use of APO. However, no reports exist of addiction following low-to-moderate APO dosing. Based on these data, APO appears to possess a relatively benign side-effect profile, but targeted studies will be needed to assess the relative safety of its use in patients with potential confounding cardiovascular disease.
Conclusion
A significant body of knowledge surrounding the effects of APO administration exists, which, when assembled in the context of tobacco dependence and cessation, suggests the possibility of repurposing this drug for this indication. The concepts for how APO may correct modified dopamine levels associated with chronic nicotine use and nicotine withdrawal are conceptually described in Figure 1. Elevating the background dopamine signal with SL APO during the quitting process may remove multiple barriers for maintaining tobacco abstinence and combat the cravings that drive relapse. APO may stabilize a disrupted dopaminergic system that maintains an anhedonic state and may reverse a latent hypersensitivity during tobacco withdrawal.
Several observations regarding potential dose-dependent effects of APO can be extrapolated from existing studies. At higher doses, it has been shown to act post-synaptically to stimulate locomotor activity, which provides the therapeutic effect in the treatment of PD. 128 At lower doses, APO has a higher affinity for the presynaptic auto-receptor reducing dopamine release and inducing hypomotility, 129 an effect that may reduce the chemical burst that addresses drug-seeking behavior. APO is also reported to possess potent sedative properties and possible liability for addiction and psychosis at higher doses, 128 observations that further favor its use in low doses to treat tobacco use disorder. This dose-dependent effect has not been fully studied in humans, however, and will require further clinical studies.
APO also has the capacity to modulate altered serotonergic pathways involved in withdrawal symptoms. It is hypothesized that apart from restoring important cell population activity and preventing reinforcement cues, APO might also provide secondary effects associated with preventing weight gain associated with smoking cessation. Repurposing of APO for the treatment of tobacco use disorder will likely require lower dose regimens than those currently approved by the FDA for treating PD. The administration via an innovative SL approach may also expand current pharmacological cessation strategies. Therefore, APO represents a novel, accessible, and rational pharmacologic agent that is worth of consideration for repurposing as a medication for the treatment of tobacco use disorder to expand the armamentarium clinicians have to combat the tobacco epidemic.
Footnotes
Acknowledgments
We would like to thank Stephen Ekker for his input and guidance on the compilation of the work within this manuscript. We would also like to thank the Mayo Clinic, Clinical Translational Science program for their support thru the University of Puerto Rico Medical School Summer Scholar Program.
Disclosure Statement
J.O.E has received grant funding from Pfizer, Takada, NIH, and DOD outside the submitted work.