
Abstract
HIV dynamics in seminal plasma during primary HIV infection was evaluated through an observational study of individuals with primary HIV infection at the University of Washington Primary Infection Clinic. Seminal plasma HIV RNA was quantified using a real-time reverse transcription PCR assay. Blood plasma RNA was quantified by bDNA or PCR-based assays. Longitudinal analyses of HIV RNA levels over time used random effects regression analysis. From 1993 to 2005, 110 men collected 327 semen specimens. Initial blood and seminal plasma RNA levels in untreated men were only moderately correlated (Spearman r = 0.38, p = 0.0002). Estimated peak and set point levels were lower in semen than blood by 0.8 (p = 0.001) and 0.7 (p < 0.001) log10 copies/ml, respectively. RNA decay rates were similar in the two compartments (p = 0.4). For 2 months after infection, mean HIV RNA levels in seminal plasma remained above a threshold level (3.8 log10 copies/ml) that has been associated with recovery of infectious virus in vitro. HIV-positive men are likely to be most infectious in the first months following HIV acquisition. However, the modest relationship between HIV RNA levels in blood and seminal plasma suggests that the relative risk of HIV transmission during primary infection may vary from current estimates that are solely based on blood levels. Incorporating seminal plasma HIV levels into future mathematical models may increase the accuracy of these models.
Introduction
T
The limited available data that describe seminal plasma HIV RNA levels during primary HIV infection are similar to data from men with established infection. 13 –18 In the United States, blood and seminal plasma HIV RNA levels during primary HIV infection are moderately correlated at best, 9,10,19,20 and mean HIV RNA levels have been reported to be 1.3–1.5 log10 copies/ml lower in semen than in blood. 9,10 Similar findings were recently demonstrated in a study of 16 men with primary HIV infection (subtype C) who presented to a sexually transmitted disease clinic in Malawi. 21
A full understanding of how changes in HIV RNA levels (i.e., viral dynamics) following HIV acquisition impact HIV transmission remains elusive. We sought to address this issue by modeling longitudinal HIV RNA levels in blood and semen collected from men with primary HIV infection.
Materials and Methods
Patient population
From 1993 to 2005 individuals with primary HIV infection were enrolled into an observational cohort at the University of Washington Primary Infection Clinic. 22 –25 This analysis expands on a description of HIV RNA levels in 72 semen samples from 34 men enrolled before 1997. 19 Although eligibility criteria for study participation have varied slightly over time, at the time of entry into the cohort all subjects were either HIV antibody negative (acute HIV infection) or HIV antibody positive with a negative or indeterminate Western blot, negative “detuned” antibody test, or negative HIV test within 365 days prior to screening (early HIV infection). All subjects were enrolled within 240 days after HIV infection, estimated to be the date of onset of seroconversion symptoms 22 or, for asymptomatic subjects, the midpoint between the last negative and first positive HIV tests. Some subjects received antiretrovirals (ARVs) through nonrandomized research protocols or primary care. The University of Washington Institutional Review Board approved this study, and all subjects gave written consent for study participation.
HIV RNA quantification
Initially, blood plasma HIV RNA quantification used branched DNA (bDNA) assays with lower limits of detection (LLDs) of 10,000 or 500 copies/ml (Chiron Corporation, Emeryville, CA). In later years, specimens with results below LLDs were retested using an ultrasensitive reverse transcription polymerase chain reaction (RT-PCR) assay (Roche, Branchburg, NJ; LLD = 50 copies/ml) or an independently validated real-time RT-PCR amplification assay (LLD = 50 copies/ml). 26 After 2002, specimens were evaluated by one of the two RT-PCR assays. Intertest reliability among all of these assays is high, and the testing laboratory was certified to perform these assays by the National Institutes of Health Division of AIDS-sponsored Virology Quality Assurance Program. 27 –29
Semen was collected by masturbation and processed within 2 h. 13 Specimens were diluted to reduce viscosity and centrifuged to separate the seminal plasma and cell pellet. Boom (silica) extraction was performed to minimize the effect of inhibitory factors, and HIV RNA was quantified using the real-time RT-PCR assay (LLD = 300 copies/ml) or Roche Amplicor HIV-1 Monitor versions 1.0 or 1.5 (LLD = 200 copies/ml). 30 For both blood and semen, specimens with HIV RNA levels below LLDs were assigned censored values.
Statistical analysis
Statistical analyses were performed using Stata9 software (StataCorp LP, College Station, TX). To assess the correlation between initial HIV RNA levels in the two compartments, we compared the closest blood sample that was obtained within 45 days of the date of the first semen collection. Viral decay models used random effects regression analysis. Two models of blood and semen were fit to the longitudinal data: the first used data from the first 100 days following infection to estimate intercepts and slopes of viral decay and the second used data from day 100 to day 365 to estimate viral set points. The estimated intercept of the first model (day 0) represented the symptom onset date for most subjects, which approximated peak viremia. The estimated coefficient of the time covariate represented the slope of viral decay. In the second model, the set point was derived from the average of all HIV RNA values between day 100 and day 365 for all individuals, which accounted for the correlation within subjects due to repeated measurements. We conducted a sensitivity analysis to evaluate how these estimates might change when we varied the day that the set point was established to earlier or later than day 100.
Results
Between 1993 and 2005 110 male subjects collected a median of 2 (range 1–11) and a total of 327 semen specimens. At the first screening visit at the PIC, 9 (8%) subjects remained HIV antibody negative, 5 (5%) subjects were antibody positive with a negative or indeterminate Western blot, 10 (9%) subjects were eligible for study enrollment because they had a negative detuned antibody test, and the remaining 86 (78%) subjects had last tested HIV antibody negative a median of 146 (range 9–760) days prior to study screening. (Note that subjects who were referred for screening when they were antibody negative/RNA positive are included in this last category if they were antibody positive at the first PIC visit.) The median age of study subjects was 34 years [interquartile range (IQR) 29–38 years] at study enrollment. Most subjects (80%) experienced symptoms consistent with the acute retroviral syndrome, but only two men (2%) described symptoms or were diagnosed with a sexually transmitted infection at the time that semen specimens were collected. Subjects were screened for study enrollment a median of 59 days (IQR 27–98 days) from the estimated date of HIV infection, and the initial semen specimen was collected a median of 108 days (IQR 66–183 days) after infection; 118 semen specimens were collected within the first 180 days after HIV infection. The mean initial CD4+ T cell count was 580 cells/mm3 [standard deviation (SD) 198 cells/mm3] among all subjects.
Among the 89 subjects who were not treated with ARVs at the time of their first specimen collection, the mean initial seminal plasma HIV RNA level was 3.6 (SD 1.0) log10 copies/ml; levels were highest in nine men who collected their first semen specimens within 1 month of HIV infection (median 5.0 log10 copies/ml, IQR 3.8–5.3 log10 copies/ml) (Fig. 1). Two-thirds of untreated subjects who collected their initial semen specimen within 1 month after HIV infection had HIV RNA levels above the threshold level of 3.8 log10 copies/ml that is associated with persistent recovery of infectious HIV in mixed lymphocyte cultures. 13 This proportion declined in subsequent months. Seminal plasma HIV RNA levels were undetectable in all 21 subjects who were receiving ARVs at the time of the initial collection.
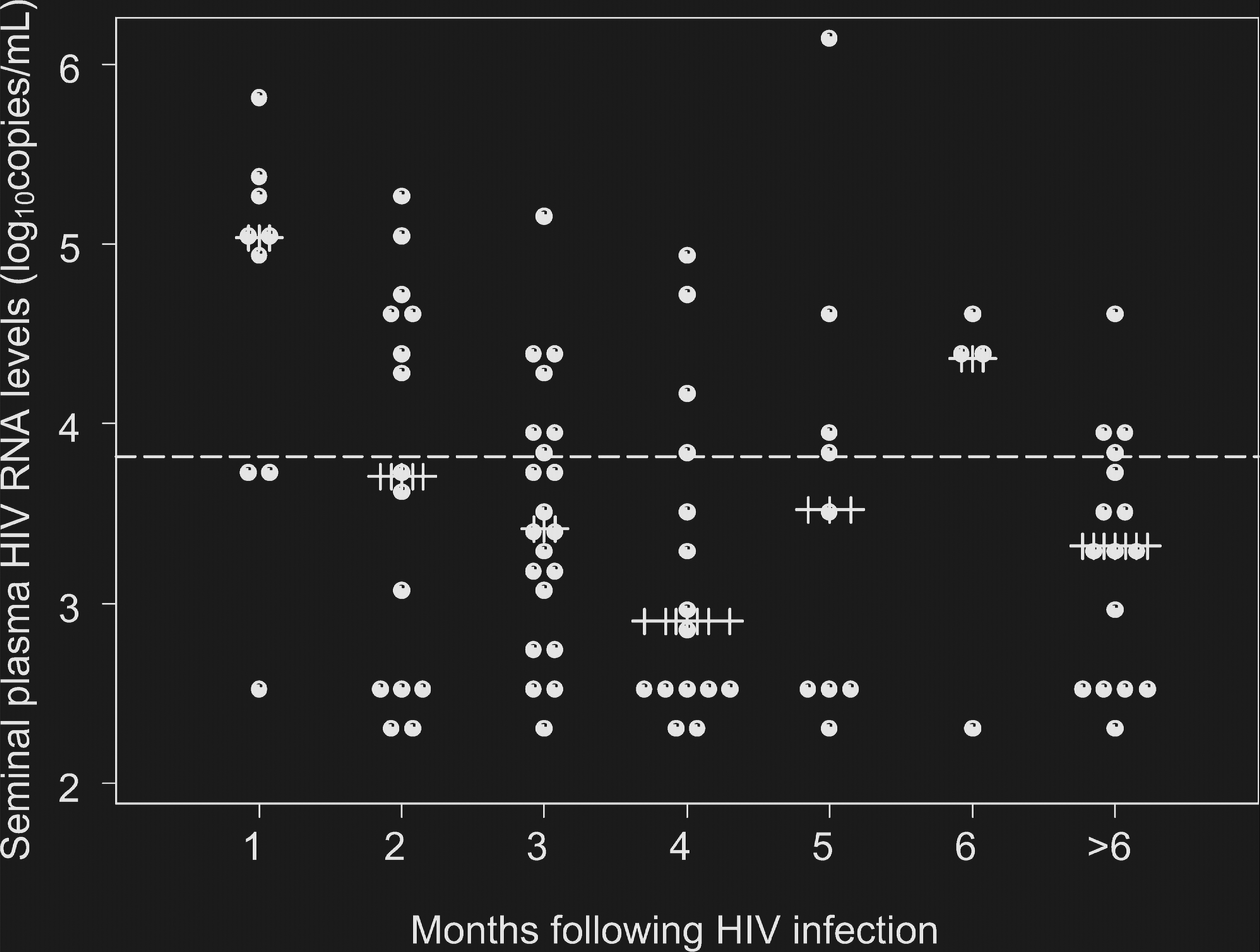
Circles (•) represent the initial HIV RNA level in seminal plasma among 89 subjects who were untreated at the time of the collection of their first semen specimens. Plus signs (+) represent median HIV RNA level by month since the estimated date of HIV infection. The dashed line represents the threshold at 3.8 log10 copies/ml associated with the ability to culture infectious virus. 14 The proportions of subjects whose initial specimens had seminal plasma HIV RNA levels above this threshold were for specimens collected within 1 month of HIV infection, 67%, 1–2 months after infection, 47%, 2–3 months after infection, 29%, 3–4 months after infection, 20%, 4–5 months after infection, 44%, 5–6 months after infection, 75%, and greater than 6 months after infection, 25%.
Among all subjects, the mean HIV RNA level in the first paired blood sample was higher than in the initial semen specimen (4.0 versus 3.3 log10 copies/ml, p = 0.0001 by paired t-test). The mean initial blood plasma HIV RNA level was 4.4 (SD 1.1) log10 copies/ml in the 89 untreated subjects, and the median blood plasma HIV RNA level was 1.8 (IQR 1.5–3.0) log10 copies/ml in the 21 subjects receiving ARVs. HIV RNA levels in initial semen and paired blood samples from untreated individuals were only moderately correlated (Spearman r = 0.38, p = 0.0002).
Data censoring occurred frequently at LLDs for assays quantifying HIV RNA levels in blood (27 specimens <50 copies/ml, 8 specimens <500 copies/ml, and 18 specimens <10,000 copies/ml) and seminal plasma (37 specimens <200 copies/ml and 97 specimens <300 copies/ml). Longitudinal regression analysis of all samples collected within a year of infection from untreated individuals estimated that the peak HIV RNA level was higher in blood than seminal plasma (5.3 versus 4.5 log10 copies/ml, p = 0.001) (Fig. 2), but rates of viral decay in blood and seminal plasma were similar (−0.34 and −0.44 log10 copies/ml per month, p = 0.4). Due to the relatively small sample size and infrequent sampling, attempts to estimate the exact day on which the HIV set point was established 31 were not successful. However, sensitivity analyses confirmed that the set point occurred no later than day 100 (data not shown). The viral set point was higher in blood than in seminal plasma (4.2 versus 3.5 log10 copies/ml, p < 0.001). The viral set point for seminal plasma derived from the longitudinal regression analysis was not different from a cross-sectional analysis of the mean HIV RNA level of seminal plasma specimens collected closest to 180 (±60) days after HIV infection (3.3 log10 copies/ml).
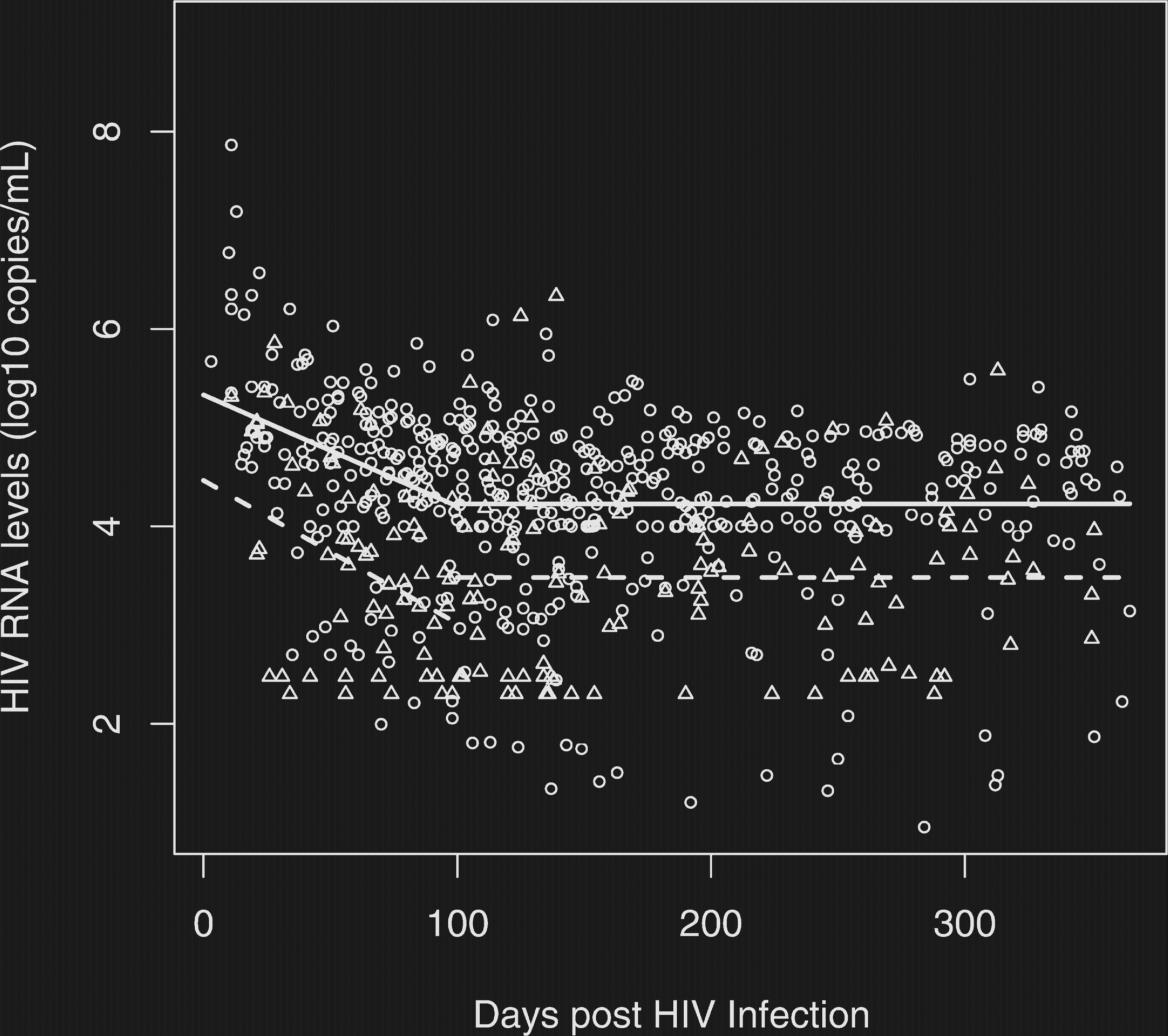
HIV RNA levels in blood and seminal plasma in untreated subjects over time. Circles represent HIV RNA levels in blood plasma from subjects who were not receiving antiretroviral therapy at the time of the specimen collection. Triangles represent HIV RNA levels in seminal plasma from untreated subjects. The solid line is the initial slope of viral decay in blood and the viral set point in blood after 100 days following HIV infection; the dashed line indicates the same in seminal plasma.
Data were insufficient to assess the impact of ARVs on the rate of viral decay during primary HIV infection because in the first 100 days after HIV infection only two subjects collected semen specimens both before and after the start of ARVs. In the year following infection, seminal plasma HIV RNA was detectable in 125 (78%) of 160 samples from 88 subjects not receiving ARVs. Of the 42 ARV-naïve subjects who collected at least two semen specimens, four (10%) had consistently undetectable levels, 22 (52%) had consistently detectable HIV RNA levels, and the remaining 16 (30%) had undetectable HIV RNA levels in a medium of 25% (IQR 20–50%) of the semen specimens. In contrast, seminal plasma HIV RNA was detectable in two (22%) of nine samples from four subjects on nucleoside reverse transcriptase inhibitors (NRTIs) alone, none of 11 samples from 11 subjects on non-nucleoside reverse transcriptase inhibitor (NNRTI)-based therapy, 2 (10%) of 20 samples from 15 subjects on protease inhibitor (PI)-based therapy, and none of four samples from four subjects who were receiving both an NNRTI and PI. However, compared to subjects receiving NNRTI-based therapy, these differences in the proportions of subjects with detectable HIV RNA were not statistically significant.
Discussion
Our study shows that HIV RNA levels peak in seminal plasma shortly after the acquisition of subtype B HIV and for approximately 2 months after HIV infection remain above a level that is associated with viral infectivity in mixed lymphocyte culture. 13 Like another study of men acutely infected with subtype C virus, 21 these data provide an explanation for the relatively increased risk of sexual HIV transmission from individuals with primary HIV infection 1 and further strengthen the rationale for the use of public health-based pooled HIV RNA testing programs to identify highly infectious individuals during acute HIV infection. 32 –35
Our data also highlight the compartmentalization of HIV between the blood and genital tract. 36 HIV RNA levels in blood and seminal plasma during primary HIV infection were only moderately correlated, consistent with other smaller studies. 9,10,20,37 –39 This only moderate correlation may explain why the variation in blood HIV RNA levels cannot fully explain the risk of sexual HIV transmission and supports the inclusion of genital tract HIV RNA levels 40 and other genital tract cofactors 41 in models of sexual HIV transmission. Furthermore, before blood HIV RNA levels alone are used to estimate whether non-genital tract coinfections such as malaria 42 and tuberculosis 43 increase the risk of sexual HIV transmission, empiric data should be collected as part of proof-of-concept studies to show that these coinfections increase genital tract HIV RNA levels.
Although the inclusion of genital tract HIV RNA levels in mathematical models that estimate the relative risk of HIV transmission may increase the accuracy of these models, use of our data could somewhat overestimate the population-level risk of HIV transmission during primary HIV infection. Seminal plasma HIV RNA levels in our cohort may not be perfectly representative of all individuals who acquire HIV infection because individuals who are diagnosed and referred for study enrollment during primary HIV infection are likely to have experienced symptoms consistent with the acute retroviral syndrome, and this has been associated with higher blood HIV RNA levels. 23 In our study, subjects with seroconversion symptoms also had higher seminal plasma HIV RNA levels compared to asymptomatic subjects, but this association was no longer significant after controlling for blood plasma HIV levels (data not shown) due to the moderate correlation between blood and seminal plasma HIV RNA levels. Despite this limitation, our data may be actually more representative of seminal HIV RNA levels during primary HIV infection compared to other previously published studies because of the extremely low rate of concurrent, clinically apparent STIs among our study participants.
We did not measure peak HIV RNA levels in semen or estimate the timing of peak levels because few subjects in our cohort collected semen specimens prior to peak viremia. Therefore, based on currently available data, any estimate of the timing of peak viremia in seminal plasma would be entirely based on theoretical modeling. Our models could overestimate peak levels in blood and seminal plasma if the onset of symptoms precedes peak viremia. However, any difference between the peak HIV RNA levels in blood and seminal plasma would remain constant unless the timing of peak levels varies in the two compartments.
Our data are also consistent with prior pharmacologic studies in established HIV infection. Despite intraclass variability, ratios of ARV levels between seminal plasma and blood are typically lower for PIs than NRTIs or NNRTIs. 44 –55 We could not, however, definitively evaluate the impact of ARVs on viral decay rate in seminal plasma because of infrequent sampling following ARV initiation.
In summary, although our study represents the largest published analysis to date of seminal plasma HIV shedding during primary HIV infection, many questions remain unanswered. Future studies will require earlier and more frequent sampling to evaluate the timing of peak HIV RNA levels in seminal plasma and the extent to which penetration of ARVs into genital tract fluids and tissues affects the rate of viral decay in semen during primary HIV infection. Our data show that HIV RNA levels in seminal plasma (and, by inference, infectiousness) may remain elevated for 2 months or more following HIV infection. Future mathematical models that quantify the proportion of HIV transmission from individuals with primary HIV infection should incorporate genital tract HIV dynamics in order to assess the relative need for the expansion of public health interventions to identify individuals with acute and early HIV infection and prevent HIV transmission.
Footnotes
Acknowledgments
We would like to thank the subjects who provided specimens for this study, Terri Smith for data assistance, and Larry Corey, MD, John Krieger, MD, Michelle Berrey, MD, Timothy Schacker, MD, and Theresa Shea, PA-C for their previous work on this project. Financial support was provided by NIH K23 AI-65243 (J.S.), NIH R01 AI-55343 (S.H.), NIH U01 AI-41535, NIH P01 AI-57005, and CFAR Laboratory Core Grant AI-27757, DK-49477, and AI-38858. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. Presented in part at the 13th Conference on Retroviruses and Opportunistic Infections, Denver, CO, February 5–8, 2006, abstract #396.
Disclosure Statement
Pharmaceutical support was provided by Bristol-Myers Squibb (formerly DuPont Pharmaceuticals Co.), GlaxoSmithKline, and Merck & Co, Inc.