
Abstract
Candida albicans and Candida glabrata are two important human pathogens associated with high mortality. The anti-Candida potential of an antihypertensive drug, amlodipine besilate (AB), was studied against 10 strains of Candida, including 8 clinical isolates. AB is an inhibitor of voltage-gated Ca2+ channel (VGCC) of mammals. CCH1 expresses in a part of Ca2+ channel of Candida, which is a homologue of α subunit of mammalian VGCC. In plate assays, all strains of Candida showed sensitivity to AB on agar media at 256 μg/mL concentration, AB caused lethality at concentrations of 16 and 64 μg/mL in clinical isolates of C. glabrata and all strains of C. albicans, respectively. Minimum fungicidal concentration (MFC) values of AB varied for different strains. The clinical isolates of C. glabrata turned out to be more susceptible to AB than those of C. albicans. At 16 μg/mL, AB showed reduction of biofilm in the range of 41.51%–79.66% for C. glabrata strains and 32.00%–54.06% for C. albicans strains. AB has shown potential antifungal properties against the laboratory strains and clinical isolates of C. glabrata and C. albicans. In conclusion, AB exhibited potential antifungal properties against planktonic form and biofilm of C. glabrata and C. albicans. It was more effective against C. glabrata than against C. albicans in vitro.
Introduction
Incidence of Candida causing infections is growing worldwide due to increased practices of antibiotics, central venous catheter, parenteral nutrition, etc. especially in immunocompromised patients (AIDS, neutropenia, hematological malignancies, cancer, organ transplantation, etc.). 1,2
In the United States, candidemia infection is the fourth most common cause of hospital-acquired blood stream infection (BSI) and in Europe it ranks between 6th and 10th position. 3,4 In a study on 7,087 ICU patients from 75 countries by a group of investigators, Candida stands on the third position with infection rate of about 17%. 5 In a 16-year surveillance study, 394 cases of candidemia per 10,000 admissions have been reported from an Italian hospital where Candida albicans was present in 44.2% cases, followed by Candida parapsilosis and Candida glabrata. 6 A surveillance study from a Mexican tertiary care center on BSI revealed that C. albicans (46%) and Candida tropicalis (26%) were dominant among other species, whereas C. glabrata was more prevalent in diabetic and old age persons. 7 Non-albicans Candida (NAC) species were predominant in HIV seropositive patients admitted at HAART center in Gujarat, followed by C. albicans. 8 In another study from Maharashtra, a total of 523 isolates were identified as C. albicans (36.7%), C. tropicalis (35.1%), C. glabrata (28.1%), and Candida krusei (16.3%). 9 The rate of medical device-associated infections was reported to be 2.1 per 1,000 devices a day in a tertiary care hospital in Maharashtra state of India. 10 The prevalence of NAC has also been reported in neonates in Uttarakhand state of India. 11
Although C. albicans is dominant among other species in the clinical samples, the epidemiology of Candida-caused infections is now shifting worldwide from albicans to NAC species. 12,13 Members of NAC species are emerging as predominant pathogens in the cases of mucocutaneous and disseminated infections after C. albicans. 14 In a previous study, C. glabrata was predominant among NAC members, in case of oropharyngeal and vulvovaginal infections. 9 In past few years, the isolates of C. glabrata have shown resistance to azole and echinocandin drugs. 15 Rising resistance in clinical isolates of C. albicans and C. glabrata to existing antifungal drugs has attracted the attention of researchers to explore effective antifungal drugs. 16 The approach of drug repurposing (also known as drug repositioning) is applied to find out new indications of existing drugs, which has been implemented by various groups across the globe for the development of antifungal or anti-Candida drugs. 17 –20 Derivatives of 1,4-dihydropyridine have been reported to be effective against planktonic growth of several bacteria and fungi, especially Aspergillus fumigatus and C. albicans. 21,22
Amlodipine besilate (AB) (1,4-dihydropyridine) is a well-known calcium channel blocker that acts on L- and N-type calcium channels in mammals. 23 Calcium ion (Ca2+) channels are essential for the regulation of cell cycle, sporulation, hyphal morphogenesis, and pathogenesis. 24 –27 In mammals, voltage-gated calcium channels (VGCCs) play a central role in various physiological functions, hence are the promising target for therapeutics. 28 –30 Members of Ca2+ homeostasis pathway (calcium–calcineurin signaling pathway) have been suggested as potential targets for the development of new antifungal drugs. 31 Yeast Cch1 is a homologue of α1 subunit of mammalian VGCC and plays an important role in Ca2+ uptake along with regulatory integral plasma membrane protein, Mid1. 32 –34 A similar Ca2+ channel protein has also been verified in C. glabrata, that is, CgCch1. It has also been reported that cch1/mid1 mutants of C. glabrata are defective in Ca2+ uptake and lose viability upon prolonged exposure to fluconazole. 35 Previous studies have reported antimicrobial, antileishmanial, and anticancer activities of amlodipine. 36 –39 A recent study has shown the antifungal properties of amlodipine, against C. albicans, in combination with fluconazole. 40 An in silico study has also exhibited the docking potential of AB against CgCch1. 41
In this report, we have documented the anti-Candida properties of a Ca2+ channel blocker against two most prevalent Candida species, C. glabrata and C. albicans.
Material and Methods
Strains, Reagents, and Growth Conditions
Total 10 wild type strains including two reference strains, C. glabrata ATCC 90030 (procured from Institute of Microbial Technology), C. albicans ATCC MYA-2876 (thankfully provided by Prof. K. Ganesan, IMTECH), and eight clinical isolates (four of each C. glabrata and C. albicans, obtained from Department of Microbiology, Shri Guru Ram Rai Institute of Health and Medical Sciences, Dehradun, Uttarakhand, India) were used in this study. Reference strains of C. albicans and C. glabrata are represented as CA and CG, respectively, henceforth. Clinical isolates of C. glabrata and C. albicans are represented as CCG1, CCG2, CCG3, CCG4 and CCA1, CCA2, CCA3, CCA4, respectively, in the figures and text. The culture was maintained at 37°C in YPD media (1% yeast extract, 2% dextrose, 2% peptone, and 2% agar for solid media). For planktonic growth and mature biofilm assays, log phase culture was diluted in RPMI-1640 medium (mentioned as RPMI henceforth). XTT [2,3-bis-(2-methoxy-4-nitro-5-sulfophenyl)-2H-tetrazolium-5-carboxanilide] sodium salt, phosphate-buffered saline (PBS), menadione, YPD, fluconazole, and RPMI were procured from Himedia. AB was thankfully given by a pharmaceutical manufacturer, Vilin Bio Med Ltd.
Effect of AB on Growth
The spotting assay was performed for investigating the effect of AB upon the growth. 42 In brief, log phase cells of C. glabrata, C. albicans, and clinical isolates (OD600 nm: 0.60) were spotted in 10-fold serial dilutions (104, 103, 102, and 101) onto the YPD plates, containing AB at a log2 concentration range starting from 64 to 512 μg/mL along with a control plate with no drugs. The plates were incubated at 37°C for 18 h before being photographed.
Antifungal Susceptibility Test
Susceptibility of Candida strains to AB was determined in RPMI media as per CLSI, M27-A2 guidelines for broth microdilution assay. 43,44 Log phase cells (OD600nm: 0.8) were diluted to have 2.5 × 103 cells/mL, and 100 μL of it was added into each well of a 96-well microtiter plate containing log2 concentration range 0.5–512 μg/mL of AB, along with a control well with no drug. Plates were incubated at 35°C for 48 h. After incubation, wells of the plate were analyzed for growth by taking OD at 600 nm. Reading of the media blank was subtracted from test readings and a line graph was plotted between OD600nm (Y axis) and concentration of drug (X axis).
In addition, minimum fungicidal concentration (MFC) of AB was determined for all strains, as described previously with few modifications. 45 In brief, 5 μL cultures from each well of a 96-well microtiter plate were spotted onto the YPD plate. Plates were then incubated at 35°C for 18 h before being photographed.
Effect of AB on Preformed Biofilm
The biofilm was developed in the 96-well flat bottom plates in RPMI. 44 In brief, log phase culture was diluted to 107 cells/mL in PBS. The 100 μL of cell suspension was added to each well and plates were incubated at 37°C for 90 min. After incubation, wells were washed with 200 μL of PBS and 200 μL of RPMI was added to each well. Plates were incubated at 37°C for 24 h with shaking for biofilm formation. Furthermore, wells were washed twice with 200 μL of PBS. To each well, 200 μL fresh RPMI containing log2 concentration range of AB (0.5–16 μg/mL) was added along with a control well with no drug; plates were incubated again at 37°C for 24 h with mild shaking. After incubation, the biofilm was quantified by XTT reduction assay and metabolic activities of biofilm were expressed in terms of absorbance at 600 nm. Reading of the reagent blank was subtracted from test readings and a line graph was plotted between OD600 nm (Y axis) and concentration of drug (X axis). Relative reduction in metabolic activity of the biofilm at the highest concentration (16 μg/mL) was estimated as percentage reduction in the OD600 nm of the biofilm after exposure of drug when compared with control biofilm (without any drug). Statistical differences in the biofilm activities were compared with the biofilm of respective control (without any drug).
Statistical Analysis
Mean of three values of OD600 nm in broth microdilution assay and the assays for biofilm activity are shown along with standard deviation. Student's t-test was applied for analyzing the significant differences between the values of biofilm activities. P values <0.050 and <0.001 were taken as significant (“*”) and highly significant (“**”), respectively.
Results and Discussion
Several epidemiological studies have indicated that C. glabrata stands second after C. albicans among the Candida members for causing candidiasis worldwide. 12,13 The anti-Candida property of AB was tested against reference strains and clinical isolates of C. albicans and C. glabrata. Amlodipine is an inhibitor of mammalian VGCCs (a homologue of Candida, Cch1).
AB Inhibited Growth of Candida
In the spotting assay, Candida species appeared susceptible at 256 μg/mL (and above) of AB (Fig. 1 and Supplementary Fig. S1). AB is a well-known antihypertensive drug that acts by binding and inhibiting mammalian VGCC. 23 In recent studies, AB has also been proven to possess antibacterial activity. 36,46 AB appeared to be lethal for both species of Candida (Fig. 1) because AB is known to affect intracellular Ca2+ by reducing its uptake.

Spotting assay on YPD plates with AB. Log phase cells of C. glabrata
Antifungal Susceptibility Test
Antifungal susceptibility of AB was analyzed in RPMI broth, following CLSI guidelines. In general, all strains showed a decrease in growth in a dose-dependent manner (Fig. 2 and Supplementary Fig. S2). The minimum inhibitory concentration (MIC) of fluconazole varied for different strains (Supplementary Table S1 and Supplementary Fig. S3; Supplementary Data are available online at
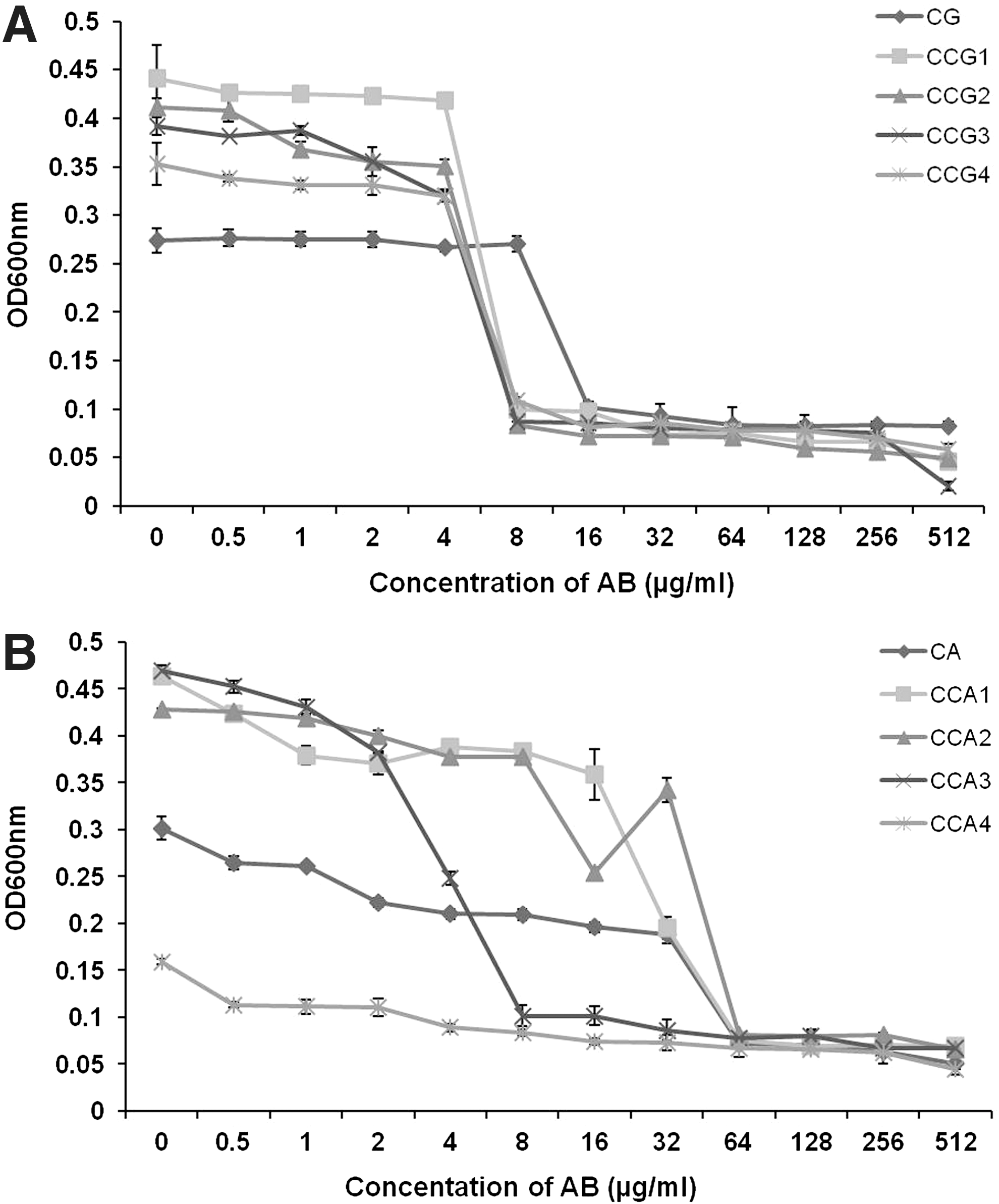
Antifungal susceptibility assay of Candida strains. AB, in the given concentrations, was tested in RPMI against Candida glabrata and its clinical isolates
Among all C. glabrata strains, CG was found to be the most resistant to AB, whereas the clinical isolates of C. glabrata were found to be relatively sensitive (Fig. 2A). CCA3 appeared to be the most sensitive to AB followed by CCA4 and CCA1, whereas CA and CCA2 were found more resistant than other C. albicans strains (Fig. 2B).
All strains of C. albicans and C. glabrata were analyzed to determine the fungicidal effect of AB (Fig. 3 and Supplementary Fig. S4). In the given range of AB concentrations, CG showed MFC of AB between 256 and 512 μg/mL, whereas MFC of AB for CCG1, CCG2, CCG3, and CCG4 was reported to lie between 8 and 16 μg/mL (Table 1). The MFC of AB for the strains of C. albicans was found as 16–32 μg/mL for CCA3, 32–64 μg/mL for CA, CCA1, and CCA4, and 64–128 μg/mL for CCA2 (Table 1). An independently produced second set of data of MFC values is given in Supplementary Table S2.

Fungicidal activity of AB. Log phase cells of C. glabrata
Minimum Fungicidal Concentrations of AB Against Different Strains of Candida
AB, amlodipin besilate; CA, reference strain of Candida albicans; CCA, clinical isolates of C. albicans; CCG, clinical isolates of Candida glabrata; CG, reference strain of C. glabrata; MFC, minimum fungicidal concentration.
Based on the antifungal susceptibility test and MFCs, AB has emerged as a better antifungal agent against C. glabrata strains, whereas fluconazole showed better antifungal activities against C. albicans. C. glabrata is naturally resistant to azoles due to the presence of less affinity to lanosterol 14 α−demethylase (Erg11p), inherent mechanism for the upregulation of ERG11 (for ergosterol biosynthesis) and ABC transporters (for increased drug efflux). 47 Our results are in agreement with the findings of Liu et al., 40 where it has been shown that AB alone is not much effective against the planktonic cells of C. albicans. 40 Another study has shown that CCH1 mutant of C. glabrata is more susceptible to the azole drugs. 35 AB is a known inhibitor of Ca2+ channel and has shown good affinity with C. glabrata Cch1p, which may result in low Ca2+ uptake. 41 Calcium ion is an important secondary messenger that regulates several intracellular pathways and ultimately responsible for the cell fitness and virulence of fungal pathogens. 48,49 The importance of Ca2+ has been depicted in other fungi also; absence of CCH1 or MID1, causing limiting intracellular Ca2+, has resulted in the loss of viability in Cryptococcus neoformans. 50
AB Reduced Preformed Biofilm
Fungal biofilm, an important clinical manifestation, is more resistant to the antifungals than planktonic cells by virtue of its organized structure. 51 C. glabrata biofilm has been reported to be azole resistant, in vivo. 16 Upon exposure to AB, mature biofilm of all strains of C. glabrata has shown dose-dependent decrease in the metabolic activities (Fig. 4A). In the absence of drug, CCG1 showed the highest biofilm activity among all Candida strains, even better than that of CG, whereas other clinical isolates of C. glabrata (CCG2, CCG3, and CCG4) revealed biofilm activities significantly lower than that of reference strain (Fig. 4A). Relative reductions in biofilm (at 16 μg/mL AB) were reported to be 48.96%, 79.66%, 44.24%, 50.00%, and 41.51% for CG, CCG1, CCG2, CCG3, and CCG4, respectively (Table 2).
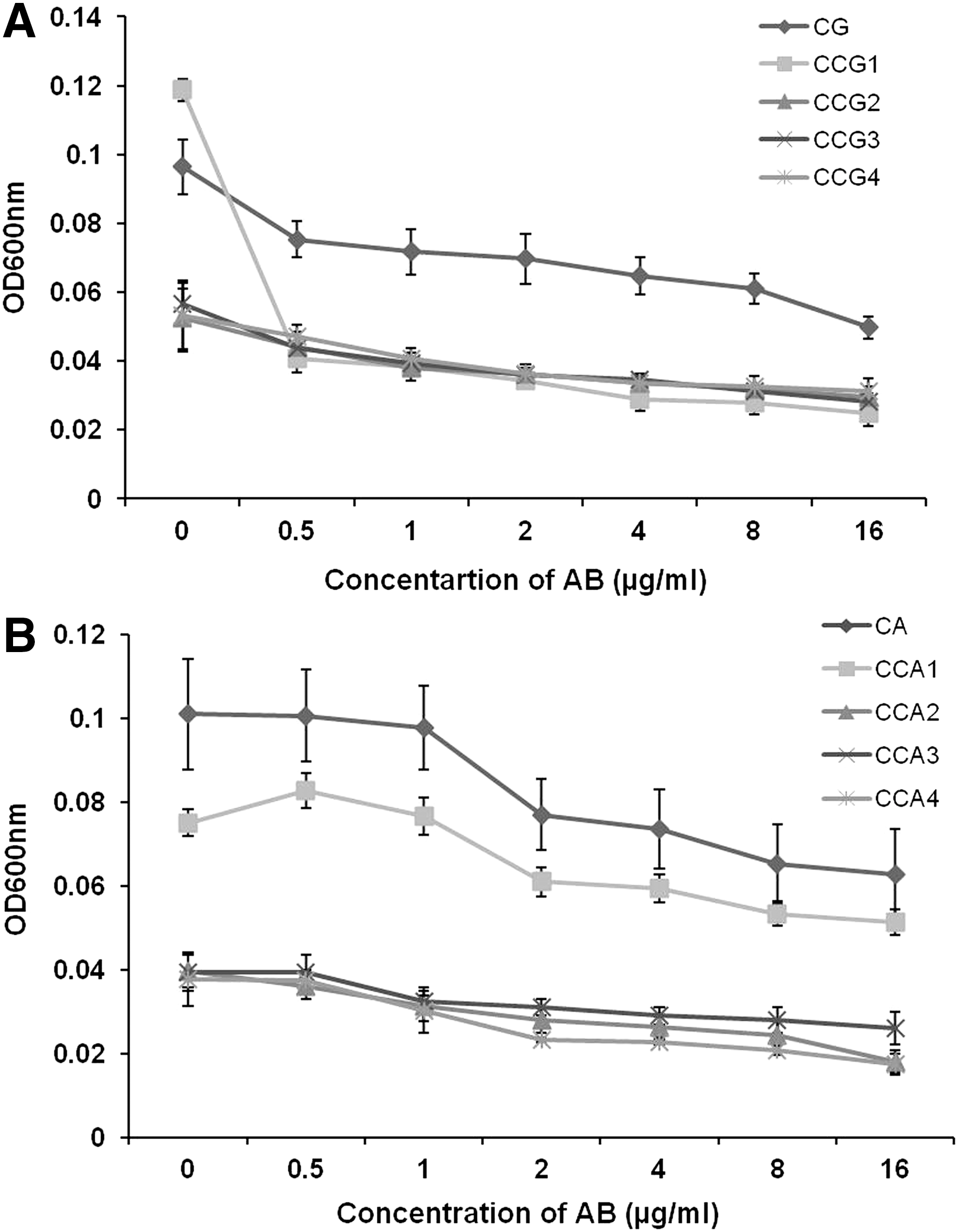
Effect on preformed biofilm of Candida. C. glabrata biofilm
Relative Reduction in Metabolic Activities of Candida Biofilm upon Exposure to AB
RRMA, relative reduction in metabolic activity.
C. albicans strains have also shown concentration-dependent decrease in biofilm activities upon exposure to AB (Fig. 4B). In the absence of drug, CA showed the highest biofilm activity among all strains of C. albicans. Even in the absence of drug, clinical isolates (CCA1, CCA2, CCA3, and CCA4) exhibited biofilm activities markedly lower than that of reference strain. Relative reductions in biofilm of C. albicans (at 16 μg/mL AB) were reported in the range of 32.00%–54.06% (Table 2). An independently produced second set of data of relative reduction in metabolic activities of Candida biofilm upon exposure to 16 μg/ml AB is given in Supplementary Table S3.
Our results indicated that AB significantly reduced the preformed biofilm of C. glabrata and C. albicans in a concentration-dependent manner (Fig. 4). This reduction in the biofilm activities could be credited to the reduced Ca2+ uptake, resulting in defective cell physiology and virulence. It has been shown earlier that mutants of A. fumigatus, defective in calcium channels, lose virulence in murine model. 52 In Aspergillus nidulans, calcium ion channels are also reported to regulate the pattern of growth and cell wall components. 27 Cell wall components provide a platform for adhesion and biofilm formation over the surfaces; therefore, blocking of Ca2+ channel by AB may reduce the biofilm. Further studies are required to reveal the mechanism behind the reduction in growth, viability, and biofilm activities upon exposure to AB, by looking at AB-mediated alteration in expression of genes related to virulence (adhesion and biofilm).
To our knowledge, this is the first report on the effect of AB against preformed biofilm of C. albicans and C. glabrata, demonstrating its therapeutic potential in clinics. AB can readily be developed as a drug against superficial and invasive candidiasis, as repurposed drugs need not undergo toxicity studies, saving time and cost.
In conclusion, AB has shown anti-Candida activities against planktonic and biofilm forms of C. glabrata and C. albicans. It is inhibitory for the growth of C. glabrata and C. albicans in plate assays. AB showed better inhibition of C. glabrata strains than C. albicans in antifungal susceptibility assays and is found to be fungicidal at lower concentrations. AB has significantly reduced the preformed biofilm of all strains of C. glabrata and C. albicans, but exhibited better results against the biofilm of C. glabrata strains. Hence, AB has substantial antifungal potential against the planktonic form and biofilm of different strains of C. glabrata and C. albicans, including clinical isolates.
Footnotes
Acknowledgments
We are thankful to Vilin Bio Med Ltd., Roorkee, Uttarakhand, India, for providing amlodipine besilate used in this study. P.G. is supported by INSPIRE fellowship from the Department of Science and Technology, Government of India. We are thankful to Miss. Pramila Kothari, MSc dissertation student and Mr. Haseen Ahmad, a MTech trainee, for their help during initial work. The contribution of Ms. Rupinder Kaur, Professional Communication Department, Graphic Era University, is acknowledged for checking grammar and punctuations. We acknowledge the support of the Director, Defence Institute of Physiology and Allied Sciences (DIPAS), DRDO, Delhi-54 along with Dr. Amitabha Chakrabarti, Sc. ‘E’ and Dr. R.C. Meena, Sc. ‘C’, DIPAS, for allowing us to conduct some experiments in their laboratory. We are also thankful to Prof. L.M.S. Palni, Dean, Biotechnology and Prof. Ashish Thapliyal, Head, Biotechnology, Graphic Era University, for his constant support during the course of this study.
Disclosure Statement
No competing financial interests exist.