
Abstract
Antimicrobial resistance in disease-causing microbes is seen as a severe problem that affects the entire world, makes therapy less effective, and raises mortality rates. Dermal antimicrobial therapy becomes a desirable choice in the management of infectious disorders since the rising resistance to systemic antimicrobial treatment frequently necessitates the use of more toxic drugs. Nanoparticulate systems such as nanobactericides, which have built-in antibacterial activity, and nanocarriers, which function as drug delivery systems for conventional antimicrobials, are just two examples of the treatment methods made feasible by nanotechnology. Silver nanoparticles, zinc oxide nanoparticles, and titanium dioxide nanoparticles are examples of inorganic nanoparticles that are efficient on sensitive and multidrug-resistant bacterial strains both as nanobactericides and nanocarriers. To stop the growth of microorganisms that are resistant to standard antimicrobials, various antimicrobials for dermal application are widely used. This review covers the most prevalent microbes responsible for skin and soft tissue infections, techniques to deliver dermal antimicrobials, topical antimicrobial safety concerns, current issues, challenges, and potential future developments. A thorough and methodical search of databases, such as Google Scholar, PubMed, Science Direct, and others, using specified keyword combinations, such as “antimicrobials,” “dermal,” “nanocarriers,” and numerous others, was used to gather relevant literature for this work.
INTRODUCTION
The skin, the largest organ in human body, has a conducive surface area to facilitate medication absorption. In between the external environment and the host body, the skin acts as a defense. Soft tissues beneath the skin, including fat, fascia, and muscle, support the skin. 1 Skin serves the body’s many defensive and homeostatic purposes, including shielding it from hazardous substances, including chemicals, germs, heat damage, and radiation. In addition, the skin plays a crucial role in blood pressure and temperature control. The only organ in the host body with a multilayered structure is the skin, which would be essential for maintaining homeostasis. 2
Although it is acknowledged that the majority of the skin’s protective characteristics are found in the stratum corneum, the skin has a variety of unique biochemical properties and characteristics that support its antibacterial and permeation barrier activities owing to epidermal and dermal layers. The intact, unaltered stratum corneum acts as an impenetrable barrier to microbiological infiltration in its capacity as an antibacterial shield. The bioactive lipids constituting stratum corneum specifically ceramides and cholesterols create specific permeability barriers and function as the main protective barrier for the entire morphology. 2
A normal flora of bacteria, including Staphylococcus, Propionibacterium, and Corynebacterium species, and yeasts that live inside the skin, is colonized on the skin. 3 The skin protects against microbial infections by producing fatty acids and sebaceous secretions from hydrolyzing sebum lipids. 4 However, wounds, burns, scratches, needle injections, lacerations, and other skin breaks allow infectious organisms and natural flora to enter the body 1 and skin becomes prone to skin and soft tissue infections (SSTIs). 5 SSTIs can range in severity from minor to serious illnesses. 6 With a 71% surge in hospital admissions, SSTIs are thought to be the most common disease. 7
Antimicrobial peptides (AMPs), secreted in skin layers, also provide defense against infection. Skin AMPs are produced by keratinocytes, sweat glands, etc. These are small peptides (<10 kDa, 12–50 amino acids) and function through a defined high-affinity antimicrobial target. Some of the famous peptides are nisin, gramicidin from Lactococcus lactis, Bacillus subtilis, and B. brevis.
Although the stratum corneum is the main location, they are usually produced in other epidermal layers. The skin’s intrinsic defensive mechanisms rely heavily on the AMPs, particularly defensin and cathelicidin, which are typically tiny cationic polypeptides. In addition, they influence the generation of chemokines and cytokines, wound healing, and inflammation. 8
COMMON MICROORGANISMS THAT CAUSE DERMAL BACTERIAL INFECTIONS
Staphylococcus aureus and methicillin-resistant S. aureus
A gram-positive member of the Staphylococcaceae family, Staphylococcus aureus forms an asymmetrical grape-like cluster when it grows. 9 Common human skin, intestinal tract, throat, and nasal passage infections by S. aureus do not harm the host. 10 S. aureus is present in the nose, skin, and mucous membranes of 15%–40% of fit human beings, 11 however, S. aureus can easily get inside the body via skin burns, surgical wounds, and skin breaks, causing minor SSTIs. S. aureus infections can lead to cellulitis, impetigo (superficial pyogenic inflammation of epidermis), and folliculitis, which is marked by clusters of small, erythematous pustules or papules in hair follicles. 5,12 Penicillin G (a β-lactam antimicrobial), discovered to be effective in the management of bacterial infection, was first introduced in the early 1940s in response to the rise of infections brought on by S. aureus. However, soon after the β-lactam antimicrobial was introduced, S. aureus was found to be resistant to it. The enzyme β-lactamase, which inactivates the β-lactam, is produced by resistant bacteria. 13 To solve this problem, methicillin (a semisynthetic penicillin) first developed in 1959. Penicillin-binding proteins (PBPs) in the cellular membrane interact with methicillin to prevent the cross-linking of peptidoglycan chains in the cell wall. 14 However, barely two years after methicillin was first introduced and utilized in clinics, methicillin-resistant S. aureus (MRSA) bacteria evolved in 1961.10 By the late 1980s, over 95% of S. aureus strains worldwide had developed resistance against penicillin. 15 To survive in clinically relevant concentrations of β-lactam antimicrobials, MRSA creates a different PBP, PBP2a, which is generated by the mecA gene and has a decreased affinity with this class of antimicrobials. The PBP2a in MRSA facilitates the continuing synthesis of cell wall components in the presence of β-lactams. 13 The prevalence of SSTIs linked to S. aureus ranged from 23% to 61%, with MRSA making up about 25%–74% of isolates.
Streptococcus pyogenes
Streptococcus pyogenes, often known as Group A Streptococcus (GAS), is a species of gram-positive streptococcal bacterium that frequently results in SSTIs, including transient cutaneous and oropharyngeal infections. 16 S. pyogenes infections are extremely infectious. Airborne droplets, coming into contact with nasal discharge, touching infected objects or surfaces, contact of the skin with infected lesions, and affected food sources can all result in the spread of bacteria. It can enter the skin through abrasions or skin sores and cause cellulitis or erysipelas. 17 The illness causes sepsis in both children and adults frequently, has a significant mortality rate, and accounts for at least 150,000 fatalities a year globally. 18 The drug of first choice is penicillin and patients who experience β-lactam drug allergies can use macrolides instead of penicillin. 19 S. pyogenes caused SSTIs with a 4%–32% occurrence and a 1%–3% resistance rate. According to reports, S. pyogenes can develop resistance to macrolides 20 and have decreased susceptibility to penicillin and its analogs. 21 In the 1950s, the first report of a macrolide-resistant S. pyogenes was published. 22 According to a study, S. pyogenes isolates obtained at the University of Iowa Hospitals and Clinics in the United States between January 2011 and September 2012 caused necrotizing soft tissue infections that were resistant to antimicrobials. Seven isolates (30%) of S. pyogenes strains were resistant to erythromycin, eight isolates (35%) were resistant to clindamycin, and seven isolates (30%) were tetracycline resistant. 23 A total of 124, that is, 42% of the 299 GAS isolates gathered in Japan between 2011 and 2013 were resistant to macrolides. Clarithromycin, clindamycin, and azithromycin resistance rates were 42%, 43%, and 16%, respectively. A maximum of 101 specimens, that is, 34% exhibited strong erythromycin resistance (minimum inhibitory concentration [MIC] ≥16 µg/mL). Erythromycin’s MIC 50/90 values for the 299 GAS isolates were 0.25 ≥ 128 µg/mL. 19
Pseudomonas aeruginosa
Pseudomonas aeruginosa, a proactive gram-negative type of bacteria, disproportionately affects immunocompromised people such as those with cancer, diabetes, HIV infection, transplants, cystic fibrosis, severe burns, implants, or those receiving corticosteroids and antimicrobials, accounting for 10% of hospital illnesses. 24 P. aeruginosa colonizes the interdigital space and moist, macerated skin and is a common nosocomial pathogen (similar to burns and wounds). Together with mucous membranes and healthy human skin, it may also infect cats and dogs. 25 P. aeruginosa uses the type III secretion system, a specific sort of cellular poisoning, to slow down the innate immune system’s rapid response to invading bacteria by killing host phagocytic cells while releasing activator toxins inside eukaryotic cells. 26 P. aeruginosa has the capacity to adjust to its environment to encourage colony growth in biofilm. This increases the pathogen’s chance of survival and shields it from the host’s immune system and antimicrobial treatments. 27 With a frequency of 14%–62% and a tolerance rate of 7%–48%, P. aeruginosa developed SSTIs. P. aeruginosa develops β-lactam antimicrobial resistance (AMR) by overexpressing the efflux pump, membrane porin, inducible AmpC chromosomal β-lactamase, and lateral gene transfer. 28 In a research, all P. aeruginosa isolates displayed resistance to imipenem, ceftazidime, meropenem, ciprofloxacin, and tobramycin, whereas more than half of P. aeruginosa isolates were resistant to aztreonam and piperacillin. 29 Of the 31 P. aeruginosa samples examined, 48% had carbapenem resistance. All of the carbapenem-resistant P. aeruginosa isolates showed imipenem MIC values greater than 32 µg/mL. 30 P. aeruginosa is also a key contributor to the slow healing of wounds. According to a meta-analysis study, chronic nonhealing wounds with 78.2% of the biofilms present had poor wound healing. It was detected Multi drug Resistance (MDR) P. aeruginosa in 58.6% of clinical specimens taken from injured individuals. Therefore, improved therapeutic and preventative approaches are needed to address MDR P. aeruginosa infections of wounds. 31
Escherichia coli
Escherichia coli, a gram-negative bacteria of the Enterobacteriaceae family that inhabits human digestive systems, is a common cause of SSTIs and urinary tract infections. 32,33 Enterobacteriaceae isolates are resistant to broader spectrum β-lactam antimicrobials because plasmid-mediated enzyme synthesis renders medications inactive by hydrolyzing their β-lactam rings. 34 Approximately 3%–15% of SSTIs were caused by E. coli and up to 28% of cases were resistant. According to Fan et al., the rate of ciprofloxacin resistance has dramatically grown in the E. coli strains isolated over the study period (during 2002–2006, the increase was reported to be 30%). 35 The prevalence of ampicillin resistance was 96% for the years 2009–2010 and 100% for the years 2011–2013 among 26 hospitalizations in China with difficult SSTIs affected with E. coli. The rate was likewise over 80% for the years 2009–2010 for ceftriaxone, ceftazidime, aztreonam, cefepime, and piperacillin. 36 In the SENTRY Antimicrobial Surveillance Program’s 13526 E. coli isolates that were gathered throughout 2014 and 2015 in Latin America, the Asia Pacific region, North America, and Europe, 59 E. coli strains were resistant to colistin, with MICs of less than 4 µg/mL. 37
Klebsiella pneumoniae
The gram-negative bacterium Klebsiella pneumoniae is a significant proactive pathogen in pancreatic abscesses, bloodstream infections, respiratory tract infections, intestinal infections, and infections of the operative site and wound. 38 Serum complement proteins, that are bactericidal, and polymorphonuclear granulocytes, that phagocytose the pathogens, are the two key components that protect the host from bacterial invasion. The defense against K. pneumoniae infection is aided by neutrophil myeloperoxidase and lipopolysaccharide-binding proteins. 39 Bacteria have a polysaccharide capsule made up of complex acidic polysaccharides, which determine their pathogenicity. This capsule protects bacteria from phagocytosis and serum bactericidal proteins. It adheres to host cells with many fimbrial and nonfimbrial adhesions, which is critical to the infectious process. Genes producing extended-spectrum β-lactamase are frequently found in K. pneumoniae, and they play a crucial role in the organism’s resistance to antimicrobials. 34 K. pneumoniae SSTI rates ranged from 6% to 10%, and up to 6% of patients developed resistance. Cefoxitin, cefotaxime, chloramphenicol, colistin, gentamicin, polymyxin B, trimethoprim, rifampicin, imipenem, ceftazidime, and meropenem were the 11 antibacterials that Abuzaid et al. examined, along with five biocides (benzalkonium chloride, chlorhexidine, MediHex-4, Trigene, and Medisc). Several strains showed resistance to rifampicin (having MIC up to 64 mg/L for all cases), cefotaxime, chloramphenicol, ceftazidime, and trimethoprim (having MICs up to 128 mg/L for all cases). It was discovered that Trigene, benzalkonium chloride, and chlorhexidine susceptibility was significantly reduced (MICs varied between 32 and 128 mg/L). 40 Zaman et al. discovered that all isolated strains of K. pneumoniae were resistant to ceftazidime, cefepime, cefotaxime, ciprofloxacin, and piperacillin–tazobactam (having MICs up to 256 g/mL), whereas 91% (21/23) of the isolated strains of K. pneumoniae were resistant to amikacin and gentamicin. 41 A total of 331 of the 7,480 K. pneumoniae isolates collected in Europe, the Asia Pacific area, North America, and Latin America for the SENTRY Antimicrobial Surveillance Program in 2014 and 2015 were colistin-tolerant, with colistin MICs of less than 4 µg/mL. 37
ANTIBIOTICS
Antibiotics are substances created by living tissue to fight infections, and man has modified them to fight off single-celled predators. 42 It is derived from natural sources such as bacteria, molds, and other microorganisms. It is regarded as one of the greatest scientific and technological achievements.
Penicillin, the first extensively utilized antimicrobial was found in 1928. Alexander Fleming cautioned in 1945 that the wonder of antimicrobials might be destroyed by bacterial resistance. 43 Beta-lactam antimicrobials were developed shortly after and quickly showed their effectiveness against penicillin-resistant organisms. 44,45 Following the identification of MRSA, records of resistance to almost all currently prescribed medications have been made. 46 Enterococcus faecium, S. aureus, K. pneumoniae, Acinetobacter baumannii, P. aeruginosa, and Enterobacter (ESKAPE) species are among the high-priority ranking antimicrobial-resistant organisms that need immediate treatment. The World Health Organization (WHO) has classified 12 microbes as critical to medium prioritized diseases, including the ESKAPE (WHO). 44,45
Antimicrobial resistance
The WHO defines AMR as the capacity of a pathogen (including viruses, bacteria, and some parasites) to resist the effects of antimicrobials (such as antimicrobials, antivirals, and antimalarials) (WHO, 2021). Standard treatments stop working as a result, and infections continue and could spread to other people. Since it only relates to resistance to medications used to treat bacterial illnesses, the term “antimicrobial resistance” is more specific. According to the WHO (2014), AMR affects numerous infections and is widespread around the world. To acquire quantitative data on AMR, Hendriksen et al. (2019) used a metagenomic analysis of domestic sewage from 79 locations worldwide to support their assertion. 47
AMR makes it difficult to use Antimicrobial Agents (AMA) as it leads to treatment failure. As a result, research is being decreased on AMA formulation. The main causes of this reduction are systemic infections and associated resistance. The topic of AMA research becomes even less intriguing because of the high cost and length of time required for new drug creation. 42
End users’ ignorance of the consequences of improper use and management of antimicrobials led to the development of resistant bacteria over time. Resistant genes can develop as a result of unintended DNA changes that can be transmitted through vertical gene transfer from parents to children or as a result of transposons, plasmids, and bacteriophages that resemble foreign DNA being spread horizontally. This resistance Fleming referred to as acquired resistance, and it represents the success of selective pressure. Moreover, there is also a type of resistance known as intrinsic resistance, in which genetic traits give all members of a particular bacterial genus the inherent ability to resist the action of an antimicrobial as a consequence of the structural or functional attributes of the bacteria. 48 These characteristics are unrelated to previous antimicrobial exposure.
Multidrug resistance, or the concurrent resistance development to several antibacterial drugs, is the main problem with antimicrobials. This may occur when a particular bacterial strain carries a variety of resistance genes, each of which imparts resistance to a particular antimicrobial or it could happen when a single resistance mechanism provides resistance to a number of distinct antimicrobials. These kinds of bacteria are referred to as “superbugs” as they can cause infections that are resistant to treatment with regular antimicrobials.
There are several choices among the inherent or acquired ways by which microbes can evade the fatal effects of antimicrobials (Fig. 1 ).
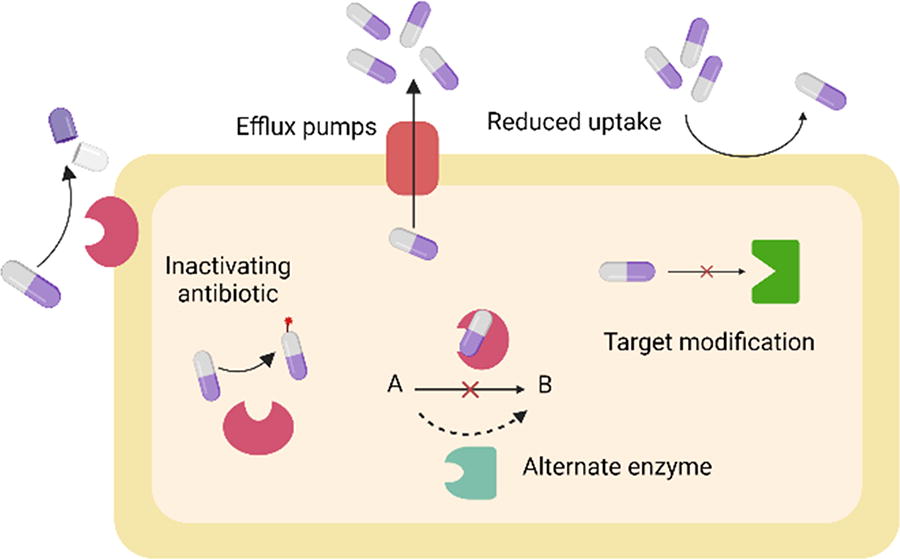
Illustrating the mechanisms by which bacteria develop resistance to antibiotics: (1) antibiotic absorption is decreased; (2) antibiotic efflux is increased; (3) antibiotics are inactivated; (4) target alteration occurs; and (5) alternative metabolic pathways are developed. Comprehending these pathways is essential for formulating tactics to counteract antibiotic resistance. 49,50
Reduction of antimicrobial uptake by bacterial cells
Big polar molecules cannot penetrate the cell of gram-negative bacteria due to a semipermeable barrier on their exterior membrane. Porins, which are protein channels, are the means by which many antimicrobials and other small polar compounds can penetrate the bacterial cell. The concentration of the medicine at the target site can be decreased if bacteria lose or mutate such channels, which will slow or stop the drug’s entry into the cell. This is the mechanism of action of AMR in gram-negative bacteria against β-lactams, chloramphenicol, and tetracyclines. 49,50
An increase in the antimicrobial’s efflux from bacterial cells
All cell types have cytoplasmic membranes that contain protein transporters known as efflux pumps. They require a chemical energy source to operate since they are active transporters. Antimicrobials can be expelled by hyperexpression of efflux pumps in microorganisms. A prominent resistance mechanism against tetracyclines, macrolides, chloramphenicol, and fluoroquinolones is enhanced efflux. 49,50
Making antimicrobials inactive
Antimicrobial degradation or inactivation is a typical resistance mechanism. The development of an enzyme able to inactivate aminoglycosides, macrolides, β-lactams, and chloramphenicol is typically the cause of bacterial resistance to these substances:
Target modification
Modifications in the target protein’s amino acid content and/or conformational changes can result from mutations in the genes that code for the antimicrobial targets. A drug’s affinity toward its target or a prodrug’s affinity for such an enzyme that converts a prodrug into an active drug may be decreased by such alterations. Various modifications to the natural target, such as ribosomal protection against tetracyclines and macrolides, mutations in the target (such as fluoroquinolone resistance), or even the acquisition of a resistant variant of the native sensitive target can all lead to these changes. For example, the production of a certain PBP (PBP2′, PBP2a, or MecA) causes staphylococcal resistance to methicillin. 49,50
Alternate metabolic pathway development
The most extreme forms of resistance include intricate metabolic adaption processes and other modifications, similar to those found in enterococci that are resistant to vancomycin and staphylococci that are resistant to methicillin. Vancomycin resistance has a connection to the metabolic reorganization of the cellular membrane. Vancomycin attaches with great intensity to D-Ala-D-Ala repeats at the end of the peptidoglycan peptides in normal bacteria, preventing the mechanism of wall formation. Resistant bacteria can make peptidoglycan having changed chemical structure and D-Ala-D-lactate terminal repeats (and similar structures such as D-Ala-D-Met and D-Ala-D-Phe). Vancomycin has a thousand times stronger affinity for the D-Ala-D-Ala dipeptide than it does for D-Ala-D-lactate. The antimicrobial cannot prevent the growth of the bacterium that produces the changed peptidoglycan as a result of its diminished affinity for the modified target. Neisseria meningitidis and S. aureus increased the production of para-aminobenzoic acid (PABA), competing molecule of these medications, which is yet another example of metabolic pathway changes. The lesser the sulfonamide binds to dihydropteroate synthase, the more PABA is generated. 49,50
DERMAL USE OF ANTIMICROBIAL AGENTS
Topical application of antimicrobials is a preferable course of treatment for infections of the skin and soft tissues due to a targeted approach and elimination of systemic complications. Dermal antimicrobial medications can be used to treat colonized or infected areas directly, aiding in SSTI prevention and the treatment of mild to moderately serious SSTIs. Dermal drug delivery techniques include colloids, solutions, lotions, suspensions, semisolids (such as gels, creams, foams, pastes, and ointments), solids (such as powders and aerosols), sprays, transdermal patches, and transdermal administration methods (a drug reservoir that may have drug release-controlling membrane, such as nanoparticles [NPs], liposomes, and microcapsules). 51 When compared with oral or intravenous administration, dermal antimicrobials have many benefits for patients such as the removal of enzymatic hydrolysis and quick clearance in the digestive tract or first-pass metabolism when given orally; absence of physical pain and discomfort that is apparent with intravenous injection; reduction of drug interactions and systemic adverse effects; enhanced treatment adherence and comfort; and also decreased cost of treatment. 1 Local delivery can restrict the possibility of systemic antimicrobial absorption, hence lowering AMR.
Dermal antimicrobial preparations have lower systemic toxicity, provide higher concentrations of drug at the site of SSTIs, and are just as effective as systemic antimicrobials in treating the condition. 52 Even while the dermal drug delivery route of antimicrobials has numerous advantages over oral and systemic administrations, it is not risk-free since drug movement throughout the layers of the skin, hair follicles, and the appendage glands later culminates in the systemic circulation. Many of these negative consequences could be the result of drug toxicity or overdose. 53 To prevent the risks of systemic adverse effects, dermal preparations should be given using a small yet effective dose.
NANOCARRIERS FOR DERMAL DELIVERY OF ANTIMICROBIAL AGENTS
Nanocarriers have been used in a wide range of biomedical applications and have shown to be efficient drug delivery systems and a potential carrier for antibacterial agents. The development of AMPs with increased action against MDR bacteria has been largely attributed to the use of NPs such as Metallic nanoparticles (MNP)s, polymers, dendrimers, liposomes, and nanostructured lipid carriers (NLCs). However, AMPs have been found to have limitations, including cytotoxicity, stability profiles, conjugation procedures, and shelf life. Liposomes can trigger an immunological response and have a poor loading capacity. Although liposomes are biocompatible and can be loaded with both hydrophilic and hydrophobic medicines, issues such as drug-loading effectiveness and immunogenicity continue to be problematic. Monodispersed molecules having a great degree of control over the crucial molecular design parameter are dendrimers. Dendrimers continue to be severely constrained by the expense of synthesis and its generality. Research has documented polymeric NPs’ biocompatibility and environmental biodegradability. It is simple to alter and regulate medication release in this type of carrier. As a useful and intriguing alternative, the use of nanocarriers to broaden the selection of medications available for transdermal delivery has evolved. Through the stratum corneum, both lipophilic and hydrophilic medications can be administered with the potential of having a local or systemic activity to treat a variety of disorders. 54 Nanocarriers as drug carriers can potentially enhance drug specificity, bioavailability, and therapeutic efficacy while improving patient compliance during therapy. Besides, NP-based drug delivery can enhance drug retention with tunable release kinetics at the disease site inside the skin. Table 1 and Figure 2 describe the different types of nanocarriers utilized for dermal antimicrobial delivery. Table 2 lists various benefits and drawbacks of nanocarrier systems for topical distribution of antimicrobials.
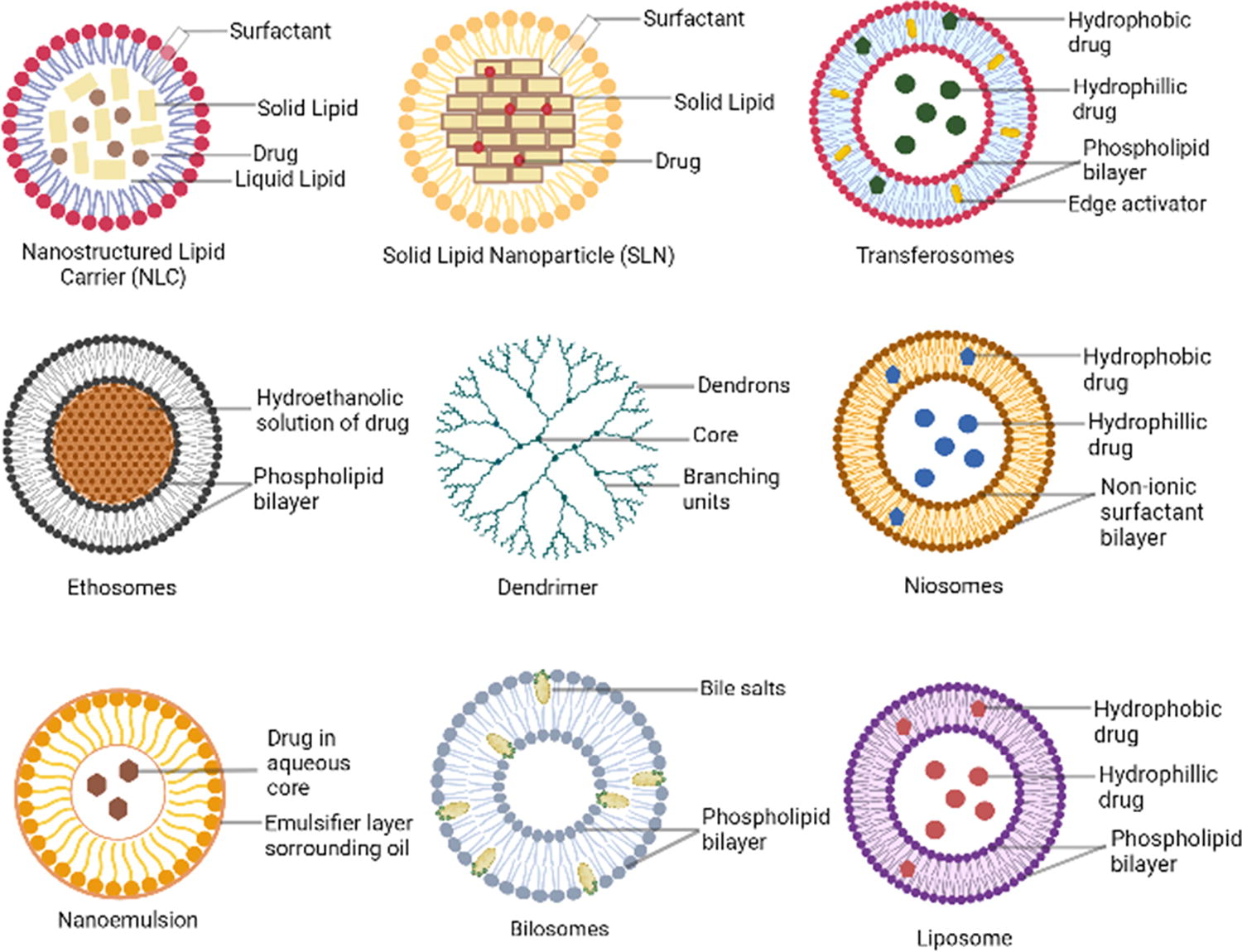
Summarizing the various types of nanoparticles used for dermal delivery. These include nanostructured lipid carrier (NLC), solid lipid nanoparticles (SLNs), transfersomes, ethosomes, dendrimer, niosomes, nanoemulsion, bilosomes, and liposomes. 54
Nanocarriers for Dermal Delivery of Antimicrobial Agents
AgNP, silver nanoparticle; AuNP, gold nanoparticle; Fe3O4-Ag, silver-coated magnetite nanoparticle; MRSA, methicillin-resistant S. aureus; MSNs, mesoporous silica nanoparticles; NLCs, nanostructured lipid carriers; PEG, polyethylene glycol; PLGA-HPMA, poly (lactic-co-glycolic acid)-N-2-hydroxypropylmethacrylamide; PMLA, polymaleic acid; SLNs, solid lipid nanoparticles; SME, soyaethyl morpholinium ethosulfate.
Benefits and Drawbacks of Nanocarrier Systems for Topical Distribution of Antimicrobials
Nanostructured lipid carriers
NLCs are a redesigned dosage form of solid lipid nanoparticles (SLNs) that have a core matrix made up of both solid and liquid lipids. Compared with SLNs, NLCs demonstrated greater storage stability and improved encapsulation efficiency. 55 NLCs offer controlled drug release through the lipid matrix while safeguarding the active ingredients from deterioration. Because of their large capacity to load drugs and site-specific distribution, they show enhanced delivery of the drug. 56 The drug solubility used in the production of medicines, food products, and cosmoceuticals is said to be improved by them. 57
Upon initial NLC manufacturing, roughly 5% of the drug (by weight) is typically included in the lipid mixture, and about 3%–4% drug loading is accomplished (with average encapsulating efficiencies of around 70%). Stearic acid, monostearin, glyceryl dilaurate, hydrine, cetyl alcohol, glyceryl monostearate, and Imwitor 900 are examples of common solid lipids used; Capmul, oleic acid, glyceryl mono-dicaprylate, and caprylic/capric triglycerides are common liquid lipids used. 58 There were uncountable researches undertaken pertaining to NLCs. However, few of them with outstanding outcomes have been elaborated in Table 3.
Researches Pertaining to Nanocarriers and Their Results Obtained
MIC, minimum inhibitory concentration.
Solid lipid nanoparticles
SLNs are composed of solid lipid matrices and are biocompatible/biodegradable. 59 For a variety of reasons, SLN are intriguing lipid-based drug delivery vehicles, the particle size of SLN is at the nano- to submicron scale (10–1000 nm) after drug encapsulation. They do not need the utilization of organic solvents for their manufacturing, and finally, the particle synthesis method (e.g., high-pressure homogenization) could be carried out at a lower cost. 58 SLNs have the benefits of colloid carriers and can be utilized to prolong the release of lipophilic drugs and increase drug bioavailability. 59,60
Due to the drug being directly targeted to the site of action, SLNs have a significant degree of stability and lower toxicity in the surrounding tissues. 61 Fabrication of SLN in powder form, which can then be added to tablets, capsules, or pellets to improve medication delivery, is another benefit. It is important to remember that the undesirable particle growth caused by agglomeration or coagulation, which causes a quick “burst release” of the drug, may restrict the use of SLN formulations. The loaded medicine can be accommodated in SLN’s flawless crystal lipid matrices, which are sandwiched amid fatty acid chains. The expulsion of the drug-loaded solution occurs frequently as a result of the development and strengthening of the crystal structure throughout SLN manufacture and storage, which is a significant drawback of such NPs. 60 There are certain other pertinent researches that were carried out and governed by optimistic results, as shown in Table 3.
Liposomes
Liposomes are circular, semipermeable vesicles made up of phospholipids, or amphiphilic lipids, organized to create one or more lamellae or concentric bilayers partitioned by aqueous compartments with a core aqueous volume that is trapped. The external or internal aqueous environment is in contact with the hydrophilic portions of phospholipids, whereas the hydrophobic moiety is in contact with one another. Liposomes are regarded both as NP and microparticle systems due to their vast range of sizes from 20 nm to several micrometers. Since its inception, liposomes have grown to be the most extensively researched and widely used drug-delivery systems for topical and systemic administrations. They make excellent carriers for both hydrophilic compounds found within the central hydrophilic core or within the spaces between lamellae and for hydrophobic compounds that can be incorporated into lipid bilayers. Liposomes can be categorized as multilamellar vesicles (MLVs) (>0.5 μm), oligolamellar vesicles (0.1–1 μm), large unilamellar vesicles (LUVs) (>0.1 μm), and the small unilamellar vesicles (SUVs) (0.1 μm) depending on the number and size of bilayers. Every type of vesicle has a standard aqueous/lipid ratio value; the greater the ratio, such as in LUVs, the higher the capacity to carry water soluble drugs, while the vesicles with a lower aqueous/lipid ratio, such as in SUVs and MLVs, are ideal for carrying hydrophobic drugs, such as many antimicrobials. 62 Liposomes are immensely popular as drug carriers due to a number of benefits, including the fact that they are nontoxic and biodegradable due to their components being comparable with that of biological membranes, which are composed of natural or synthetic lipids. Second, the ability to precisely modify the size, lipid content, surface charge, and surface changes to provide improved circulation half-life, manageable release kinetics, and focused drug administration makes the liposomal system particularly ductile. Liposomes are masking devices, or “Trojan horses,” as Bangham used to refer to them, that allow protecting integrated active components from any degradation. Their ability to form a fusogenic membrane is another highly intriguing characteristic; in fact, their lipid bilayer structure enables them to easily combine with all biomembranes, including the bacterial ones. 63 This characteristic enables liposomes to acquire effective intracellular concentrations in cases of intracellular infections, overcoming one of several antimicrobials’ major limitations and preventing the development of AMR. Due to all of these factors, liposomes are among the most popular, patented, and licensed drug delivery systems for clinical usage. 64 Because of their low therapeutic index, significant side effects, and resistance mechanisms, various antifungal, anticancer, antimicrobial, and antiviral agents are undoubtedly among the drugs that can benefit from being delivered by liposomes. Regarding antimicrobials, liposomes are a way to deliver multiple drug ingredients that work synergistically to fight infections. They can deliver multiple drug ingredients that combat synergistically to overcome resistance, eliminate forms of resistance such as biofilms, and enhance concentration of drug at the sites of infection. 65 Table 3 represents certain other researches that need to be brought forward.
Ethosomes
A new variety of ultradeformable vesicles (UDV) called ethosomes were created by Touitou et al. (1997). 66 They are also known as elastic nanovesicles because of their size (between 150 and 200 nm) and remarkable deformability. 67 The vesicular networks known as ethanolosomes are made up of ethanol, phospholipid, and water. 68 Various phospholipids, that is, natural, semisynthetic, and synthetic origin, including soybean and egg, can be used in concentrations ranging from 0.5% to 10%. Phospholipid examples are phosphatidylethanolamine, hydrogenated phosphatidylcholine, and phosphatidylinositol. When used between 20% and 45%, ethanol works well to improve permeation through skin. The melting point of the stratum corneum lipid is lowered as a result of this molecule’s interaction with the polar head group, improving the mobility of lipid bilayers and cellular membrane permeability. 68 A perfectly elastic vesicle membrane is produced by the high ethanol content, which is beneficial for improved skin delivery. In addition, the formulation’s use of ethanol promotes the development of lamellar-shaped vesicles, which have been shown to enhance the solubility and trapping of a variety of medications, such as minoxidil and testosterone. Due to interactions between the formulation’s high ethanol concentrations, the phospholipids found in the vesicular membrane, and skin lipid molecules, ethosomes have been demonstrated to increase the skin permeability of numerous drugs. When ethanol binds with polar head of skin lipids, the stratum corneum’s lipid domains become less rigid. Skin permeability may have increased due to the liquid crystalline state’s greater fluidity. It is also thought that ethanol makes ethosome vesicles more elastic, making it easier for them to move through the lipid channels and pores in the stratum corneum. At various locations along the pathway of penetration, the fusing of vesicular membranes to skin lipids is anticipated to have an impact on drug release. 69 Table 3 puts forth a few additional commendable researches and their remarkable outcomes.
Dendrimers
The dendrimers are symmetrical highly branched macromolecules that have branching units that branch out from a central nucleus in all directions and end in surface-level functional groups. Dendrimer derives from the Greek term “dendron,” which not only refers to trees but also to neuronal dendrites. It describes a defined topological arrangement and the organized and hyperamified nanostructure that resembles a tree. 70,71 As a result, the number of potential dendrimer structures that can be created increases exponentially. Dendrimers are created by repeatedly condensing the same unit using either divergent (from the center to the perimeter) or convergent (from the peripheral to the nucleus) synthetic methods, producing up to a size of 2–5 nm. 72 As a result, a globular form made up of three structural zones is implemented: the center nucleus or multifunctional core, the branches connecting to the center known as “dendron,” and lastly the periphery’s active sites. 72
Given that certain dendrimers, such as cationic dendrimers, have demonstrated inherent antibacterial properties, dendrimers represent new prospects as nanobactericides (the nanoformulations exerting bactericidal actions) as well as nanocarriers that can enhance the therapeutic action of conventional antimicrobial compounds. Due to their ability to electrostatically interact with negative-charged bacterial envelopes, positive-charged nanomolecules are known to have antibacterial potential. As a result, biocidal dendrimers are positively charged and have functional groups such as amine or tetra alkyl ammonium, whereas anionic dendrimers are ineffective. 72 PAMAM dendrimers disrupt the membrane and result in the loss of cytoplasmic contents after electrostatic interactions with bacterial surfaces. 73 They are effective against both resistant and susceptible bacteria. Conversely, bactericidal dendrimers exhibit cytotoxicity toward mammalian cells in addition to the beneficial microbicide effect. Studies were performed where they changed the amine group of cationic PAMAM dendrimer with PEG linkers to get around this problem while maintaining therapeutic efficacy. Because it enables the creation of high surface levels, functional dendrimers with the quaternary ammonium salt boost their antibacterial efficacy in comparison with the identical nonassociated salts. In vitro tests on S. aureus, E. coli, and P. aeruginosa revealed significant antibacterial activity for PAMAM dendrimer complexes and silver-PAMAM dendrimer nanostructured materials. 74 They have been investigated as an antibacterial coating because polyglycerol dendrimers made with chitosan and functionalized with boron were very viscous, biodegradable, and efficient against S. aureus. When an AMP is created in dendrimer form, its durability to protease and peptidases is increased, and its antimicrobial activity is increased in comparison with its monomeric form. In solution, amphipathic dendritic dipeptides self-assemble and function as proteins that generate pores in membranes, hence changing permeability. The antimicrobial compound dendrimer G3KL, which is only made of naturally occurring lysine and leucine residues alternated in the branches, has been shown to be potent against multidrug-resistant A. baumannii and P. aeruginosa while being only slightly harmful to human red blood cells. 75,76
According to Kalomiraki et al., dendrimers can encapsulate small therapeutics, metals, or imaging moieties, which can fit inside their branches, and their spherical form allows them to interact via hydrogen bonding, lipophilicity, and charge interactions. Aside from their structure, dendrimers’ capacity to efficiently permeate cell walls due to their size and lipophilicity may make them suitable drug delivery vehicles for numerous therapies. 77 Abdel-Sayed et al. discovered that polycationic dendrimers can have an antiangiogenic influence on burn wounds. Three generations of AMP dendrimers (AMPDs) were created by dispersing the amino acid residues L-lysine (G3KL) and L-arginine (G3R) across the branches. It was shown that AMPDs, G3KL, and G3R could be safely utilized in conjunction with biological bandages formed of progenitor skin cells to prevent P. aeruginosa infection and promote wound healing in keratinocytes and endothelial cells. 78 Other promising researches have been mentioned in Table 3.
Nanosponges
β-cyclodextrin-made nanosponges (NS) claimed to increase the solubility of Biopharmaceutics Classification System (BCS) class II and class IV drugs. 79 Drug delivery, biocatalyst, as well as the adsorption of harmful substances have all been studied using NS. 80 To boost the bioavailability and solubility of poorly soluble medications, there has recently been an increase in interest in developing drug delivery systems based on NS. 79,81 NS has been demonstrated to be an inventive spherical nanocarrier with large porous surfaces and vast cavities that can accommodate both hydrophilic and lipophilic pharmacological moieties, 82,83 and circumvent the limitations of drugs. 83,84 Prepared nanomatrix could be administered topically, parenterally, and orally. 84 Cyclodextrin nanosponges (CDNS), a type of nanocolloidal carrier, have a number of advantages over other cargos, including large drug loading, long-term stability, a high solubilization capacity, extended-release, and the simplicity of scaling up. 85 The research community has become increasingly interested in this prospective drug delivery method. NS are an intriguing alternative to conventional carriers for medications with low water solubility. However, one of the most significant drawbacks of topical NS is the discomfort associated with their direct application to the skin due to their particle structure. NS made of cyclodextrin can be incorporated into a variety of topical products, such as creams, gels, or ointments, in this regard. Furthermore, Argenziano et al. created semisolid preparations of imiquimod-loaded NS and evaluated their potential for cutaneous delivery. The ability of β-cyclodextrin NS to target the action of highly permeating drug molecules in the skin’s exterior regions was also demonstrated by this group. These adaptable carriers, which have pores and a nanosize range of 200–500 nm, can entrap both hydrophobic and hydrophilic medicines. 86 A range of crosslinkers and cyclodextrins are combined in predetermined molar ratios to form cyclodextrin NS. According to published research, carbopol hydrogels with NS incorporated in them improve drug absorption in the targeted area of skin. 86,87 The hydration process used by hydrogels to increase medication administration into the skin is well documented. 88 There were uncountable researches undertaken pertaining to NS. However, few of them with outstanding outcomes have been elaborated in Table 3.
Niosomes
Niosomes are highly organized bilayer structures of amphipathic molecules that form when nonionic surfactant and cholesterol self-assemble in aqueous conditions. 89 These carriers might be useful for creating medication reservoirs in the epidermis. Today, more than 50% of drug candidates have poor water solubility 90 ; niosomes can increase the solubility of the molecule with poor aqueous solubility. These submicroscopic amphiphilic drug transporters improve the controlled release of medications to a specific area, the enhancement of drug deposition within skin, and the gradual release of drugs from a carrier during therapy. Drugs delivered topically using niosome carriers may exhibit cellular interaction with the epidermal tissues, prolong drug residence duration in the stratum corneum through regulated drug release, and minimize systemic toxicity. 90 Desoximetasone was encapsulated in niosomes by Parinbhai Shah et al. in 2021, which altered the drug’s release, possibly eliminating unfavorable side effects brought on by drug accumulation, and reduced the need for repeated application of the treatment. Desoximetasone-loaded niosomes were integrated into a gel formulation to allow for enough skin contact time. 91 The primary disadvantage of niosomes, however, is physical instability while storage, which results in the encapsulated medication being aggregated, fused, sedimented, and leaked. As a result, a groundbreaking pro-vesicular system known as “proniosomes” was created. Proniosomes are niosome hybrids made of liquid crystalline compact or dry-formulated particle carriers covered with nonionic surface-active chemicals, which are then instantly transformed into niosomal dispersion by hydrating with hot water while gently stirring before usage. These adaptable vesicular carriers serve as carriers or permeation promoters through the stratum corneum, and they demonstrate a more prospective promising technique for transdermal medication delivery. These are preferable and more thoroughly studied than other vesicles because they exhibit superior chemical and physical stability, are biodegradable and biocompatible, nontoxic, have the ability to permeate the skin, prolong the release of the drug, increase bioavailability, and reduce adverse effects and high reflux. The majority of research pioneers concurred that direct contact between these vesicles and the skin is necessary for efficient drug administration. 92 There are certain other pertinent researches that were carried out and governed by optimistic results, as shown in Table 3.
Transfersomes
Transfersomes are elastic nanovesicles mostly composed of phospholipids and edge activators (EAs) such as sodium deoxycholate, Span 60, Span 65, Span 80, sodium cholate (NaCo), dipotassium glycyrrhizinate, Tween 20, Tween 60, and Tween 80.67 It is the first generation of UDV, and it was first developed in 1992 by Cevc 93 (transfersomes, a trademark of IDEA AG, Munich, Germany). These elastic vesicles penetrate and permeate the skin as a result of a synergistic interaction between their carrier qualities and permeation-enhancing capacity. Based on their constitution, transfersomes can either keep their original structure or combine with skin lipids to pass through the skin layers. Because of the EA action as a result of mechanical stress, they can readily change their form and pass through the skin barrier by moving from the inside of the vesicle to zones with lesser curvature, which reduces the membrane’s elastic potential energy to a negligible level. In accordance with this method, transfersomes can pass through channels that are only one-tenth the size of vesicles 94 and traverse the Stratum corneum (SC) under the influence of a transdermal osmotic gradient. These elastic vesicles can only move across epidermal layers in nonocclusive conditions, allowing the additional water in the formulations to evaporate and maintain this hydration gradient. As a result, they do not diffuse, hence the penetration rate is independent of the concentration difference. Transfersomes are also capable of preventing the drug from being rapidly cleared from skin blood vessels and, if necessary, promoting the drug’s retention in the layers of skin. Transfersomes have been investigated as drug delivery systems for cutaneous or transdermal application of several medicines. However, one major drawback of these vesicles is that hydrophobic medicines are difficult to load into them without affecting their strength and ductility. 94 In terms of enhancing the permeation of drugs and interactions with the human skin, transfersomes have generally been shown to be superior to traditional liquid-state and gel-state vesicles and also conventional liposomes.93 Table 3 represents certain other researches that need to be brought forward.
Bilosomes
Bilosomes, a new type of vesicular carrier first identified by Conacher et al., is made up of bile salts integrated into the membrane of niosomes. 95 Bile salts are naturally occurring surfactants that are frequently used as absorption boosters to improve medication transport through biological membranes. 96 They do this by making hydrophobic medicines more soluble and by making the basolateral and apical membranes more fluid. 97 While nanosized vesicles of bilosomes and the inclusion of surface-active agents and bile salts in the formulation imply excellent prospects for using them transdermally, drugs such as tenoxicam and diacerein were successfully delivered by cutaneous and transdermal routes. 98
Many studies have demonstrated the potential of using bilosomes to successfully deliver vaccinations orally. 99 The presence of bile salts in bilosomes’ lipid bilayers increases their resistance to gastrointestinal bile salts and enzymes, providing protection for the entrapped vaccine from the conditions of the gastrointestinal tract. 100 For the best transdermal distribution, bilosomes’ nanosized particle size is necessary. The generated vesicular system is more stable when negatively charged bile salts (such as sodium deoxycholate) are used. In addition, it fluidizes, which would improve transdermal administration. A lipophilic terpene called limonene has been reported to interact with the lipids in the stratum corneum to increase skin permeability. The use of a bilosomal method for transdermal delivery demonstrated an increased permeability through SC. In addition, its safety has been proved by histopathological methods.98 Table 3 puts forth a few additional commendable researches and their remarkable outcomes.
Nanoemulsion
A fine dispersion of drugs in nanodroplets makes up a nanoemulsion, which is an isotropic, translucent, or transparent heterogeneous combination of two immiscible liquids. An interfacial film of emulsifying agents and coemulsifiers stabilizes it. They have small droplet sizes (20–400 nm), uniform size distribution, and are kinetically and thermodynamically stable systems (with no apparent coalescence and flocculation during long-term storage), 101 and have different biological and physicochemical characteristics than other emulsions (>500 nm). 102 The two immiscible layers are generally oil and aqueous, which are supplemented with substances that are soluble in either oil or water, respectively. Mixing the aqueous and oil phases with the addition of an emulsifier results in a coarse emulsion that can naturally transform into a nanoemulsion or be made nano by providing high energy. 103 There are three types of nanoemulsions that can be categorized based on their components, that is, oil in water (O/W), where the oil phase is dispersed in an aqueous phase, 104 water in oil (W/O), where the water phase is dispersed in oil phase, 105 and bicontinuous/multiple emulsion, where the microdomains of aqueous and oil phases are interdispersed inside the system. 106
In the creation of nanoemulsions, the oil phase is essential since it solubilizes the lipophilic medications intended to treat a variety of illnesses. The amount of oil in an O/W-type nanoemulsion can range from 2% to 20% W/W, depending on the administration site. According to Choudhury et al. (2013), drugs from BCS classes II and IV are the best candidates for the creation of an O/W nanoemulsion because doing so improves the solubility of such medications. Among a pool of emulsifier systems, the best ones are chosen based on their solubility, emulsification capacity, Hydrophile Lipophile balance value, and lower toxicity profile. 107 Since they are less hazardous and irritating than their anionic and specifically their cationic forms, nonionic surfactants are frequently utilized. 108 The O/W interface’s fluidity is further reduced as a result of the diffusion of the coemulsifier into the emulsifier’s interfacial coating, increasing the entropy of such overall colloidal dispersion. The interface is further stabilized, improving the hydrocarbon chains’ mobility. The strength of coemulsifiers is assessed using the area of the stabilized nanoemulsion zone under the phase diagram. 109 Other promising researches have been mentioned in Table 3.
Microemulsion
A microemulsion is a dispersion made up of an aqueous phase, an oil, a surfactant, and a cosurfactant. Microemulsions are a thermodynamically stable, optically isotropic liquid solution. Although there are many different ways to administer medications to patients in theory, the dermal use of microemulsion has drawn more attention. 110
The ability to create preparations of a W/O or O/W kind, the relationship between the quantities of the surfactant and cosurfactant, and the harmony of the lipophilic/hydrophilic phases are some similarities between the emulsions and microemulsions. 102 There are many benefits to using microemulsion for cutaneous and transdermal medication delivery. Three primary theories have been put out to explain why microemulsions are better for cutaneous medication delivery than other methods. First, the significant solubility potential of microemulsion systems for both hydrophilic and lipophilic medicines may improve thermodynamic behavior toward the skin. Second, microemulsion compounds that function as permeation enhancers may damage the stratum corneum and improve the flux of medications through the skin. Third, because it is simple to alter a drug’s affinity for the internal phase to favor partitioning into the SC, the drug’s permeation rate could be increased. 111 There are certain other pertinent researches that were carried out and governed by optimistic results, as shown in Table 3.
Silver nanoparticles
Silver nanoparticles (AgNPs) are NPs of silver ranging between 1 and 100 nm in size. The main mechanism of intriguing features of AgNP antimicrobial actions is based on adhesion to microbial cells, penetration inside the cells, reactive oxygen species, and free radical generation, and modulation of microbial signal transduction pathways. Due to this, AgNPs had a significant effect on the biomedical sector. 112 The antibacterial properties of silver compounds have long been understood, but since the development of antimicrobials, silver preparations have relegated themselves to a minor role. However the emergence of resistant strains has brought renewed focus to their potency for clinical use. Wide-spectrum antibacterials, AgNPs, are effective against both gram-positive and gram-negative bacteria, including antimicrobial-resistant strains and bacterial populations seen in biofilms. NPs cannot access the cytoplasm of gram-positive bacteria because of their thick peptidoglycan coating, hence the impact is greater against gram-negative bacteria. Yuan et al.’s evaluation of the MIC of glutathione-coated AgNPs (GSH-AgNPs) on E. coli and S. aureus serves as evidence for this claim. They found a significant difference between the two different bacteria, that is, 180 and 15 g/mL for S. aureus and E. coli, respectively. The NP MIC is one order of magnitude more than the Ag+ MIC for S. aureus, while the MIC values of colloidal and ionic Ag for E. coli were similarly quite comparable. 113 These data suggested different bacterial–NP interactions depending on the different bacterial topologies. It was verified by Transmission Electron Microscopy (TEM) examination of bacterial cultures exposed to completely ionized GSH-AgNPs. Because gram-negative bacteria have a thin bacterial envelope, which makes it simpler for NPs to enter the cytoplasm and find their targets than gram-positive bacteria do, the authors concluded from the images that the effects of GSH-AgNPs are stronger against E. coli than they are against S. aureus. 113
The production of Ag+, oxidative stress, as well as nonoxidative mechanisms is just a few of the processes that contribute to AgNP-antimicrobial activities. AgNPs can change the phospholipid bilayer and hinder transport through cells because of their ability to accumulate in the cellular envelopes and cling to bacterial cell surfaces through electrostatic attraction and interactions with the thiol group of cell membrane proteins. The form of the membrane is hampered by the development of numerous “depressions” and gaps that lead to cytoplasmic leakage and are more likely to result in cell death, and the bacterial cell wall becomes much more spherical and porous. 114 Ag+ NPs also cause an increase in reactive oxygen species levels within the cell, which causes hyperoxidation of proteins and DNA as well as direct lipoperoxidation-mediated rupture of the cell membrane. 115
AgNPs have undergone substantial research and are currently used in the pharmaceutical industry. When used with other antimicrobial medicines, AgNPs have produced synergistic effects. The MDR bacteria may be destroyed by the stronger NP conjugates. After being conjugated to AgNPs, Andersonin-Y1’s effectiveness against K. pneumoniae was increased. In contrast to the AMPs, with an MIC of 50 µM, the AMP-conjugated AgNPs’ MIC ranged from 5 to 15 µM. Nanocarriers are thought to be potential antimicrobial alternatives based on additional insights into their antibacterial mechanism provided by molecular dynamic simulation and nuclear magnetic resonance spectroscopy and which suggested killing by membrane pore creation through the hydrophobic collapse process. 116 To produce synergistic antimicrobial effects, AgNPs have been designed and synthesized with several compounds that show antibacterial activity. 117 Further testing of these findings was done on E coli. Scanning electron microscopy, transmission electron microscopy, and the lactate dehydrogenase (LDH) assay were used to analyze morphological alterations, cellular uptake, and the mechanisms of antimicrobial activity. The treated cells differed in size and form from the control cells, and there were cell lysis and membrane damage, suggesting that the NPs induced the cells to burst. Also, both bacterial strains’ lower cellular activity as seen by the LDH experiment points to an inhibited electron transport chain. This outcome was consistent with the previously suggested mechanism for NPs’ antibacterial action. 118
A study was conducted with E. coli and S. aureus, and the bacteria were subjected to sublethal dosages of AgNPs (already reported in the same study) for five days. The results showed that the bacteria’s tolerance to AgNPs increased, with half-maximal inhibitory concentration values increasing from 11.89 to 17.59 mg/L in the case of E. coli and 6.98 to 18.09 mg/L in the case of S. aureus. The findings indicate that bacteria evolved tolerance to a sublethal dose of AgNPs after successive selections of the cells that survived.
A similar result was reported in the study carried out by Panacek et al., in which E. coli and P. aeruginosa were subjected to AgNPs and then cultivated to see if the bacteria developed resistance to the NPs. The results showed that both bacteria developed resistance to the NPs, as evidenced by an increase in their MIC from 3.38 to 13.5 mg/L in E. coli after numerous rounds of culture, and a similar effect was found in P. aeruginosa. 119
Gold nanoparticles
Similar to AgNPs, gold nanoparticles (AuNPs) can come in a variety of sizes and forms, including nanorods, nanospheres, nanoprisms, and nanocages. These characteristics affect their color. As a result, metallic gold is golden in color, whereas colloidal gold has a variety of colors due to absorbance mechanisms that depend on certain Localized Surface Plasmon Resonances bands and scattering, such as ruby red for nanospheres and black or blue for nanorods. 120
AuNPs can be used in a variety of biological applications, including biosensors, genomics, the photothermal destruction of cancer cells, and the treatment of microbial infections. They have a 360-degree activity because they are good nanocarrier systems for antimicrobials and nanobactericides, as well as an evolving platform for the detection of bacteria. 50 Actually, there are divergent views on the antibacterial properties of AuNPs. The majority of experts are certain that AuNPs do not have inherent antibacterial activity on their own. They cannot be regarded as nanobactericides. Others have discovered mild antibacterial activities only at high concentrations, most likely as a result of the agent being a chemical synthesis by-product. 121 Zhan et al. discovered that AuNPs exhibit potent bactericidal effects against an E. coli strain that is multidrug resistant. 122
AuNPs feature a bactericidal mechanism independent of reactive oxygen species, making them different from most metallic NPs and presumably ensuring that they are less harmful to mammalian cells. Although there have been ups and downs in the utilization of gold as a bioactive compound over the years, both in bulk form and at the nanoscale level, and their application as antibacterial agents still seems to be debatable, AuNPs are widely regarded as the best possible nanocarriers for a variety of molecules, including vaccines, conventional antimicrobials, and AMPs. There are several in vitro examples of improving antimicrobial efficacy and preventing resistance mechanisms in the literature, particularly in the latter scenario. 123
In fact, the majority of MNPs, including AuNPs, can serve as both antimicrobial agents and drug transporters. Although AuNPs have been shown to have bactericidal effects on multidrug-resistant gram-negative bacteria, carriers are the preferred use for AuNPs. 118 The shape, size, and surface makeup of AuNPs are thought to be responsible for their therapeutic benefits. While the surface composition can be changed by adding biomolecules through electrostatic contact and covalent conjugation, the size and shape can be changed during synthesis by adjusting the proportions among metal precursors and reducing agents. For the objective of target specificity, targeting moieties such as antibodies are attached. 124 Ultrasensitive 17-estradiol detection was made possible by immobilizing anti-17-estradiol on AuNPs. 125 Table 3 represents certain other researches that need to be brought forward.
Metal Oxide NPs
Zinc oxide NPs
Zinc oxide (ZnO) is a harmless compound, according to both the European Food Safety Agency and the U.S. Food and Drug Administration (US FDA). As a result, it is utilized in the food industry (both as a food ingredient and as a substance for food packaging to maintain color and maintain microbiological safety) 126,127 and in the cosmetics industry (for its deodorant, antibacterial properties and as a sunscreen such as TiO2). Due to their optical, physiological, and antibacterial qualities, ZnONPs have become popular among metal oxide NPs. ZnONPs are undoubtedly very intriguing nanomaterials for a variety of industrial uses, including optical communications and the production of cement, rubber, coating, paint, and lubricants to name a few, 128 as well as for biological uses, particularly in the antibacterial and anticancer. 129 The release of Zn2+ ions is the mechanisms of ZnO antibacterial actions. Zn2+ ions adhere to the surface of the bacterial cell wall and change the permeability of bacterial cell membrane. It also affects the amino acid metabolism.
It is reasonable to assume that nanosize-ZnO, with its high surface-to-volume ratio, is a superior antibacterial than its bulk counterpart assuming ZnO possesses good antibacterial capabilities. In fact, ZnONPs have excellent stability, a decent toxicological profile, and are inexpensive. They are also efficient against a variety of resistant and sensitive human infections. Studies have specifically shown that ZnONPs are biocompatible with cell lines from humans while having notable selective toxicity toward a variety of gram-negative and gram-positive bacteria. ZnONPs alone can be regarded as nanobactericides due to their inherent antibacterial activity, but because their additive action with specific types of antimicrobials has been shown, they can also be used as drug carriers to boost traditional antimicrobial activity and combat resistance mechanisms. 130
The size of the particles and concentration, surface properties, shape, and Ultra Violet (UV) light exposure are some of the factors that favorably affect ZnONPs’ antibacterial activity. 130 The smaller the particle size, the bigger the surface area accessible to bacteria and the simpler it is to penetrate the bacterial membrane. Moreover, the production of H2O2 and the dissolution of Zn2+ ions are events that depend on the surface area. 131 Finally, ZnONPs’ antibacterial effectiveness is improved by their reduced size. In this regard, Sirelkhatim et al. discovered that the survival of the bacterial cell drastically decreased with a drop in the particle size from 212 to 12 nm by investigating the antibacterial capabilities of ZnONPs against both gram-negative and gram-positive bacteria. Whereas ZnONPs <12 nm exhibited bactericidal action, ZnONPs >100 nm demonstrated bacteriostatic effect against MRSA. ZnO surfaces can be modified by thermal annealing, which results in a greater amount of O2 being absorbed onto the surface and a corresponding increase in the generation of reactive oxygen species, or by applying coating agents that cause a greater release of Zn2+ or improve reactive oxygen species genesis. 130 The form of ZnONPs affects cytotoxicity, the number of active surfaces (high density is associated with a strong antibacterial effect), and the internalization mechanism. Spherical ZnONPs have a harder time penetrating than wires and rods. According to Talebian et al., spherical and rod-shaped ZnONPs are less effective against E. coli and S. aureus than flower-shaped ZnONPs. 132
In addition, ZnO NPs/MPs have been combined with other antimicrobial medicines, metal oxide NPs/MPs, and devices to improve antibacterial action against pathogenic microbes. They exhibit synergistic or enhanced antibacterial properties against S. aureus, B. subtilis, E. coli, P. aeruginosa, Aeromonas veronii, and K. pneumoniae. ZnO NP/MP combinations with other materials are used as dosage forms other than particles, such as membranes, films, and plates, depending on the administration route or usage, to improve antibacterial effectiveness. These dosage forms can transport the medicine to the exact location of infection in human diseases such as cystic fibrosis, endocarditis, otitis, and pneumonia. 133
Titanium dioxide NPs
Titanium dioxide NPs (TiO2NPs) are highly valuable in a variety of industrial applications due to their excellent qualities, including chemical and biological nontoxicity, chemical and physical stability, resistance to corrosion, water solubility, and low production costs. The two main uses are for pigments and paints. For instance, TiO2 is perhaps the most popular white pigment and opacifier used in food, medicine, cosmetics, and the paint industry. Glass, electric conductors, and catalysts are some further applications, followed by paper and plastics. 134 Subsequently, a number of works accompanied, in which nano-TiO2 was used in the disinfection of substrate surface, wastewater, and water. 135 In essence, similar to ZnO, TiO2 is a metal-oxide-semiconductor photocatalyst whose antimicrobial activity is primarily dependent on the production of reactive oxygen species by photocatalysis. It causes breakdown of bacterial outer cell membranes through reactive oxygen species production, which leads to cell death. TiO2NPs have the same photocatalytic properties as the bulk of TiO2 combined with the well-established and advantageous attributes of NPs. 136 TiO2NPs show broad-spectrum antibacterial action, are environmentally safe, and are effective against both gram-positive and gram-negative bacteria and fungi. 137 As evidenced by the data published in the literature, TiO2NPs are effective and useful not only for the processes of disinfecting and sanitizing water and surfaces but also for nano-antimicrobials and delivery systems of traditional antimicrobials. To prevent contamination, Pascagaza et al. recommended coating the surfaces with TiO2 in all locations that require routine disinfection, such as clinical and laboratory settings. TiO2 creates OH-radicals that are extremely reactive and capable of killing bacteria when exposed to Ultra Violet-A (UV-A) rays, water, and oxygen. It has been shown that this disinfection method is efficient based on the elimination of germs such as E. coli, S. aureus, E. faecalis, P. aeruginosa, and the fungus Candida albicans. The researchers discovered that TiO2NPs are most effective against E. coli, P. aeruginosa, S. aureus, E. faecalis, and C. albicans. 138 The antimicrobial activity of TiO2 is intimately related to NP attributes such as size, shape, and crystal nature, and also more so because TiO2 photocatalytic effectiveness depends on them, as has already been observed for other nanostructures. 139 With a band gap energy of 3.2 eV, anatase crystalline TiO2 can produce electron-hole pairs when exposed to UV-A light or shorter wavelength radiation. Since they interact with water and oxygen to form reactive oxygen species, mostly the superoxide radical and hydroxyl radical and also singlet oxygen and hydrogen peroxide, the photogenerated electrons and holes are responsible for the TiO2 photocatalytic antimicrobial action. 140 The oxidative phenomena impacting diverse bacterial cellular components are caused by a large generation of reactive oxygen species that is not balanced by their removal. Lipids are peroxidized, the porins and outer membrane proteins are affected, and the polysaccharide chains get broken down at the level of the cell wall. All of this makes it simpler to access the cell membrane. In addition to oxidizing membrane phospholipids, reactive oxygen species also cause cell lysis, enhance fluidity, the degradation of cellular components, relatively rapid release of K+ followed by a gradual liberation of RNA and proteins, and lastly, it is likely that microorganisms will mineralize. The loss of cytoplasmic material was also noted in microscopy experiments on P. aeruginosa treated with TiO2NPs: “bubble-like protuberances that discharged cellular components.” 141 Of course, the respiratory chain is inhibited as a result of membrane disruption. Table 3 puts forth a few additional commendable researches and their remarkable outcomes.
CONCERNS WITH DERMAL ANTIMICROBIAL AGENTS’ SAFETY
Dermal antimicrobials are a crucial tool for treating SSTIs as well as for preventing cutaneous and superficial infections. The spread of fungi and bacteria at the infection site can be considerably inhibited by dermal antimicrobial medications. Antimicrobials delivered dermally have various benefits over those administered systemically, including a reduction in bacterial resistance and the ability to give larger antimicrobial dosages at the infection site. 52 However, due to repeated usage and a compromised skin barrier, dermal antimicrobial medicines can have local adverse effects such as allergic contact dermatitis. 142 It is believed that allergic contact dermatitis results from a delayed type of cutaneous hypersensitivity in those who have already been sensitized. The majority of the sensitized T cells are T helper 1 type. Innate immunity is activated during the sensitization phase with the help of cytokines produced by keratinocytes. To activate T lymphocytes that are specific for the allergen, the allergen is taken up by cutaneous dendritic cells and Langerhans cells before traveling to the lymph nodes. After multiplying, these T cells enter the bloodstream and go toward the exposure site. When exposed to the allergen once more, antigen-specific T cells get activated by the release of cytokines and produce inflammation. 143
CHALLENGES IN ANTIMICROBIAL PREPARATIONS FOR DERMAL DISEASES
Due to the global spread of different fungal and bacterial strains, numerous dermal medication formulations have been created and are now accessible for purchase. Since the emergence of drug-resistant microorganisms makes it challenging to provide effective dermal therapy for SSTIs, the pharmaceutical industry and academic laboratories have dedicated a lot of time, effort, and resources to the research and development of new dermal antimicrobial formulations. In addition to having a strong antimicrobial action against a variety of pathogens, the ideal dermal antimicrobial medication should also be nonirritating and safe to use. The precise formulation, the amount of the therapeutic agent, and the length of exposure all affect a drug’s potential for toxicity. Dermal antimicrobials should be carefully formulated with the possibility of negative side effects in mind. It is important to conduct both in vitro and in vivo investigations to examine the effects of both short- and long-term skin exposures toward the newly found dermal antimicrobial medications, administrated at various doses. To definitively establish drug safety during dermal administration, clinical studies should also be carried out to investigate the safety and possible toxic effects of topically applied antimicrobial formulations in human subjects. Figure 3 represents the general mechanism of action of different nanocarriers of antimicrobial agents.
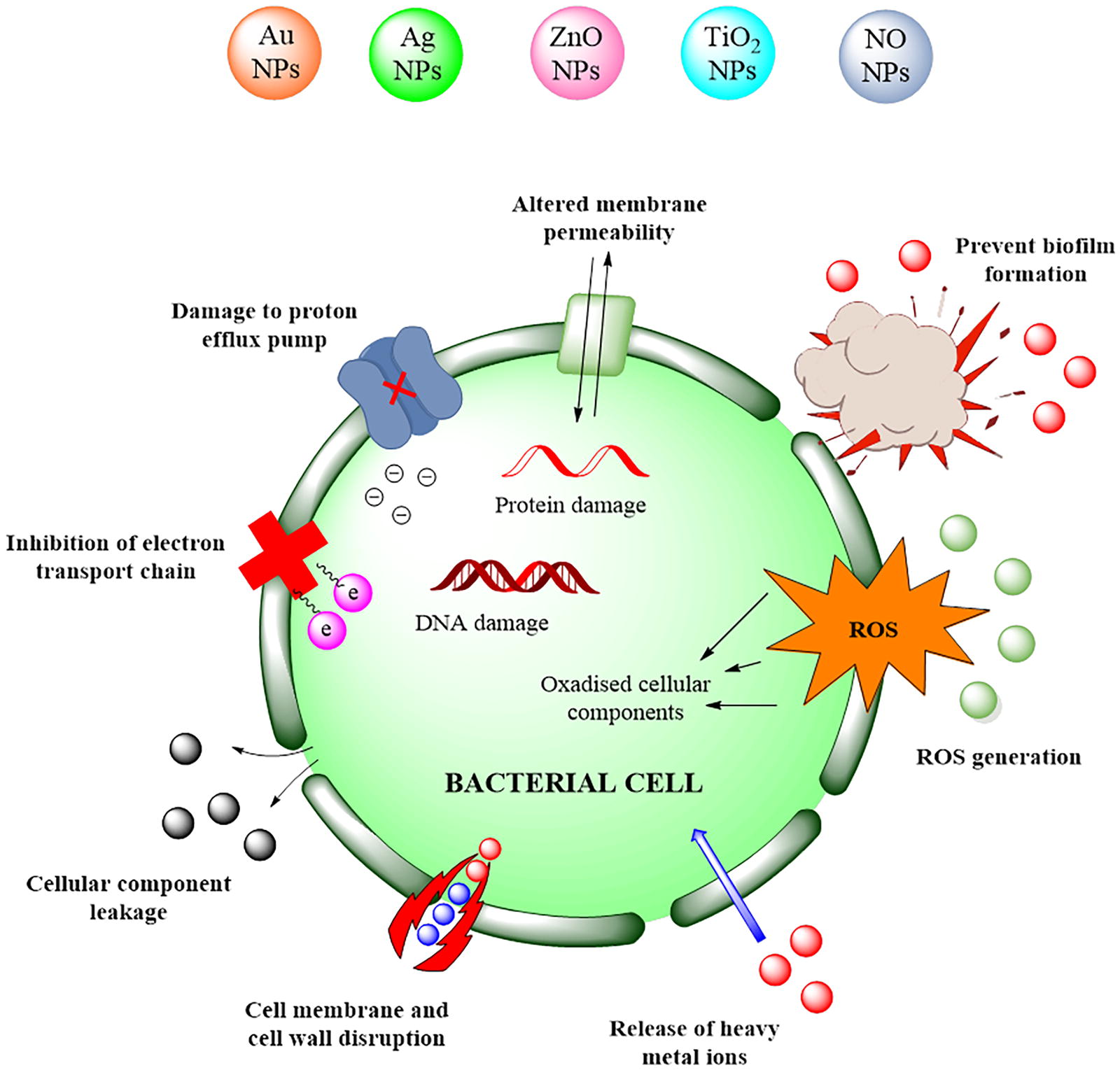
Depicting the general mechanisms of action of various nanocarriers for antimicrobial agents. This illustration highlights how different nanocarriers improve cellular uptake, enhance drug delivery, and facilitate the disruption of efflux pumps, ultimately increasing the efficacy of antimicrobial therapies. 144,145
NANOCARRIERS IN CLINICAL TRIALS
The creation of nanomedicines that are presently available was facilitated by the investigation of several functional nanomaterials in preclinical and clinical investigations, most notably several clinically authorized liposome drug preparations and metallic diagnostic agents. 144 The majority of nanocarriers used in clinical trials and preclinical studies target cancer. 145 The most popular types of carriers are lipid and polymeric nanocarriers. LiPlaCis, a lipid-based nanoformulation with cisplatin presently in phase II for the management of resistant solid tumors, and NK105 coupled with paclitaxel are two examples of such carriers under clinical studies. 146 However, in recent years, the use of nanotechnology-based therapies for illnesses besides cancer has grown tremendously. Another crucial clinical area being researched for the development of nanomedicine is antimicrobial therapy. MNPs have the ability to act as both carriers and antibacterial agents. AgNPs, in particular, can pass through the bacterial cell membrane, causing Ag+ release and toxicity. For decades, this NP has been the subject of intensive research and usage in medicine. AgNPs with antibacterial characteristics were used to treat wounds, and the FDA approved this use. 147 There are now nine clinical trials looking at AgNPs as an antibacterial treatment for various disorders.
A rising body of research indicates that AMPs are rapidly garnering greater interest for their potential therapeutic applications since they show exceptional advantages over traditional antimicrobials. AMPs have been recognized as exceptional potential antimicrobial agents to conquer AMR. AMPs perform important roles in the inherent immune system and are specifically involved in all life-forms. Certain AMPs have been preserved throughout evolution, which may be a sign that these compounds have the potential to limit the tendency for the emergence of microbial resistance. Just a few AMP-based preparations have progressed into clinical studies despite the medicinal advantages of AMPs. 148 AMPs are categorized in clinical trials. It is possible to increase AMPs’ transport, biological activity, stability, and toxicity by making specific alterations to them. The latest developments in drug delivery using nanotechnology have been thoroughly studied. As nanotechnology has been successfully used to create better medication delivery systems, its usage for the distribution of AMPs is also feasible and may result in the creation of brand new antimicrobial drugs that can combat MDR. More research into MNPs’ basic biological effects, biodistribution, and pharmacokinetics is essential for therapeutic applications, particularly with regard to silver as well as other nano-based nanocarriers. 149
CONCLUSION AND FUTURE PROSPECTS
Microbes evolve exponentially faster than the development and utilization of antimicrobials, which poses a problem. However, as a result of antimicrobial overuse and even improper usage of various other antimicrobials, these drugs eventually lost their antimicrobial efficacy and drug-resistant bacteria started to emerge. Although AMPs have been considered a replacement for antimicrobials, there are still unidentified antimicrobials in AMPs, and the reduced pharmacokinetics of peptide medicines makes it difficult to use existing AMPs effectively. Their entry into clinical studies and eventual implementation may be facilitated through the utilization of AMP delivery devices. Antimicrobials work by specifically targeting certain cellular elements or metabolic intermediates, which inhibit or kill bacteria. Inhibiting essential enzymes that are involved in microbial growth and metabolism is the most frequent approach. This might cause genetic changes that make bacteria resistant to antimicrobials. In contrast, AMPs conjugate to the negatively charged bacteria’s bilayer membrane, thanks to their amphipathic characteristics, allowing for quick penetration. Mutations have no effect on this process. Furthermore, AMPs work throughout the whole cellular membrane to combat bacteria, making it difficult for them to acquire resistance. AMPs with immune regulatory capabilities broaden the scope of their mechanism of action. Antimicrobials go through detoxification, and full renal clearance is not always guaranteed. Nevertheless, monomeric amino acids, which can be directed to crucial biosynthetic pathways, are involved in the metabolic breakdown of AMPs. Novel treatments are desperately needed because present antimicrobials and antimicrobial medicines are constantly developing resistance. Because of the method through which they physically damage the viruses’ phospholipid bilayer and kill them, AMPs have become available alternatives. The danger of drug resistance to such peptides is constrained by the metabolic necessity of membrane repair. However, the adoption of AMPs has been constrained by their correlation with other factors such as instability and proteolytic breakdown. To address MDR issues, drug delivery systems are recommended as the best method for drug uptake, release (sustained, regulated, and triggered), and protease prevention. Drug delivery methods made of nanomaterials are increasingly used to increase therapeutic activity and lessen negative side effects. It is important to determine the method by which NPs’ conjugation, functionalization, entrapment, and complex can affect bacterial populations given their extensive therapeutic participation. The therapeutic indices of several nanocarriers, including MNPs, polymeric, and liposomes, all have been found to be good. Table 3 describes the effects of dermal delivery of nanocarriers of antimicrobial agents on an animal model.
NPs can target infection locations, which is a distinct advantage. To effectively combat pathogens and MDR infections, it is crucial that nanocarriers and AMPs work in concert to penetrate cell walls, aggregate particles, produce reactive oxygen species, and suppress cellular activity. Although identifying the right carrier, entrapment effectiveness, and conjugation chemistry are hurdles for AMP-carrier systems, there are various active research investigations for AMP-nanocarrier optimization. Basic research with in vitro endpoints had geometrically more AMP conjugated with the nanocarriers when compared with clinical trials. Further in vivo research is needed to comprehend the immunological and physiological barriers to reduce the difficulties in clinical trials as AMP discovery continues to grow. When it comes to combating MDR infections, AMP nanocarriers are indeed a worthwhile investment because nanotechnology has the potential to revolutionize the medical industry.
Footnotes
ACKNOWLEDGMENTS
The authors are thankful to Metro College of Health Sciences & Research, Greater Noida, and the Department of Pharmaceutical Technology, Meerut Institute of Engineering & Technology for providing necessary facilities.
AUTHORS’ CONTRIBUTIONS
Conception and design: All authors. Material preparation, data collection, and analysis: P., P.K.G., and S.K. First draft of the article: P. All the authors commented on the previous versions of the article. All authors read and approved the final article.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The study did not involve any human subjects, and therefore, no ethical approval was required.
CONSENT FOR PUBLICATION
The study did not involve any human subjects, and therefore, no consent was required.
AVAILABILITY OF DATA AND MATERIALS
The data requested will be provided by the corresponding author upon reference to the article.
CONFLICT OF INTEREST
The authors state that they do not have any conflicts of interest.
DISCLOSURE STATEMENT
The authors have no relevant financial or nonfinancial interests to disclose.
FUNDING INFORMATION
The authors declare that no funds, grants, or other support was received during the preparation of this article.