
Abstract
Micro- (MPs) and nanoparticles (NPs) have been recently studied for their application in ophthalmic drug delivery. These drug delivery systems are able to circumvent the ocular barriers that currently limit the efficacy of conventional treatments, as well as provide a more sustained release of drug, reducing the frequency of administration and increasing patient compliance. This review summarizes the recent trends in ophthalmic research from conventional treatment to the utilization of MPs and NPs as drug carriers.
Introduction
The eye is an essential sensory organ of the human body. It is responsible for sight, visual cues, and maintaining balance.
1
Ocular diseases are pathologies that affect the eye. They can be classified as anterior segment or posterior segment diseases based on the anatomic regions of the eye that they affect. The anterior segment of the eye can be readily accessed for therapeutic intervention through eye drops or topical administration.
2
However, the posterior segment, including the choroid, vitreous, and retina, possesses several barriers, as well as clearance mechanisms, which limit access to therapeutic intervention. Therefore, it is imperative that researchers find a method of drug delivery that consists of the following characteristics
2,3
: Efficient barrier(s) penetration, Patient-friendly administration, Minimal side effects, Reduced toxicity, Sustained drug release, and Localization of the drug in the desired area.
Nanoparticles Versus Microparticles
One way to obtain this ideal drug delivery system is through the entrapment of drugs within polymeric nanoparticles (NPs) (1–1,000 nm) or microparticles (MPs) (1–1,000 μm). 4 –6 Micro-/nano-based systems possess the unique ability to be designed to meet specific needs based on their intended application because their structures are made up of atoms/molecules with various sizes and morphologies. These structures may be applied to the field of pharmaceutics by encapsulating active pharmaceutical agents to improve efficacy, sustainability, distribution, biocompatibility, and toxicity. 7 The major benefits of applying micro-/nanotechnology specifically to ocular drug delivery may be summarized as follows:
Smaller particles are compatible with the eye,
Size of particle allows for more patient-friendly administration,
Particles around 200 nm administered through intravitreal injection are able to be localized in the retinal pigment epithelium (RPE), 8
NPs have increased solubility and surface area,
NPs are able to be manipulated by altering the weight and hydrophilicity, resulting in a more sustained release. 9
Formulation and Characterization Methods
The two primary MP/NP formulation methods are “top-down” and “bottom-up.” The “bottom-up” approach involves manipulating thermodynamic properties to build nanostructures from smaller molecules and atoms. For example, one may alter precipitation, crystallization, emulsification, self-assembly, etc. to construct the appropriate structure. 7 The “top-down” approach involves the utilization of photolithography, micro-/nanomolding, micro-/nanofluidics, etc. to reduce the size of large molecules to form nanostructures. 10 This approach has been found to be more cost effective in manufacturing. Materials used include chitosan, lipids, poly(D,L-lactide-co-glycolide) (PLGA), poly(lactide-co-caprolactone) (PCL), poly(vinyl alcohol) (PVA), poly(DL-lactide), poly(ethylene oxide-b-lactide), etc. 4
Methods of characterization include encapsulation efficiency, drug loading capacity, size, uniformity, zeta potential, etc. Encapsulation efficiency, or entrapment efficiency, describes the amount of drug entrapped by the MPs or NPs compared to the amount of drug used in preparation. Drug loading capacity describes what percent of the particle's mass is contributed by drug.
11
It has been reported that the drug loading capacity value will always be lower than the encapsulation efficiency, as it divides the amount of drug present by the total mass of a particle (the amount of drug in addition to the amount of polymer).
12,13
The amount of drug present can be determined through examination by ultraviolet/visible spectroscopy or chromatography (high-performance liquid chromatography [HPLC], liquid chromatography—mass spectrometry [LC/MS]) with utilization of the equations below.
The ideal size for MPs/NPs depends on the therapeutic application. Both size and zeta potential (surface charge) are commonly determined using dynamic light scattering and imaging methods. 14 These characteristics prominently influence the cellular uptake of particles. In addition, the shape and dimensions of a MP/NP can greatly influence how it is internalized by cells. Imaging is a valuable tool for analyzing these properties. Multiple technologies have been developed to allow for the visualization of these particles such as transmission electron microscopy, scanning electron microscopy, scanning tunneling microscopy, and atomic force microscopy (Table 1) followed by in vitro and in vivo studies. 15 –17
Characteristics of Micro-/Nanoparticle Imaging Techniques
3D, three-dimensional; AFM, atomic force microscopy; SEM, scanning electron microscopy; STM, scanning tunneling microscopy; TEM, transmission electron microscopy.
Ocular Anatomy
The eye is responsible for providing what is arguably the most critical of senses: sight. It is essential for maintaining balance and providing a sense of one's surroundings. A cross-section of the eye shows both the anterior (cornea, iris, pupil, ciliary body, and conjunctiva) and posterior (sclera, choroid, retina, fovea, optic nerve, and vitreous body) segment structures (Fig. 1). Barriers to these structures include the mucoadhesive tear film on the surface of the eye, tight junctions within the cornea, inner limiting membrane, blood–aqueous barrier (BAB), as well as the blood–retinal barrier (BRB), which is composed of Bruch's membrane (BM), and the RPE (Fig. 2).
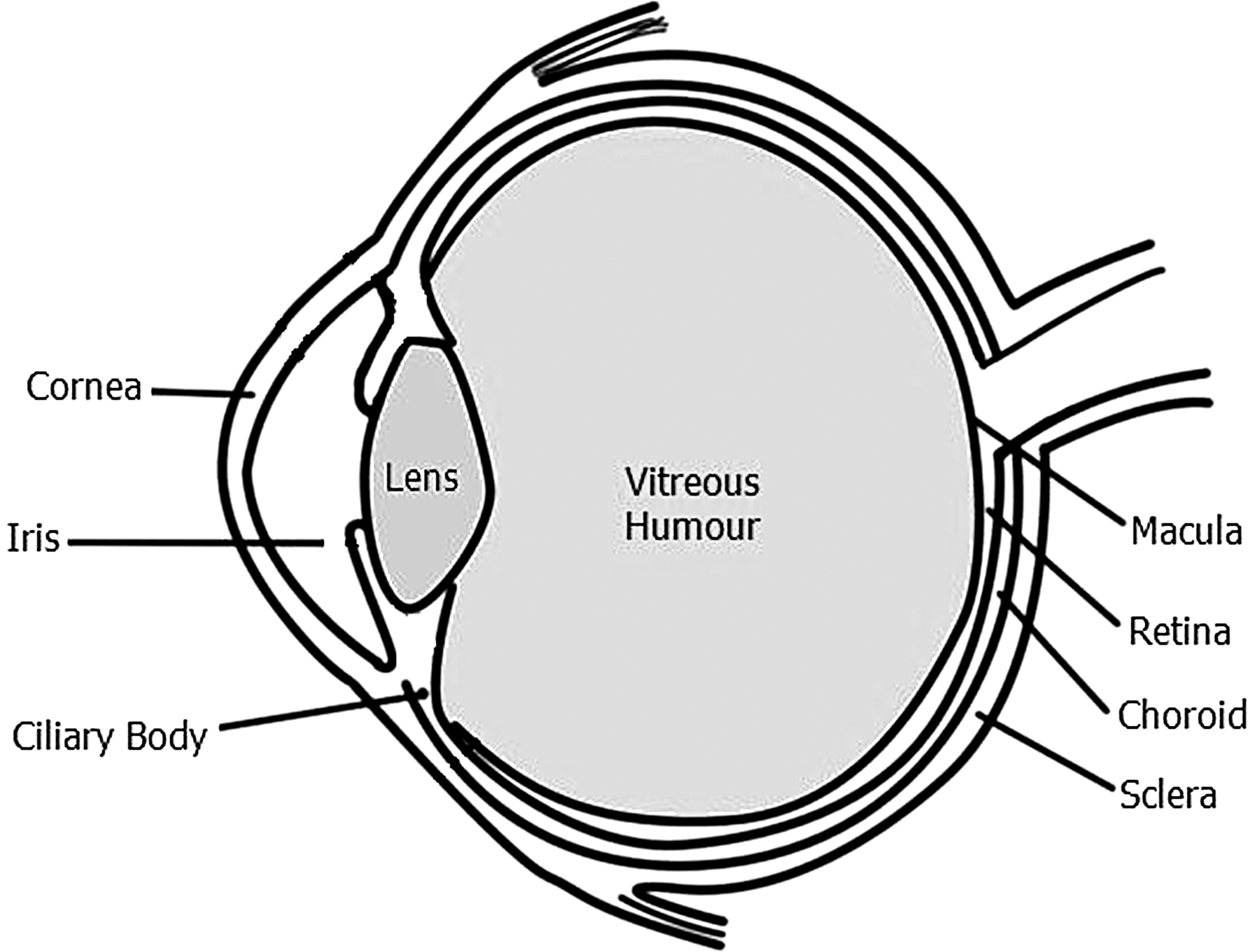
Labeled image of prominent sites within the eye.

Labeled image of barriers within the eye:
Routes and Targets for Drug Intervention
Multiple modes of administration are available for ocular therapies. These include topical, systemic, subconjunctival, and intravitreal administration (Table 2). Topical administration is the most common route of administration for anterior segment ocular diseases (Fig. 3A). 18 However, this route has a <5% bioavailability due to several barriers (i.e., corneal epithelium, corneal endothelium, retinal endothelium, and RPE) and nasolacrimal drainage. 19 The posterior segment of the eye is more difficult to reach. Therefore, the preferred administration routes are intravitreal or subconjunctival injection (Fig. 3B, C).

Labeled image of administration routes:
Administration Routes for Anterior and Posterior Segment Ocular Diseases and Their Characteristics
There are several angiogenic factors that have been known to contribute to the progression of posterior segment ocular diseases. Therefore, ocular neovascularization can be combated with a variety of antiangiogenic therapies targeting these different factors. 9,20 Vascular endothelial growth factor (VEGF) plays a central role in mediating angiogenesis and vascular permeability. The presence of elevated levels of VEGF has been observed in neovascular membranes in some diseases (age-related macular degeneration [AMD] and diabetic retinopathy [DR]), and its intraocular levels show strong correlation with the neovascularization associated with these pathologies. 20 In addition, it has been reported that hypoxia inducible-factor 1α (HIF-1α) results in the overexpression of VEGF, as well as other proangiogenic factors, including platelet-derived growth factor 21 and angiopoietin-like 4, 22,23 which are prominent components of many ocular diseases. Therefore, the suppression of HIF-1α may prove another beneficial therapeutic target for posterior segment ocular diseases such as AMD and DR. 23,24 For example, Yoshida et al. utilized digoxin to treat mice with ischemic retinopathy. The results demonstrated successful inhibition of HIF-1α translation. 24
Ocular Diseases
Dry Eye
Dry eye, or keratoconjunctivitis sicca (KCS), is an ocular disease associated with the inflammation of the ocular surface and lacrimal glands. KCS may be caused by tear deficiency or excessive tear evaporation due to a damaged interpalpebral ocular surface or a number of systemic diseases (i.e., diabetes mellitus, thyroid disease, rheumatoid arthritis, and systemic lupus erythematosus). 25 Patients suffering from dry eye are at risk for bacterial infections (i.e., keratitis), which can lead to blindness. Conventional treatments are dependent on the severity of the condition. For example, mild-to-moderate dry eye may be treated with gels and ointments to replenish tears, and more severe conditions may be treated using aggressive therapies, including corticosteroids, antibiotics, or surgical intervention. 25
Micro/nano-application
Researchers investigated the use of chitosan-based NPs loaded with cyclosporine A (CyA), a local immunosuppressant, for topical administration in the treatment of extraocular disorders like dry eye. 26 These NPs were formulated using ionic gelation and characterized for their size, encapsulation efficiency, and zeta potential (Table 3). The results of the in vitro study determined a gradual sustained release over 24 h. In vivo studies were performed on rabbit models and demonstrated a sufficient therapeutic concentration in the cornea within 48 h. Inner ocular structures, as well as blood and plasma, were tested, and no CyA was found, confirming that the drug remained at the target site. These data were compared with a solution of free CyA, which demonstrated significantly higher concentrations in the inner ocular structures, including the iris and vitreous humor, and no sustained release properties. 27
Researched and Marketed Micro-/Nanoparticle Drug Delivery Systems for the Treatment of Various Ocular Diseases
AMD, age-related macular degeneration; CNV, choroidal neovascularization; CyA, cyclosporine A; EE, entrapment efficiency; IOP, intra ocular pressure; MPs, microparticles; NPs, nanoparticles; PCL, poly(lactide-co-caprolactone); PEG, polyethylene glycol; PEO, polyethylene glycol; PLA, poly lactic acid; PLGA, poly(D,L-lactide-co-glycolide); PVA, poly(vinyl alcohol); siRNA, small interfering RNA; VEGF, vascular endothelial growth factor; ZP, zeta potential.
Glaucoma
Glaucoma is reportedly the leading cause of irreversible blindness in the world, affecting >70 million people worldwide. 28 This disease is caused by a group of optic neuropathies that lead to progressive degeneration of retinal ganglion cells. Damage to these neurons results in what is called “cupping” of the optic disk and vision loss. From a pathophysiology standpoint, glaucoma patients are observed to have elevated intraocular pressures. Therefore, reducing intraocular pressure is considered the only proven method to treat glaucoma. Several clinical trials show positive results in slowing disease progression and preventing the development of the disease. 28
Micro/nano-application
Researchers at the University of Pittsburgh have studied the utilization of PLGA microspheres (20 μm) containing brimonidine tartrate, a conventional drug used in the treatment of glaucoma. These microspheres were then entrapped within a hydrogel, and rabbit models were used to determine the reduction of intraocular pressure through topical administration (i.e., eye drops). The results of the study showed sustained, long-term drug delivery by the observance of reduced intraocular pressure up to 28 days postadministration with no signs of irritation or inflammation. 29
In addition, Natarajan et al. developed Lipolat™, a liposomal formulation of latanoprost, which is currently licensed to Peregrine Ophthalmic and is undergoing Phase II Clinical Trials to treat glaucoma (Table 3). When administered through subconjunctival injection, the formulation resulted in a consistent decrease of intraocular pressure for >50 days in rabbits, ≤120 days in nonhuman primates, and >3 months in a First-in-Man clinical trial. 30
Fuchs' Dystrophy
Fuchs' endothelial dystrophy is a bilateral, progressive ocular disease characterized by chronic loss of physiologically and morphologically altered endothelial cells, corneal scarring, vascularization, and potential corneal blindness. Conventional treatments include corneal transplantation and/or surgical intervention at an early stage to ensure that the disease is treated before symptoms become irreversible. 31 Unfortunately, these treatments pose a risk of postoperative complications, including inflammation and infection (refer to below sections).
Cataract
Cataract is a leading cause of blindness globally, with the World Health Organization (WHO) reporting the worldwide numbers of diagnosed patients to be around 20 million, and remains the leading cause of age-related vision loss in the United States. 32 Lens transparency and refractive properties are modulated by the concentration of crystalline proteins in lens fibers. Mutations in these proteins can lead to aggregation, causing cataract formation and elevated oxidative stress. 33 Conventional treatments include vitamins with antioxidant properties (A, C, E, niacin, thiamin, riboflavin, and carotenoids), as well as surgical intervention. 32,34 However, there are many postoperative complications (i.e., inflammation and infection) that may arise from this treatment route.
Inflammation
The inflammatory response is pivotal to injury recovery. However, this process may also further tissue damage, promote angiogenesis, and result in corneal opacity in ocular injuries. Ophthalmic surgeries pose the significant side effect of postoperative inflammation. Conventional prevention and treatment for this phenomenon include steroids. Patient noncompliance resulting in missing a dose of steroid drops inhibits the prevention and treatment of postoperative inflammation (i.e., uveitis). 35
Micro/nano-application
Films made from PCL and PLGA have been administered through subconjunctival implantation in postoperative glaucoma patients for inflammation reduction. 2 For example, Surodex™ (Allergan, Inc., Irvine, CA) is a currently marketed product utilized postcataract surgery to deliver a sustained release of the anti-inflammatory dexamethasone through anterior chamber implantation (Table 3). In addition, Yuan et al. fabricated nanowafers with PVA, a biocompatible polymer that is currently utilized in solution as artificial tears, to combat opacification and loss of vision resulting from neovascularization of the cornea. Once formulated, the nanowafers were loaded with doxycycline, a green fluorescent-emitting antibiotic and implanted onto the corneas of rats to be compared with free drug solution. 36 The results of the study showed that the nanowafer was able to release doxycycline for a longer period of time than free drug with increased precorneal residence time (Table 3).
Infection
Although highly common, the signs and symptoms of ophthalmic infections vary widely in severity and are categorized by those affecting the cornea and conjunctiva, intraocular infections, and infections of the surrounding soft tissue. 37 Infections of the cornea and conjunctiva, including conjunctivitis and keratitis, are the least severe of these groups. Of these, viral conjunctivitis, bacterial conjunctivitis, and allergic conjunctivitis are the most common causes. However, most cases alleviate without medical intervention. 38 Bacterial conjunctivitis may present with mattering and adherence of the eyelids upon waking without itching and may be treated with topical antibiotics to decrease the duration of infection. 38 Typical antibiotics include moxifloxacin (Vigamox®) 39 and azithromycin (AzaSite®). 40 One consistent sign of allergic conjunctivitis is itching. This may be treated with topical antihistamines, mast cell stabilizers, or nonsteroidal anti-inflammatory drugs 38 such as ketorolac tromethamine (Acuvail®), olopatadine HCl (Pataday®), or bepotastine (Bepreve®). 40 Endophthalmitis is a severe intraocular infection often caused by ocular penetration or surgery and must be treated quickly to avoid loss of vision. 38 Antibiotics are prescribed through both intravitreal injection and systemic administration and are repeated as necessary. In acute cases, the vitreous may need to be removed. 41 Soft tissues surrounding the eye may contract infections, including preseptal and orbital cellulitis. Preseptal, or periorbital, cellulitis affects the structures anterior to the orbital septum, including the eyelids. Conversely, orbital cellulitis is a condition affecting structures posterior to the orbital septum. If the orbit and optic nerve are unaffected, preseptal cellulitis may be treated with oral antibiotics. 37 Orbital cellulitis, although less common, can be much more severe than preseptal cellulitis and may be treated with antibiotics or surgery. 42
Micro/nano-application
Genta et al. formulated chitosan NPs encapsulating acyclovir to combat the low bioavailability of conventional acyclovir ointments. The microspheres were ≤25 μm, demonstrated a sustained release profile in vitro, and provided a higher concentration of acyclovir than free drug in the desired area in vivo. 43 Years later, Cortesi et al. characterized Eudragit MPs of acyclovir and found that the release was sustained without any loss of efficacy compared to free drug. 44 Overall, MPs provide significant advantages in the treatment of ocular infections.
Nanocarriers resolve the issue of administration-induced infections by providing a longer residence time at the ocular surface and thereby avoiding nasolacrimal clearance 16 and enhancing bioavailability. 45 Pignatello et al. applied this principle by encapsulating sodium ibuprofen in Eudragit RS100 NPs. Dissolution tests indicated that these NPs demonstrated a sustained release profile and efficacy equal to that of currently administered eye drops with a lower required dose of drug. 46 Costa et al. then investigated the use of chitosan-coated alginate NPs encapsulating daptomycin for the treatment of bacterial endophthalmitis. The size of the NPs ranged from 380 to 420 nm, and the system demonstrated a higher degree of epithelial retention compared to free drug, thus confirming its advantages in ocular therapeutics. 47
Choroidal Neovascularization
Neovascularization facilitates the repair of damaged tissues by promoting the formation of new vessels from preexisting vessels. 9 These newly formed vessels replace any vessels damaged during injury. 48 However, neovascularization in the choroid exacerbates the underlying complication. Newly formed retinal cells grow within the retina, causing intraretinal microvascular abnormalities. Once the growth of new vessels reaches a certain point, they will begin to grow past the surface of the retina into the vitreous and become deficient in tight junctions, thus allowing plasma to leak into surrounding tissue, causing continued degeneration of the vitreous and potentially leading to progression of ocular disease and/or hemorrhage. In addition, further retinal detachment may affect the macula, causing vision loss or blindness. 48 A key feature of choroidal neovascularization (CNV) is hypoxia, which results in elevated HIF-1 levels and stimulates the expression of VEGF. Therefore, CNV is characteristic of several ocular diseases, including AMD, pathologic myopia, DR, and retinal vein occlusion (RVO).
Age-Related Macular Degeneration
AMD is a progressive disorder of the eye in which the photoreceptors and underlying RPE undergo degeneration, which worsens with time. Contemporary statistics suggest that nearly 2 million people in the United States suffer from AMD, but these numbers are likely to reach 3 million by 2020. 49 The disease is generally divided into two categories: wet and dry. Wet AMD accounts only for 15% of all AMD cases. Although its occurrence is relatively rare compared to dry AMD, wet AMD is extremely destructive and can lead to a significant loss of vision. 50 The macula is the most sensitive portion of the eye and is responsible for the sharpness and resolution of central vision. In a healthy eye, the RPE cells in the macular region are displaced in such a way that does not allow retinal blood vessels into the region. Thus, there is no interference with the incoming image on the macular center. In wet AMD, however, new vessels start growing beneath the retina after protruding through the BM. Vessels grow in the avascular regions of the outer retina and into the subretinal space, resulting in initial CNV that can cause blurring and distortion of central vision. This is often one of the earliest symptoms of wet AMD. 51
Micro/nano-application
Kompella et al. utilized solvent evaporation to formulate poly lactic acid (PLA) MPs of polymeric-budesonide, which inhibits the expression of VEGF. This drug delivery system was administered through subconjunctival injection into the eyes of Sprague-Dawley rats and was analyzed 1, 7, and 14 days post-treatment. On the 1st day after treatment the tissue levels of budesonide solution were 2–5.5 times higher compared to MP-encapsulated budesonide. The results of the study found that a 0.1 μM treatment of budesonide decreased the expression of VEGF down to 67% compared to controls while having a 99% rate of cell viability during treatment. 4 Therefore, subconjunctival administration of budesonide-encapsulated PLA MPs is advantageous in providing a sustained drug release within the retina.
In addition, Hirani et al. 9 utilized PLGA NPs conjugated with polyethylene glycol (PEG) (PEG-PLGA) to encapsulate the corticosteroids triamcinolone acetonide (TA) and loteprednol etabonate (LE) through nanoprecipitation. PLGA is Food and Drug Administration approved, and NP forms of the polymer have demonstrated the ability to sustain and control drug release with reduced cytotoxicity and side effects. PEG was utilized for its ability to work in conjunction with PLGA to increase drug release and reduce reticuloendothelial system uptake by maintaining a slow clearance from the bloodstream. TA and LE are conventionally used as solutions for the treatment of ocular diseases such as AMD. 9,52 The results of the study showed that free TA solution significantly reduced the secretion of VEGF after 12 h, but was completely released into the surrounding media within 48 h in vitro. TA NPs provided a sustained release after 72 h and demonstrated a significant reduction in VEGF. This delivery system exhibited a sustained release of TA for ∼10 days. 9
Pathologic Myopia
Pathologic myopia is the seventh leading cause of blindness in the United States and currently shows a particularly high incidence in young generations and urban populations. 53 However, the development of pathological myopia is expected in increase in the United States as the occurrence of myopia has become more prevalent in the aging population. 54 The disease is characterized by a progressive elongation of the eyeball resulting in degeneration of the retina and choroid. Although its exact pathogenesis remains unclear, several risk factors (i.e., peripapillary and subfoveal choroidal thinning, scleral thinning, and deformed/irregular eye shapes) have been identified. 55
Micro/nano-application
The intravitreal injection of anti-VEGF agents has had limited success due to the necessary frequency of injection and associated complications. MPs and NPs provide a sustained release of drug, thereby reducing the frequency of injection and raising patient compliance. Ye et al. prepared bevacizumab-loaded PLGA microspheres for the treatment of CNV caused by pathologic myopia. The results demonstrated that the microspheres delivered a higher concentration of drug to the vitreous than free drug solution and possessed a higher bioavailability (Table 3). 56
Dexamethasone acetate is a potent corticosteroid and anti-inflammatory agent that is used in the treatment of CNV. Xu et al. studied the therapeutic effects of PLGA NPs encapsulating dexamethasone. The NPs demonstrated a controlled and sustained release of drug for 40 days. When administered in rats through intravitreal injection, dexamethasone concentrations remained within the effective range for over 56 days with no retinal toxicity (Table 3). 57
Diabetic Retinopathy
DR is currently the leading cause of legal blindness in the United States, with 4.2 million diagnosed cases and 655,000 of these resulting in sight-threatening symptoms. This disease can be attributed to a major proportion of all visual impairment and irreversible blindness cases worldwide. 51,58,59 DR is a vascular disorder of the retina, which occurs as a complication of diabetes mellitus. Vision loss associated with DR may be caused by various mechanisms, such as neovascularization leading to vitreous hemorrhage or retinal detachment or macular edema and retinal capillary nonperfusion. DR shares a common pathology with AMD as they are both characterized by angiogenesis, inflammation, permeability, and neurodegeneration. Signs symptomatic of retinal ischemia are also evident, including microaneurysms, venous caliber abnormalities, neovascularization, and hemorrhages. 60
Micro/nano-application
Conventional treatments for DR utilize the inhibition of VEGF due to its role in neovascularization and proliferation. VEGF may be produced through several pathways, including the cyclooxygenase 2 (Cox-2) mechanism. 61 Amrite et al. studied the effects of PLGA microspheres loaded with celecoxib, a Cox-2 inhibitor. The MPs demonstrated a sustained release of drug in vitro, and drug was maintained in the retina for 60 days. The MPs reduced VEGF secretion in cells and rats without any signs of toxicity or adverse effects. 61 A recent clinical trial led by Tanito et al. investigated the use of topical eye drops containing dexamethasone-cyclodextrin MPs to treat diabetic macular edema. The 19-participant pilot study found that the eye drops decreased macular thickness and increased visual acuity without adverse effects. 62
Another mechanism responsible for the regulation of VEGF is the Pl3/Akt pathway. Kalishwaralal et al. studied the inhibitory effects of silver NPs in bovine retinal endothelial cells. They found that, after 24 h, the proliferation and migration of the cells had greatly decreased, indicating an inhibition of VEGF through the Pl3/Akt pathway. 63 As stated above, bevacizumab is an anti-VEGF agent commonly used in ocular therapeutics. Lu et al. investigated the efficacy of chitosan NPs containing bevacizumab in diabetic rats. The NPs demonstrated a sustained duration in the retina with no adverse effects. 64
Retinal Vein Occlusion
RVO is widely regarded a common cause of vision loss among the elderly and has been cited as the second most common retinal vascular disease after DR. 65 It is equally prevalent in men and women ∼65 years of age or older 66 and may be classified into two categories based on the site of occlusion: branch retinal vein occlusion (BRVO) and central retinal vein occlusion (CRVO). 65 There is an anatomic variant of CRVO which, according to some studies, is regarded as a third category of RVO: hemi-RVO. 67 In BRVO, occlusion occurs at an arteriovenous intersection, while CRVO usually occurs at the lamina cribrosa of the optic nerve or surrounding tissues. 65 CRVO is observed to be associated with hypertension, diabetes mellitus, and other systemic vascular diseases. Fundus fluorescein angiography shows that CRVO can be further segregated into two types based on ischemic and nonischemic manifestations. Nonischemic CRVO is a result of the occlusion of retinal venous flow, while ischemic CRVO occurs after occlusion of both arterial and venous flow. Ischemic CRVO shows elevated symptoms of intraretinal hemorrhages, capillary nonperfusion, and macular and disc edema. 67
Micro/nano-application
RVO, among other ocular diseases, is caused by the degeneration of retinal neural cells. Erythropoietin has demonstrated neuroprotective properties in the central nervous system and retina. 68 For this reason, Rong et al. formulated and characterized PLGA/PLA microspheres encapsulating erythropoietin-dextran. These MPs demonstrated a sustained release of drug over 60 days and reduced retinal ganglion cell death in a rat model. A single intravitreal injection was shown to be effective for at least 2 weeks. 68
In addition to its potential value in treating AMD, TA has been reported as an effective therapeutic agent for the treatment of RVO and has therefore been studied in various NP and MP preparations. 69,70 Suen and Chau encapsulated TA into NPs using folate-functionalized PEG-b-PCL through nanoprecipitation. The NPs exhibited a sustained release for 4 weeks, low cytotoxicity, and high efficiency in the inhibition of VEGF. 71
Penetration and Biodistribution
Particle size, zeta potential, and administration route are all determining factors for the penetration and biodistribution of MPs and NPs in the eye. Sakurai et al. found that an intravitreal injection of 2 μm polystyrene MPs remained in the vitreous near the injection site and were discharged within 6 days. 72 NPs with a size of 200 nm were evenly distributed in the vitreous, while 50 nm NPs crossed retinal barriers and were found in the retina 2 months postinjection. 72 Similarly, 200 nm carboxylate-modified polystyrene NPs remained at the injection site, whereas 20 nm particles were cleared rapidly through blood or lymphatic circulation. 73 In addition, TA-loaded PLA MPs (2 μm) delivered a sustained release of drug over 2 months, while TA-loaded PLA NPs (551 nm) were unsuccessful in delivering drug. 74 Size is clearly a determinant in drug release rates and biodistribution of particles.
Particles with a zeta potential of ±25 mV are considered highly stable. 59 Anionic particles were reported to diffuse through the vitreous and penetrate the various layers of the retina, while cationic NPs are often attracted by the anionic components of the vitreous and may remain localized before reaching their therapeutic target. 45 To prove this, Kim et al. compared the efficacy of positively-charged and negatively-charged NPs in localizing to the retina and found that negatively-charged particles composed of hyaluronic acid and human serum albumin penetrated the retina and reached the RPE. 75 In addition, previous research has demonstrated that negatively-charged particles are not only more successful than positively-charged particles in penetrating the vitreous cavity but also demonstrate more significant antiangiogenic effects in ocular diseases associated with neovascularization. 76
In addition to size and zeta potential, the administration route used in NP and MP delivery also plays a significant role in biodistribution. Penetration to the posterior segment of the eye requires invasive administration (i.e., systemic, subconjunctival, or intravitreal) and is quite difficult, as the drug must flow in the opposite direction of intraocular liquid circulation and bypass several barriers. 77 Topical administration, which is perhaps the most common route of administration for anterior segment ocular diseases, has a <5% bioavailability due to these barriers, as well as nasolacrimal drainage (Fig. 3A). 18,19 Intravitreal injections insert drug directly into the vitreous of the eye, where the administered drug further diffuses into posterior segment structures like the retina (Fig. 3B). Subconjunctival injections allow drugs to diffuse from the sclera and conjunctiva into the retina and choroid, thereby circumventing most epithelial barriers (Fig. 3C). 19 Biodistribution studies demonstrate that systemic injections are the most efficient in reaching the posterior segment of the eye, but require a potentially toxic drug dose to reach an appropriate therapeutic concentration. 19
Uptake Mechanisms
The uptake mechanism followed by MPs/NPs after ocular administration is dependent on both cell type and particle size. 78 Regardless of administration route the particles must enter epithelial cells, primarily through endocytosis, to deliver drug to the targeted site within the eye (Fig. 4). 79 Endocytosis may be classified as phagocytosis or pinocytosis. In phagocytosis, specialized cells (phagocytes, macrophages, dendritic cells, etc.) collect large incoming particles and digest them with the assistance of lysosomes. Indigestible material then exits the cell through exocytosis 80 (Fig. 4A). Pinocytosis is the primary pathway by which particles are internalized by cells. There are four different pinocytosis mechanisms by which NPs and MPs may be internalized: macropinocytosis (Fig. 4B), clathrin-mediated endocytosis (Fig. 4C), caveolin-mediated endocytosis (Fig. 4D), and mechanisms independent of clathrin and caveolin. 78,79 Macropinocytosis is nonspecific and transports particles ≥1 μm into the cell through endolysosomal degradation. The last three forms of pinocytosis are collectively referred to as receptor-mediated endocytosis due to the use of receptor proteins to transport particles. Once the particles have been successfully internalized by the cell, the clathrin or caveolin and protein receptors are recycled back to the cell surface while the particles are then transported to the Golgi apparatus, endoplasmic reticulum, or lysosomes for elimination. 81 Clathrin-mediated endocytosis is primarily utilized for particles ≤100 nm, while caveolin-mediated endocytosis captures particles between 60 and 80 nm (Fig. 4). 79,81 Endocytosis mechanisms independent of clathrin and caveolin are known to exist, but are not yet fully understood.
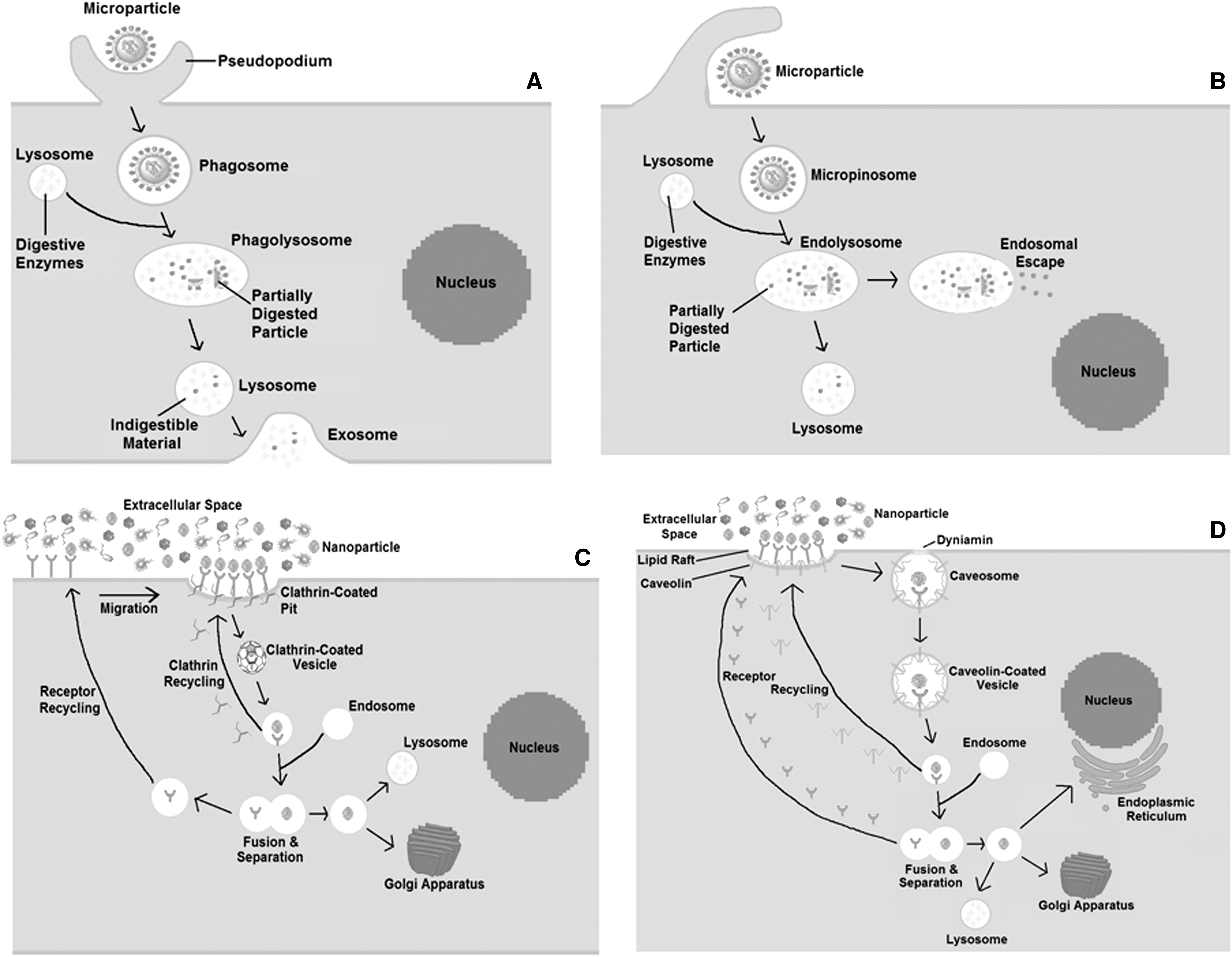
Uptake mechanisms of micro/nanoparticles.
Biodegradation and Elimination
Biodegradable polymeric MPs and NPs are frequently used in drug delivery and may be utilized for ocular applications. These polymers may be natural or synthetic, and the toxicity and method of degradation experienced by these polymers depend on their structure and properties. 82 Cross-linked water-soluble polymers (i.e., PVA) degrade through hydrolysis, resulting in soluble polymer chain fragments. Water-insoluble linear polymers (i.e., alkyl vinyl ether) undergo a process involving hydrolysis, ionization, or protonation to produce water-soluble fragments. 82 Water-insoluble polymers containing a hydrolytically unstable backbone (i.e., PLGA and PLA) degrade through hydrolytic cleavage into water-soluble fragments (Table 4). 83 The fragments produced by any of the methods are then excreted through biological waste pathways. For subconjunctival and systemic delivery, this is most often through choroidal blood and lymph circulation followed by metabolic clearance and renal excretion. 84 However, after intravitreal administration drugs and polymer fragments may be eliminated through either the anterior or posterior routes. The anterior elimination route involves diffusion through the trabecular meshwork into the aqueous humor where waste is then eliminated through aqueous outflow or uveal blood (Fig. 5A). 84 Posterior elimination routes require passage through the BAB or BRB and are only applicable to molecules and fragments <2 nm (Fig. 5B, C). Elimination rate is size dependent; small molecules will pass through the tight junctions of these barriers more quickly than larger molecules. 84
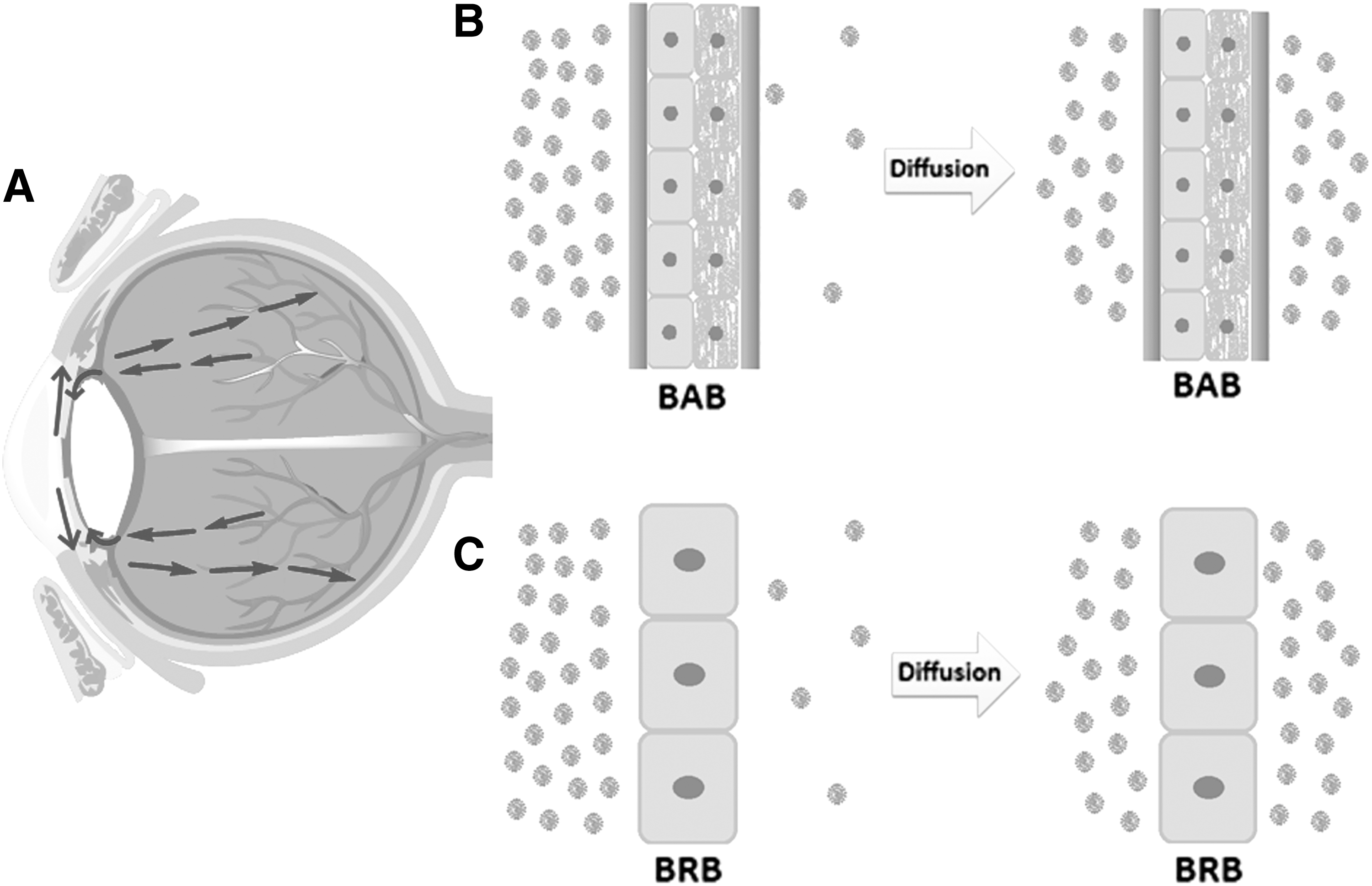
Elimination mechanisms of micro/nanoparticles from
Degradation of Polymers
Toxicity
The same properties which make MPs and NPs beneficial for ocular drug delivery have the potential to cause toxic side effects. 85 For instance, particles prepared using chitosan are generally well tolerated in ocular treatments but have been reported to induce inflammation in vivo. 86 In addition, PLGA has the potential to cause toxicity through drug-polymer interactions and inconsistent release rates. 87 However, it was unclear if this was caused by the particles themselves or by a natural immune response to the injection. Furthermore, the surface of the particles is involved in several catalytic reactions which could lead to toxicity, 88 including:
Interactions with the cell surface receptors can lead to stress response and formation of reactive oxygen species (ROS).
Interactions with mitochondria can destabilize the mitochondrial membrane or deregulate its potential disrupting oxidative phosphorylation.
Interactions with active proteins like nicotinamide adenine dinucleotide phosphate oxidase result in ROS production in the immune system.
Exposure to an acidic environment may degrade the NP or produce ions which induce the production of ROS species.
In addition, the size of the particles has been known to be a determining factor in cytotoxicity. For example, gold on the macroscale was determined nontoxic by the Joint Food and Agriculture Organization of the United Nations/World Health Organization (FAO/WHO) and Expert Committee on Food Additives (JECFA). 89 At the nanoscale level, however, gold presents high in vivo toxicity. In a recent study, gold NPs between 10 and 50 nm in diameter were more toxic than particles between 100 and 200 nm, thus confirming the theory that size is a determining factor in toxicity. 90
Conclusion
The utilization of MP and NP drug carriers for ophthalmic drug delivery will be able to combat the limitations of conventional treatment and provide patients with a more efficient comfortable means of treatment with reduced frequency of administration. Ocular neovascularization symptoms are most evident in the diseases of DR, RVO, AMD, and pathologic myopia. Proper retinal function requires high levels of energy and is greatly perturbed by variations in oxygen levels. Any reduction in oxygenation leads to the condition of hypoxia, which promotes increased HIF-1 expression. Although significant work is still needed in all domains of drug delivery for the treatment of ocular diseases, the progress made thus far is substantial. Researchers have been focusing on the development of novel drug delivery systems for ocular applications to combat poor bioavailability and low median residence time (MRT) within the desired site through the utilization of MPs and NPs. Discovering new treatments and improving on previous methodologies in the area of ocular disease treatment is a necessity. MP/NP drug delivery systems are a novel option to provide a more patient friendly administration with minimal side effects, reduced toxicity, prolonged MRT, efficient membrane penetration, minimal drug loss, and localization. 3
Footnotes
Disclosure Statement
The authors declare no conflicts of interest.