
Abstract
Intra-articular injection of drug depots is considered as a therapeutic strategy for the treatment of osteoarthritis. In this study, we designed an in vitro assay in a previously described bioreactor system to evaluate the uptake of a small molecule drug mimic as a function of drug clearance by the synovium and compressive load. Bromophenol blue (BPB) loaded hydrogels were placed on top of bovine articular cartilage explants and were compressed in a dual flow bioreactor. As a control, BPB was directly injected in the bioreactor compartment mimicking the synovial fluid. Subsequently, diffusion coefficients of the dye were estimated based on Fick's law. Mimicking synovial clearance revealed that dye penetration of BPB when released from a drug delivery system placed on top of a cartilage explant was enhanced compared to direct injection of BPB into a simulated synovial fluid. Furthermore, we show the synergistic effect of the amount of load and the frequency on drug uptake by the cartilage. In the described model, we have shown that, under compressive load, drug delivery from a depot was beneficial over conventional intra-articular drug administration. The assay mimics the complexity of the knee joint in several key aspects, which results in a more close representation of the expected drug outcome. In this study, we have evaluated the penetration of a model small molecule drug into articular cartilage under compressive conditions, and future development will focus on incorporating synovial(-like) fluid, synovium, and bone to increase the predictive potential of the assay further.
Introduction
Osteoarthritis (OA) is a degenerative disease that affects articular cartilage and surrounding tissues in the joint. 1 –4 Evidence is accumulating that aberrant joint loading is one of the causative factors initiating the onset of OA. 5 –9 Unloading of the joint by distraction has been hypothesized as a possibility to trigger a regenerative response by the body. 10 –14 In this procedure, the femur and tibia are pulled from each other thereby decreasing the compressive load on the affected tissue. 7 In animal models, this procedure has shown promising results and is now being evaluated in a clinical setting, where also positive results are obtained. 15 –20 This technique is however invasive.
Therefore, less invasive treatment options are explored as alternative. Common practice entails still oral and intra-articular drug administration, which aims at elevating pain and other clinical symptoms to improve quality of life. 21 –25 Although short-term pain relief is achieved after intra-articular drug administration, patients require recurring injections to stay pain free, as drugs are cleared quickly from the synovial fluid. 26 Therefore, the injected dose is usually high with increased risks of side effects, and the effect of these recurrent high doses is not well known. Currently, attempts are made to boost matrix production by injecting matrix components or growth factors. 27 –29
To avoid high doses, one can inject a depot, so-called drug delivery systems (DDSs), to locally deliver drugs (bulk or micro-encapsulated) over a prolonged period. This can be a suitable treatment as most OA affected joints are amenable for intra-articular injection. 30 –37 The depot ensures longer retention of the drug in the joint, because it is slowly released. Consequently lower dosages can be used. 22,38,39 A tailored release, depending on material properties, is established by diffusion of the molecules from the DDS and the degradation of the material. Characterization of these systems is often done in vitro by assessing their degradation behavior and their release profile. 40 –44 Moreover, these tests are done under static conditions which do not simulate the compressive environment the depot will be subjected to in vivo.
Due to a shortage of data on the behavior of drugs in the knee cavity after injection, there is also little known about to what extent a drug penetrates the cartilage tissue. The depth of penetration and its action under mechanical loading are largely unknown. Therefore, emphasis is put on creating an in vitro assay that can simulate key characteristics of the native joint environment, such as nutrient supply and mechanical stimulation. These systems then can aid in the evaluation of DDSs in a simulated joint environment before in vivo testing. Previously our group has reported on a dual flow bioreactor in which articular cartilage could be supplied with nutrients from both the synovial and the subchondral sides. In addition, it is equipped to apply cyclic mechanical stimulation thus creating an environment that simulates the knee joint in two important aspects. 45
In the present work, this system is applied to investigate the penetration behavior of a small molecule model compound, bromophenol blue (BPB), from a hydrogel into cartilage under compressive and hydrodynamic stimuli. In this assay, the DDS is added to the synovial side of the cartilage explant simulating intra-articular injection and subsequently mechanical stimulation is applied. BPB allowed us to evaluate the penetration into the articular cartilage over time and under different conditions. The blue staining was then used to determine the diffusion coefficient of BPB. This assay can be used to determine the applicability of DDSs in the knee joint further aiding in their development for clinical use.
Materials and Methods
Hydrogel Production
Poly(caprolactone-
For the specific polymer used in these experiments, the following procedure was used.
Under a nitrogen atmosphere, PEG1,500 (20 g), ɛ-caprolactone (35.2 g), and
The stirred mixture was cooled to ca. 100°C, followed by the addition of stannous octoate (0.4 mL). The mixture was stirred overnight at 120°C, after which it could cool to ambient temperature.
Dichloromethane (100 mL) was added, followed by the addition of triethylamine (9 mL). After stirring for 15 min at ambient temperature, excess of acetyl chloride (4 mL) was added dropwise. The obtained mixture was stirred for 4 h at ambient temperature.
The volatiles were evaporated under reduced pressure, followed by the addition of ethyl acetate (300 mL). After stirring for 5 min the mixture was filtered over a P3-glasfilter to remove triethylamine hydrochloride. Hexane was added until a precipitate was formed. The obtained mixture was stored in the freezer for 3 h, and the solvents were then decanted from the polymer. The polymer was dried under vacuum. The yield of the final product was around 80%.
For visualization purposes the gel was loaded with 0.025 wt% BPB (a hydrophobic molecule of 670 Da which is used as a model for small molecule drugs; in comparison triamcinolone acetonide, a drug used in the palliative treatment of OA, has a molecular size of 395 Da). The mechanical and physical properties of this hydrogel were described by Sandker et al. 48
In Vitro Evaluation
Material source
Knees of 10–12-month-old calves were collected from the local abattoir. Femoral condyles were exposed by removing the muscles and patella. Then, cartilage slices were made with a custom-made slicer, and cubical explants were punched from these slices and put into four chamber polycarbonate insert as described previously. 45
Explant culture
Three drops of hydrogel (26.5 μL) loaded with BPB (Fig. 1A) were placed on the surface of the cartilage explants, placed in a custom designed bioreactor published previously (Fig. 1B), 45 and compressed for 1 h with varying load (F) (0.05, 0.25, and 0.5 MPa, at constant frequency [f] of 0.33 Hz, compression time per cycle 50%). In the same manner, distinct frequencies were tested (0.1, 0.33, and 1 Hz, at constant load F = 0.25 MPa, compression time per cycle 50%). To investigate the effect of free swelling conditions and continuous compression on BPB penetration, explants were either subjected to 1, 6, 9, or 24-h of static culture or continuous compression (F = 0.25 MPa and f = 0.33 Hz, 3 × compression cycles).
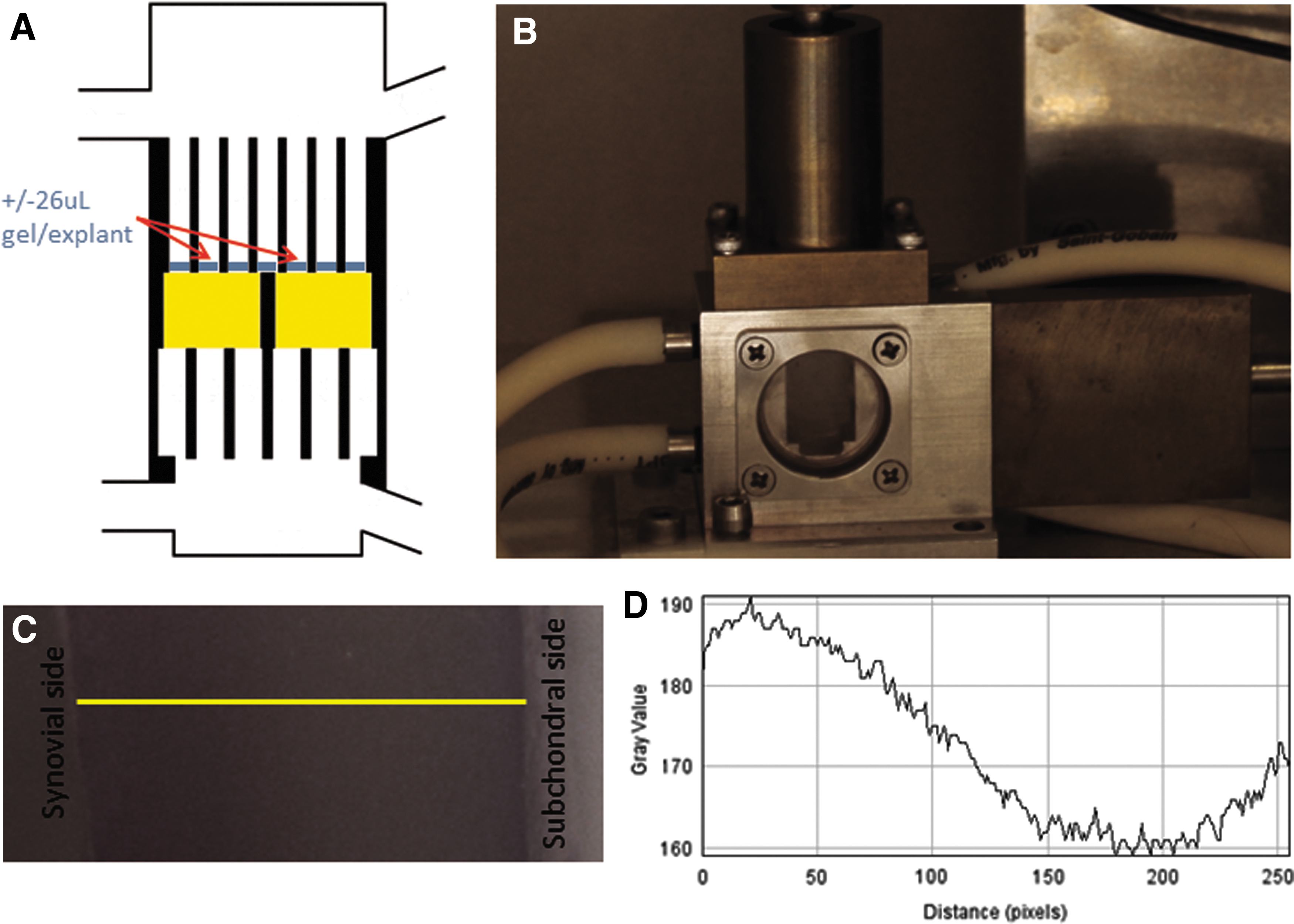
Dual flow bioreactor for the evaluation of drug delivery systems.
The influence of clearance was investigated by either direct injection of dissolved BPB (0.025 wt%) in medium at the top compartment or placing a hydrogel loaded with an equimolar concentration of BPB on top of the explants. Then, the bioreactor was connected to a syringe pump as described previously, 45 and medium flow was applied at 0.5 mL/min. Medium in the syringes was changed every 20 min for 1 h.
Macroscopic evaluation
Directly after compression, explants were dissected, BPB stain in the middle of the explant was evaluated by stereomicroscopy (Nikon, Japan), and pictures were taken with Q-Capture acquisition software (Fig. 1C). After these pictures were gray scaled, a plot profile was made along the middle line (synovial to subchondral side) of the explant with ImageJ software (Fig. 1C [yellow line] and D). Fick's law was used to estimate the diffusion coefficient after static release and release after continuous and discontinuous compression.
Estimation of the diffusion coefficient using Fick's law
When it is assumed that in a region −L < x < L the concentration of the molecule at t = 0 is C
0 and at the surfaces the concentration is kept constant at C
1, the solution of Crank can be considered. This assumes a system of nonsteady state diffusion with uniform initial distribution and equal surface concentration
49
When n is assumed 0, Equation (1) becomes:
To enable calculation of the diffusion coefficient D, Equation (2) can be written as
50,51
:
Assuming that the grayscale plot profile represents a concentration profile, the concentration term in Equation (3) also can be written as a grayscale ratio
50,51
:
When ln(G
1 − G)/(G
1 − G
0) is plotted against time, the slope of this plot gives the diffusion coefficient
50,51
:
where G is the gray value at point x along the middle line, G 0 is the lowest gray value along the middle line, G 1 is the highest gray value along the middle line, 2L is the total length of the explant (m), x is the position in the explant where the diffusion constant is determined (m), D is the diffusion coefficient (m2/s), and t is time (s).
Results
Effect of Clearance on the Penetration of BPB into Articular Cartilage
We studied BPB penetration in articular cartilage after injection of an aqueous solution of BPB or deposition of a gel loaded with an equimolar concentration of BPB in a bioreactor in which synovial clearance, the turnover of synovial fluid, is mimicked. Visual inspection confirmed that BPB penetrated further into the cartilage when released from the gel compared to the dye that was directly injected in the synovial compartment (standard condition) (insets Fig. 2). Quantification of the BPB distribution within the cartilage showed distinct profiles with a sharp peak close to the cartilage surface and fast declining slope in the standard condition, whereas the profile in the gel condition showed a broader peak at the synovial side and a slow declining slope (Fig. 2). This indicated that BPB uptake by cartilage from the gel was higher compared to the injection of an equimolar concentration of dissolved BPB in the medium compartment resembling the synovial fluid.
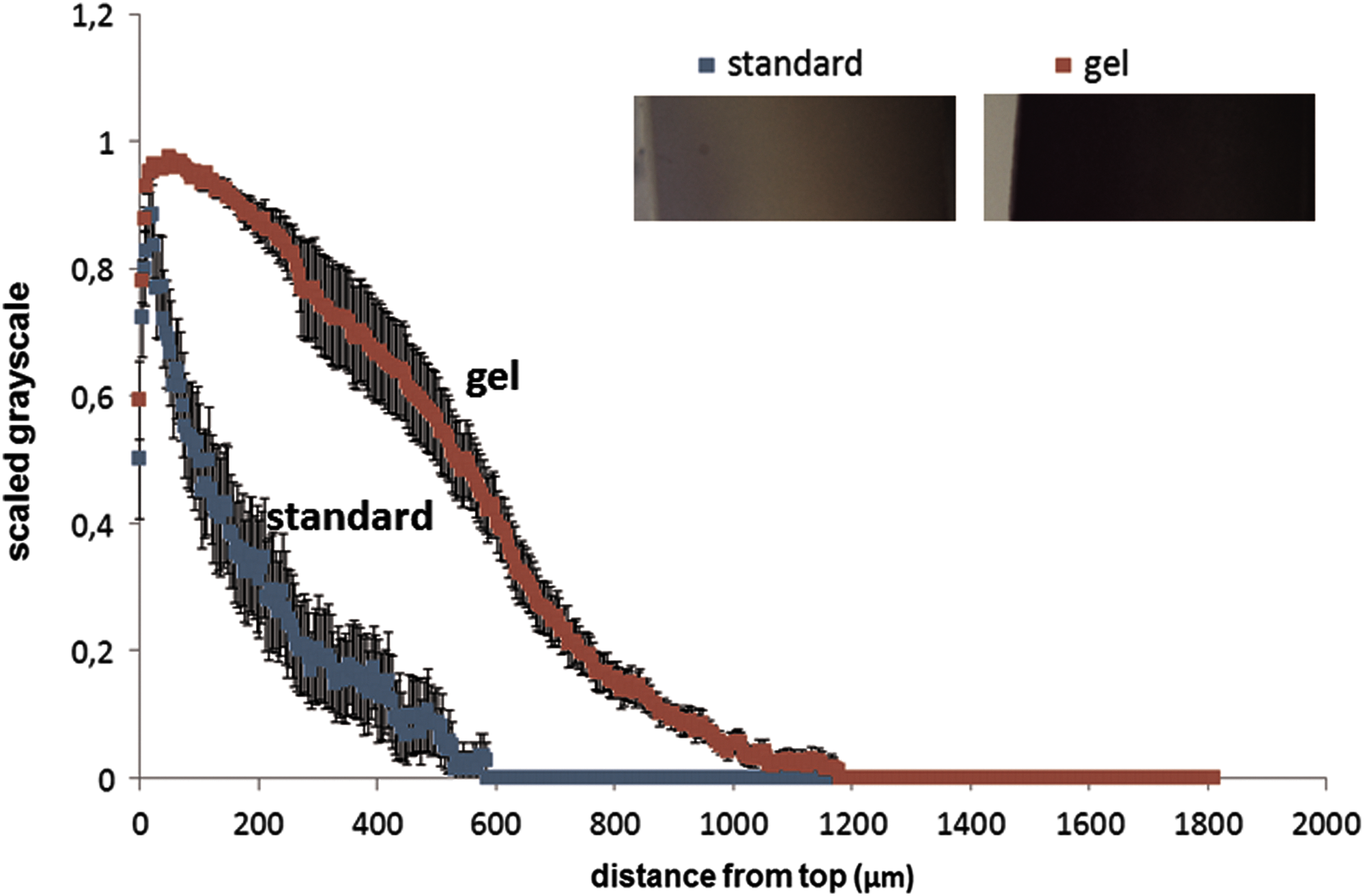
Influence of clearance on static BPB delivery into articular cartilage after 1 h. The graph represents the scaled mean grayscale profiles of BPB concentration into an explant. Insets represent explants of each condition with the synovial side on the left. Error bars represent the standard error of the mean, n = 12 explants. BPB, bromophenol blue. Color images are available online.
In an experiment using the gel setting but omitting clearance, a profile like the one of the gel condition in Figure 2 was observed (data not shown). This indicated that the clearance itself did not have an influence on the release behavior of BPB from the gel and subsequent uptake by the cartilage and was therefore not considered in subsequent experiments.
Effect of Release Duration on BPB Concentration Profile Within Cartilage
Next, we determined how the BPB distribution changes through cartilage over time. The obtained profiles after 1, 6, and 9 h of release without compression showed distinct profiles, including an increasing plateau at the synovial side indicating a further penetration of the highest BPB concentration, as well as a broader BPB distribution as observed by the steepness of the curve (Fig. 3). It seemed that after 9 h the BPB concentration profile did not change significantly compared to the profile after 24 h (Fig. 3). This was probably due to saturation of the tissue. These graphs show how a small molecule drug could be distributed through cartilage tissue when a patient is not allowed to use the joint for up to 24 h after injection of a drug depot in the knee cavity without taking synovial clearance into account.

Characterization of the concentration profile of BPB into articular cartilage after static incubation. The graph represents the scaled mean concentration profiles of BPB in an articular explant. Error bars represent the standard error of the mean, n = 12 explants. Insets represent explants of each condition with the synovial side on the left. Color images are available online.
Effect of Load and Frequency on BPB Penetration
When after 1 h of compression with varying loads the concentration distribution profiles were compared, the main difference observed was that after compression with 0.05 MPa the profile seemed like the one where no compression was applied. Under the other two conditions the profile seemed steeper. However, no significant differences were detected between the distribution profiles (Fig. 4A). When the frequency was varied, a similar observation was made. After 1 h of compression no significant differences were observed between the conditions in the distribution profiles, although under all frequencies the profiles tended to be lower compared to the noncompressed condition (Fig. 4B). So, within the range of load and frequency applied in this study no differences appeared. However, what seemed to be consistent was that the penetration of BPB under compression seemed less pronounced compared to conditions without compression (comparing the blue line with the other lines in Fig. 4A and B ) except for 0.05 MPa condition. To investigate if this effect would also appear when the delivery period was prolonged, we determined the BPB profile under continuous compression over time.
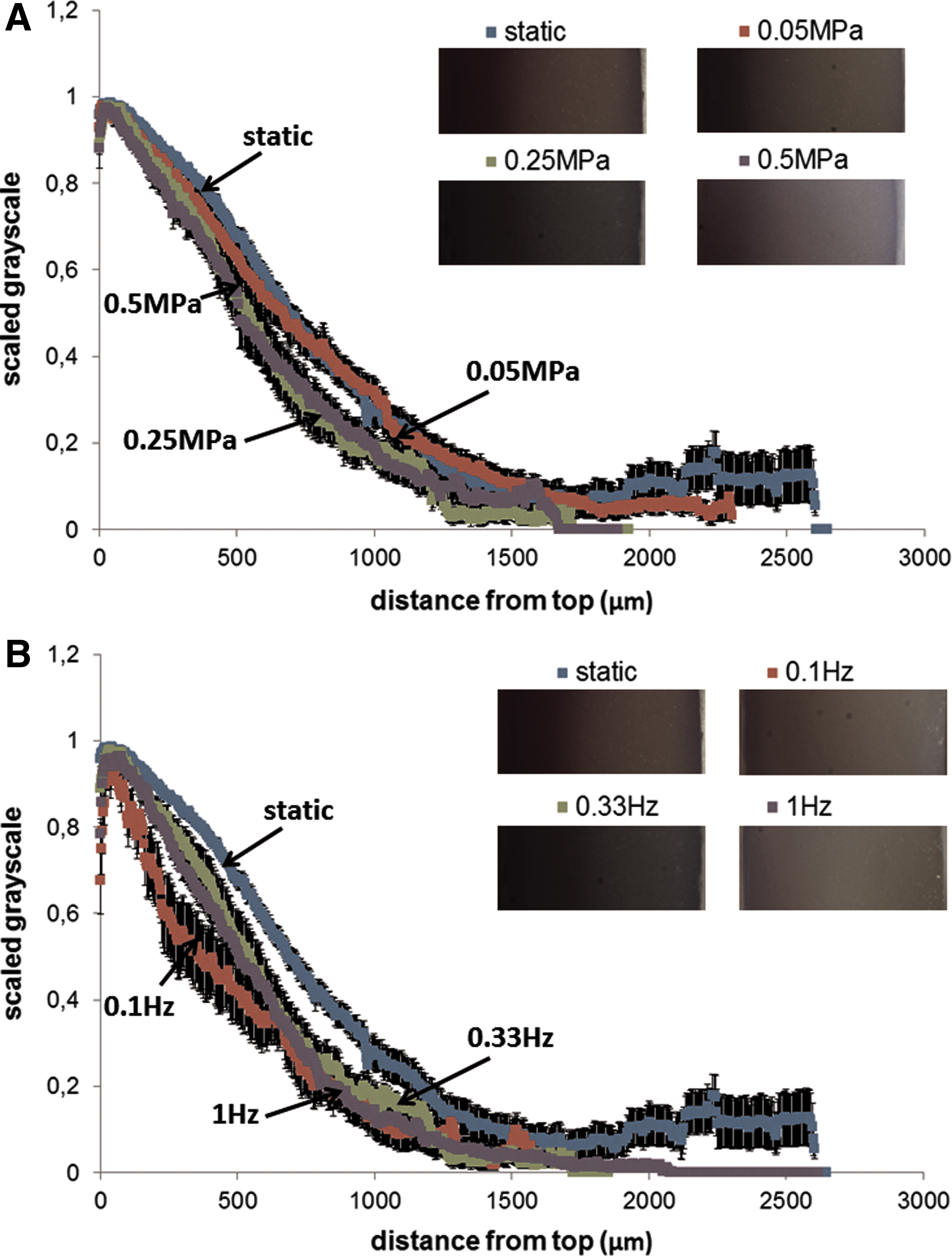
Influence of the amount of load (f = 0.33 Hz) and frequency magnitude (F = 0.25 MPa) on BPB penetration in articular cartilage after 1 h.
Effect of Free Swelling and Continuous Compression on BPB Penetration
When the BPB profiles within the explant were compared following 6, 9, and 24 h of continuous compression, a peak near the articular surface was observed. However, the slope after 9 and 24 h was found to be less steep compared to that at 6 h with the 24-h profile being lower than the 9-h profile (Fig. 5). This finding was comparable to the trend seen after static treatment (Fig. 3). Further comparison of these two figures showed that the high concentration at the synovial side ran further into the tissue when no compression was applied (Fig. 3).

Influence of continuous compression on BPB penetration into articular cartilage, F = 0.25 MPa, f = 0.33 Hz. The graph represents the scaled mean concentration profiles of BPB in an explant. Error bars represent the standard error of the mean, n = 12. Insets represent explants of each condition with the synovial side on the left. Color images are available online.
These data show that BPB penetration into cartilage decreases when the tissue is compressed. We hypothesize that this could be enhanced by allowing the tissue to relax and regain its original form. This would induce transport of water molecules and solutes from the synovial cavity into the cartilage matrix due to mechanical stimulation. However, it should be further investigated how the penetration profile would look like when a cartilage explant is discontinuously compressed (i.e., a compression period followed by a rest period).
Estimation of the Diffusion Coefficients
As Equation (4) shows, ln(G1 − G)/(G1 − G0) is a function of time t. Therefore, it was only possible to estimate the diffusion coefficient (D) at two conditions, BPB penetration after static (D(static)) release in Figure 3 and after continuous compression (D(comp)) in Figure 5. Both values were calculated at x = 1,000 μm. A trend line was fitted through the data points of each condition, and the slope was used to calculate D according to Equation (5), resulting in D(static) = 3.86 × 10–12 m2/s ± 1.47 × 10–12 and D(comp) = 2.04 × 10–12 m2/s ± 1.43 × 10–12.
Table 1 compares the diffusion coefficients of BPB (670 Da) found in this study to diffusion coefficients of molecules into cartilage matrix under compressive conditions. Diffusion of tetramethylrhodamine (TMR, 430 Da) into compressed bovine explants was found to be 25 times higher compared to our findings. 52,53 There could be several reasons for this difference: (1) the diffusion matrix; TMR could diffuse through a 650 μm cartilage sheet consisting mainly of the intermediate zone, whereas in this study full-thickness cartilage explants were used or (2) the mobility of the solute; TMR was administered in an aqueous solution, whereas BPB was encapsulated in a hydrogel. Alexa-hydrazide (570 Da) was found to diffuse ∼100 times faster into a hyaluronic acid network from an aqueous solution under noncompressed conditions. 54 Collagen condenses an intact cartilage matrix resulting in lower diffusivity of solutes. This can explain the difference in diffusion coefficients. In the same study it was found that alexa-albumin (66 kDa) diffused faster into an enzymatically degraded cartilage matrix. 54 This showed that it is the complex structure of the cartilage extracellular matrix that determines the diffusion coefficient of solutes instead of just one.
Comparison of Diffusion Constants in Compressed Articular Cartilage
BPB, bromophenol blue; FITC, fluorescein isothiocyanate.
Cartilage is an anisotropic tissue. Gradients of the two main matrix components, collagen type II and glycosaminoglycans, run through the tissue from synovial to subchondral side and vice versa, respectively. 55 The peak near the articular surface, which was consistent in all experiments, can be explained by BPB accumulation in this region. This means that the diffusion was delayed creating a depot in the superficial zone. This could be related to the local high density of the collagen network. The gradual decline in the profile suggests that with increasing glycosaminoglycan concentration in the zones underneath the superficial layer the retention of BPB in the cartilage matrix is decreased and thus its diffusion increased. This is consistent with the findings of Evans and Quinn. 56
Discussion
To the best of our knowledge this is the first in-depth study on the behavior of a drug depot for intra-articular injection under physiological relevant conditions in vitro. In vitro assays have been reported that aim at discovering biomarkers for drug treatment. 57 –59 Drug depots have the potential to replace current drug administration approaches. They can deliver a drug locally and release that drug for a longer time period as can be realized with conventional intra-articular injection in the treatment of OA as reviewed by several investigators. 60 –62 Such treatment will result in prolonged activity of a drug and thus enhanced efficacy of the treatment.
Most patients start using their joint shortly after the injection of the drug. However, it is yet unclear how mechanical compression affects the drug release and uptake. This raises the question if a physician should advise a patient to not or only minimally load the joint to enhance the penetration and action of the drug in cartilage. Therefore, in this study a drug delivery hydrogel was subjected to compressive loading to simulate the stimulation in the clinical situation, and the resulting drug uptake by cartilage was evaluated.
Clearance of the synovial fluid can decrease the uptake of a drug as reviewed by Simkin. 63 In an environment that simulated clearance it was shown in our study that the uptake of BPB after conventional intra-articular injection was significantly decreased compared to injection of BPB in a gel depot. This was in accordance with findings of Jovanovic et al., where they found that the delivery of silver particles under compression and convection was improved compared to release under static conditions. 64 It suggested that the concentration that can be achieved following direct injection may be lower than the minimal concentration required for the drug to work efficiently. 65 In contrast, dye penetration from a drug depot did not seem to be hampered by clearance compared to the profile without clearance in our study.
One consideration to be made is that in this assay a situation was created where the hydrogel was confined to the articular surface and due to the compression was dispersed into the rest of the chamber. In the in vivo situation, the hydrogel will form a drug depot within the articular joint. 66 The penetration profile of a drug from such a depot might look like the profile of the dissolved BPB presented in this article. The drug will have to diffuse from the depot and will then act as a dissolved substance in the articular fluid and be cleared at a similar rate. The prolonged release of the drug depot might increase the penetration of the drug depending on the clearance rate of the drug. We chose to set up an assay that could predict the penetration behavior of a drug from a hydrogel that interacted with the articular surface as our laboratory is developing hydrogels with these properties. 67
The clearance of a drug is determined by the viscosity of the synovial fluid. The higher the viscosity the lower the clearance and vice versa. With disease progression a reduction in the synovial fluid viscosity is observed. 68 Current treatment in early onset OA can involve viscosupplements like hyaluronic acid. As these increase the viscosity of the synovial fluid, they will increase the retention of the drug in the joint. In this assay we have not used these supplements as a control, but we recommend adding them as a comparison for drug behavior in the joint and penetration into the tissue. With the action of the drug, the tissue will regenerate and will start to release proteins that increase the viscosity of the synovial fluid. Therefore, the viscosity can be used as a benchmark for the action of the drug that is released from the hydrogel.
In this study, the influence of load and frequency after 1 h of delivery of a small molecule was negligible compared to delivery without mechanical stimulation. To optimize the drug uptake in cartilage a patient should avoid mechanical loading of the joint directly after injection of the depot. Once uptake of a drug in cartilage has been achieved, the cartilage itself may function as a drug depot. Several studies have elucidated bioreactor culture conditions for load and frequency that induce chondrogenic differentiation and/or cartilage matrix production. 69 –72 These data can help in optimizing the assay parameters to mimic pathophysiological conditions better. Of note, the experiments reported in this study were performed with healthy young cartilage. Drug penetration is determined by the composition of the tissue.
Cartilage is an anisotropic tissue with varying matrix composition between superficial, middle, and deep zones. 55 The estimation of the BPB diffusion coefficient and the peak near the articular surface in the BPB profiles under free swelling and continuous compression suggest that due to the complexity of the cartilage tissue its diffusion constant may not be considered homogeneous. Drug penetration is determined by several parameters such as water in- and outflow, interaction with the matrix, and free diffusion. Thus, the water content, as well as quantity and arrangement of matrix molecules, determines the transportation and distribution of a molecule within the tissue. During disease progression, the cartilage matrix degenerates, and this will influence the drug uptake by cartilage. The choice of the drug for treatment should also be dependent on the degree of matrix degradation to optimize treatment outcome.
Currently, techniques are developed to predict the stage of the disease, which can then be used to personalize the treatment options. 73 Another way to increase the penetration and retention of a drug in an affected joint could be achieved by enhancing the drug specificity with a moiety targeting one of the matrix components of cartilage or a drug loaded biomaterial that could attach to the degraded cartilage matrix.
Optimizing drug delivery into affected tissue is a current challenge in translational research as this will enhance our understanding and help elucidate the most optimal strategy to treat patients suffering from a degenerating disease like OA. 64
Conclusion
Our study showed that hydrogel drug depots can be the next step in effectively delivering drugs into cartilage tissue with favorable effects over conventional intra-articular injection. In addition, we showed that compression of cartilage will enhance drug delivery into the tissue. Further investigation will aid in developing a more patient-tailored treatment as a better understanding will allow us to determine how a drug specifically and efficiently can be delivered to each patient's tissue.
Footnotes
Acknowledgments
This research forms part of the Project P2.02 OA control of the research program of the BioMedical Materials Institute, co-funded by the Dutch Ministry of Economic Affairs.
Author Contribution
Study design: T.W.G.M.S. and M.K. Experimentation and data interpretation: T.W.G.M.S., D.S., and M.K. Hydrogel preparation: A.P. and M.G.W.d.L. T.W.G.M.S. wrote the article with the help of all authors. M.K. supervised the study.
Disclosure Statement
M.G.W.d.L. is a founding member of Ingell Labs. For all other authors, no competing financial interests exist.