
Abstract
HIV infection increases the oxidative stress process, and antiretroviral combination therapy increases protein oxidation and preexistent oxidative stress. The latter induces production of reactive oxygen species. Lipid peroxidation (LPO) is a means of determining oxidative stress. There is also a deficiency of glutathione in HIV infection. Persistent oxidative load leads to an accelerated rate of consumption of glutathione (GSH). This study measured LPO and GSH levels in plasma of HIV-infected individuals with or without therapy and compared these with healthy controls. One hundred HIV-infected individuals and 30 healthy controls were included in the study. LPO and GSH levels were measured in plasma according to previously described methods. The mean level of LPO in HIV-infected individuals was 0.7 ± 0.1 μmol/ml (range, 0.5–0.9 μmol/ml), whereas the mean LPO level in controls was 0.3 ± 0.1 μmol/ml (range, 0.2–0.4 μmol/ml). The mean LPO levels were significantly higher in HIV-infected individuals as compared to healthy controls (p value <0.0001). The mean GSH level in HIV-infected individuals was 0.06 ± 0.01 μmol/ml (range, 0.03–0.08). The mean GSH level in healthy controls was 0.09 ± 0.01 μmol/ml (range, 0.05–0.1). The mean glutathione level in HIV-infected individuals was significantly lower in compared to healthy controls (p value < 0.0001). There was a significant positive correlation between absolute CD4 cells and GSH levels (ρ = 0.182, p = 0.045). There is increased oxidative stress in HIV-infected patients. Whether supplementation with antioxidants will reduce this oxidative stress is still unknown.
Introduction
HIV
The infection is characterized by functional and structural changes related to the immunological system. Increased production of ROS such as superoxide anion, hydroxyl radical, and hydrogen peroxide may be related to an increased activation of polymorphonuclear leukocytes during infections or influenced by the prooxidant effect of proinflammatory cytokines produced by activated macrophages during the course of HIV infection. 3
ROS can attack double bonds in polyunsaturated fatty acids, inducing lipid peroxidation (LPO), 4 which may result in more oxidative cellular damage. 5,6 Thus, measurement of LPO is a means of determining oxidative stress. Such damage may be prevented or moderated by a normal antioxidant defense system that scavenges the ROS. Glutathione (γ-glutamylcysteinylglycine, GSH), a tripeptide present in high concentrations in all mammalian cells, has many critical protective and metabolic functions. It detoxifies electrophilic metabolites of xenobiotics and protects cells from the toxic effects of free radicals and reactive oxygen compounds. 7 It is also important in the immune response to infections and plays an important role in lymphocyte proliferation, antibody-dependent and cell-mediated cytotoxicity, and protection of lymphocytes against superoxides that are produced to destroy invading pathogens. 8,9
There have been numerous reports of GSH deficiency in HIV infection. The concentration of GSH is lower in plasma, lung epithelial lining fluid, and peripheral blood mononuclear cells (PBMCs) of HIV-infected individuals. 10 –12 Moreover, in vitro studies have shown that low GSH levels impair T cell function 12 and also promote HIV expression, 13 suggesting a link between GSH deficiency and progression of HIV disease. This was confirmed by a recent report of poor survival rates of HIV-infected individuals with lower GSH levels and improved survival when GSH was replenished. 14 Alternatively, because GSH levels fall under conditions of increased oxidative stress, such as HIV infection, it can be proposed that a persistent oxidative load leads to an accelerated rate of consumption of GSH that is not matched by an equal increase in the rate of synthesis of the tripeptide.
The purpose of the present study was to measure the plasma levels of LPO and GSH in an HIV-positive population, either asymptomatic or with AIDS, and to compare these results with those in age-matched apparently healthy control subjects.
Materials and Methods
This was a cross-sectional study. One hundred HIV-seropositive individuals were selected from the Immunodeficiency Clinic of the Internal Medicine Department of the Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh, from January 2007 to June 2007. Thirty aged- and sex-matched apparently healthy seronegative individuals were included as healthy controls. Informed consent was obtained from all individuals.
A complete medical history was taken and a physical examination was carried out to screen patients for opportunistic infections and coinfections. HIV-seropositive individuals were classified as per WHO staging. Two nucleoside reverse transciptase inhibitors and one nonnucleoside reverse transcriptase inhibitor were started as per WHO guidelines. 15
Assay procedure
LPO and GSH analyses were performed as per the methods described by Ohkawa et al. and Beutler et al., respectively. 16,17 Five milliliters of blood was drawn into pyrogen-free blood collection EDTA tubes. The sample was centrifuged and plasma was stored in 1-ml aliquots at −20°C.
Measurement of LPO
For LPO, 100 μl of plasma was incubated with 100 μl of distilled water and 50 μl sodium dodecyl sulfate (SDS) at room temperature for 10 min. Following incubation, 375 μl of 20% acetic acid and 375 μl of thiobarbituric acid (TBA) were added and the reaction mixture was boiled for 1 h, cooled, and then extracted with 1 ml of an n-butanol-pyridine mixture to avoid turbidity. The upper layer of each sample was taken and absorbance at 532 nm was measured. 16
Measurement of GSH
In brief, 0.5 ml of plasma was mixed with 1.5 ml of distilled water and 3 ml of precipitating reagent in a test tube. The mixture was allowed to stand for 5 min and filtered. One milliliter of filtrate was taken in another test tube and 4 ml of phosphate solution and 0.5 ml of 5,5′-dithiobis-2-nitrobenzoic acid (DTNB) reagent were added. Optical density was measured within 5 min at 412 nm against a test blank (containing distilled water). GSH in a concentration of 20–140 μg was used as a standard and the levels of GSH were expressed as μmol/g Hb. 17
Statistical analysis
LPO and GSH levels in HIV-infected individuals and healthy controls were compared by unpaired t-test using Graph pad prism software. Descriptive data were expressed as mean ± SD for nonparametric distribution. Spearman rank correlation was used to correlate CD4 cell count with LPO and GSH levels. A p-value of less than 0.05 was considered statistically significant.
Results
Sixty-nine HIV-seropositive males and 31 HIV-seropositive females were selected from the Immunodeficiency Clinic of Internal Medicine department at PGIMER. The mean age of the HIV-seropositive individuals was 34.1 ± 7.3 years (range, 22–53; median, 32 years). The mean hemoglobin of HIV-seropositive individuals was 11.8 ± 1.8 g/dl (range, 6.3–15.8 g/dl). The mean absolute CD4 was 207.1 ± 151.6 cells/μl (range, 16–827 cells/μl).
Opportunistic infections in the form of pulmonary tuberculosis were seen in 12 patients: one had lymph node tuberculosis and one had pulmonary tuberculosis with toxoplasmosis, six patients presented with pneumocystis pneumonia, five had oral candidiasis, three patients had herpes zoster, one had cryptosporidiosis, one presented with cryptococcosis, one had chronic diarrhea, and one patient presented with progressive multifocal leukoencephalopathy. Thirty-four patients did not receive any medication. Fifty patients received a nevirapine-based combination regimen [stavudine (d4T)/zidovudine (AZT), lamivudine (3TC), nevirapine (NVP)], 15 patients received an efavirenz-based combination regimen (AZT, 3TC, EFV), and 1 received a nelfinavir-based combination therapy (AZT, 3TC, NFV). The mean duration of treatment was 9.2 ± 7.0 months.
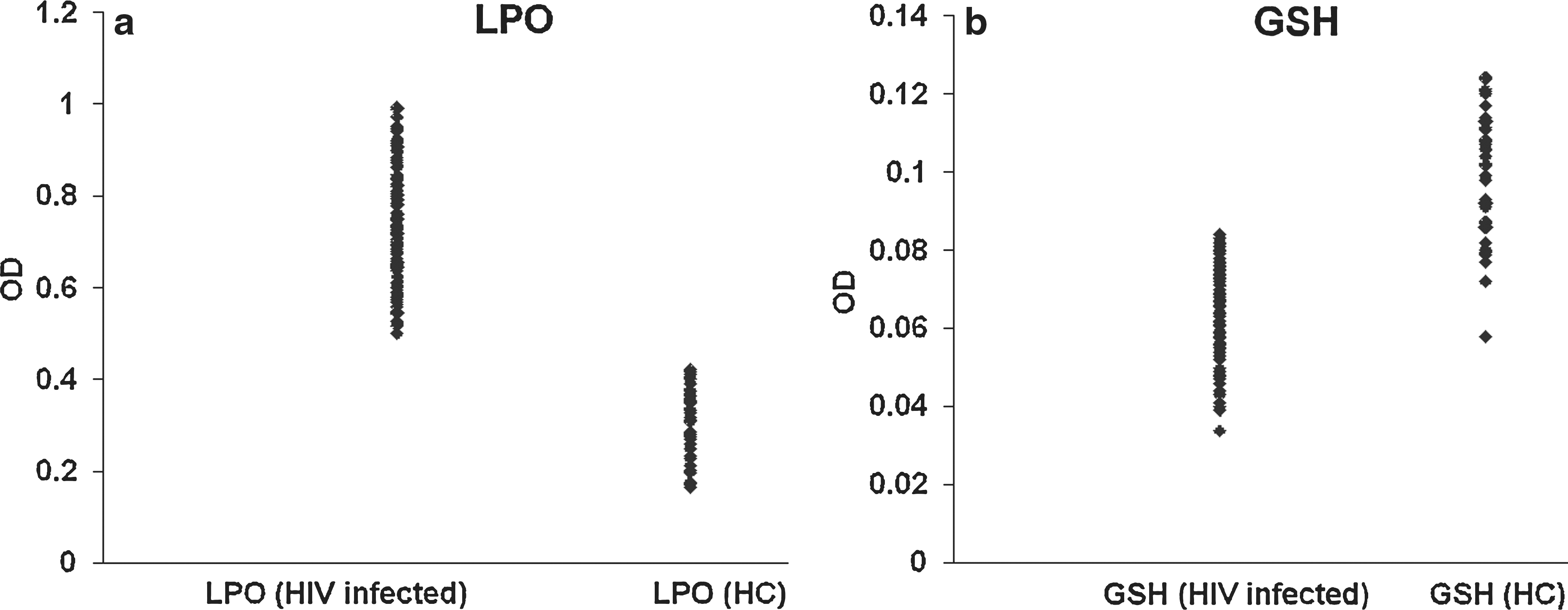
Figure 1a shows the scatter plot of LPO levels measured in plasma of 100 HIV-infected patients and 30 healthy controls. The mean level of LPO in HIV-infected individuals was 0.7 ± 0.1 μmol/ml (range, 0.5–0.9 μmol/ml), whereas the mean LPO level in controls was 0.3 ± 0.1 μmol/ml (range, 0.2–0.4 μmol/ml). The mean LPO levels were significantly higher in HIV-infected individuals as compared to healthy controls (p value < 0.0001) (Fig. 1a). Figure 1b shows the scatter plot of GSH levels measured in plasma of HIV-infected patients and healthy controls. The mean GSH level in HIV-infected individuals was 0.06 ± 0.01 μmol/ml (range, 0.03–0.08). The mean GSH level in healthy controls was 0.09 ± 0.01 μmol/ml (range, 0.05–0.1). The mean glutathione level was significantly lower in HIV-infected individuals as compared to healthy controls (p value < 0.0001).
(
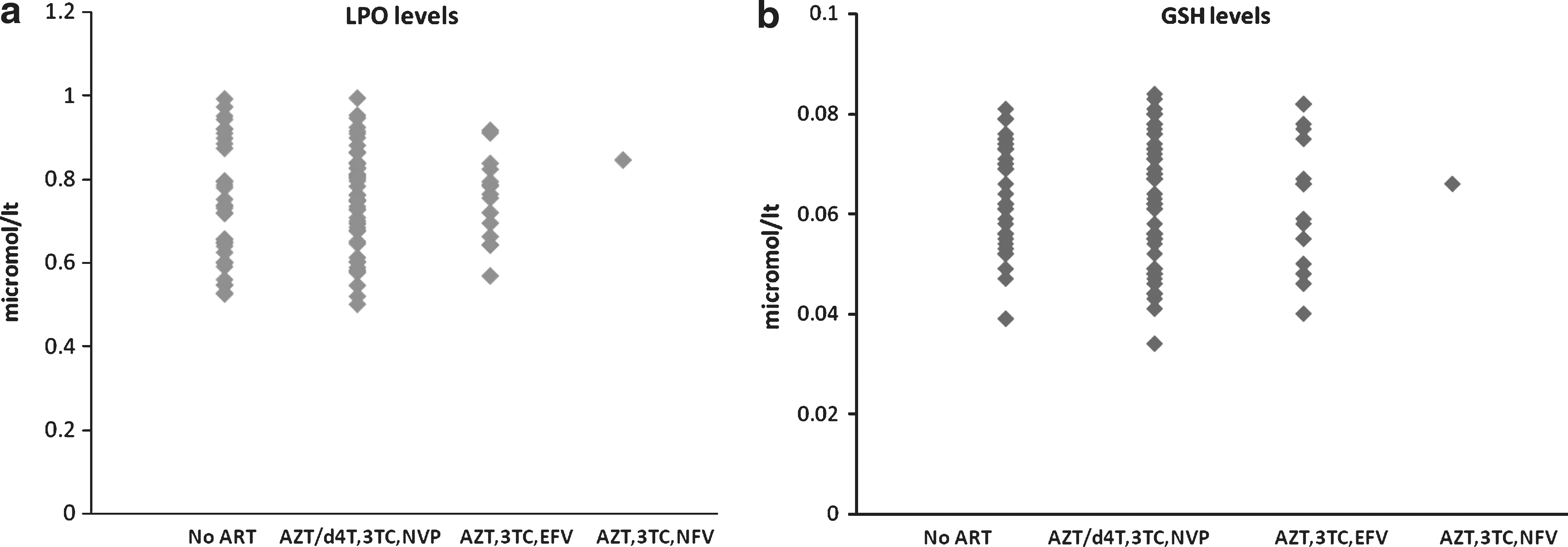
Figure 2 shows scatter plots depicting LPO and GSH levels, respectively, in cohorts that were not on antiretroviral therapy (ART) compared with those on various ART regimens. There was no statistically significant difference in the mean levels of LPO (p value 0.86) and mean levels of GSH (p value 0.51) in the HIV-infected group not on therapy versus the individuals on various ART regimens taken together as one cohort. Also, no statistical significant difference was noted between mean LPO levels (p value 0.68) and mean GSH levels (p value 0.53) in HIV-infected individuals with and without tuberculosis. There was significant positive correlation between absolute CD4 cells and GSH level (ρ = 0.182, p = 0.045); however, no such correlation was evident between CD4 cells and LPO levels (ρ = 0.011, p = 0.912). The duration of therapy did not show any correlation either with GSH levels (r = 0.01, p = 0.9) or with LPO levels (r = 0.08, p = 0.5). There was, however, an inverse correlation noted between LPO levels and GSH levels (r = –0.5, p < 0.01).
(
Discussion
Oxidative stress is the common mediator of apoptotic (programmed) cell death in HIV/AIDS. Antiretroviral combination therapy increases protein oxidation as well as the level of oxidative stress already present in HIV infection. 18 The use of highly active antiretroviral therapy (HAART) has improved the clinical evolution of these patients. However, some patients still show higher oxidative stress and other effects of HAART, such as change in lipid and muscle metabolism. 19 HIV-infected people tend to have subnormal GSH levels in plasma, lung epithelial lining fluid, and PBMCs. 10 –12 Multiple mechanisms may contribute to systemic GSH deficiency in HIV disease, including excessive production of inflammatory cytokines and use of GSH-depleting drugs such as acetaminophen. 20 Release of HIV-TAT (trans-acting transcriptional activator) blocks transcription of manganese superoxide dismutase, an enzyme that helps to prevent oxidative stress, and markedly decreases the activity of glucose-6-phosphate dehydrogenase, a key enzyme in pathways that maintain GSH in its reduced state. 21
In this study, standardized methods by Ohkawa et al. and Beutler et al. were used to study LPO and GSH levels. 16,17 The increased LPO levels and reduction in GSH levels in HIV-infected individuals as compared to healthy controls are consistent with those of many studies published previously. The results showed that in HIV-infected individuals oxidative stress was significantly higher than in noninfected individuals. However, there was no significant difference found in the levels of LPO and GSH between HIV-infected individuals receiving therapy and those without therapy. This is consistent with the result of previous study from Southern India. 21
A study by Aukrust et al. had also shown that during HAART, increases in CD4 cell count were accompanied by improvement in GSH-redox status and an increase in the subnormal levels of antioxidant vitamins, but HAART did not induce full normalization of these parameters. 19 Jahoor et al. had shown that GSH deficiency of HIV-infected individuals is due in part to a reduced synthesis rate secondary to a shortage in cysteine availability. There have been numerous reports of increased LPO and GSH deficiency in HIV infection. 22 Allard et al. had also shown lower concentrations of antioxidant compounds and higher contents of the products of oxidative reactions in HIV-infected individuals than in noninfected individuals. 23 Also, in the present study, no statistically significant difference was noted between LPO levels in HIV-infected individuals with and without tuberculosis (p value 0.68). This might be because all individuals with tuberculosis received antitubercular therapy and none of the individual enrolled had active tuberculosis.
Oxidative stress may decline with treatment in individuals with dual infection. The mechanism underlying the increased oxidative stress in the HIV population remains unclear. In addition to an excessive production of reactive oxygen species, which may be explained by polymorphonuclear leukocyte activation during infectious conditions or by a prooxidant effect of tumor necrosis factor-α produced by activated macrophages, a weakened antioxidant defense system may play a role. 22 Because it is known that GSH peroxidase plays a central role in the metabolism of reactive oxygen species, antioxidant supplements may have an effect on oxidative stress in HIV-infected individuals. 24,25
It is possible that maintenance of antioxidant defenses will be more important as survival is prolonged indefinitely, because the accumulation of tissue damage due to oxidative stress may take a long time to manifest. It is also possible that antioxidant therapy would be more beneficial in acute rather than chronic conditions because oxidative stress is much greater during acute processes, such as opportunistic infections, than during periods of clinical stability.
Thus, the potential for therapeutic benefit from antioxidant therapies remains questionable. The relationship between HIV viral content and oxidative stress as well as the effect of current antiretroviral therapies on oxidative stress need to be determined.
Footnotes
Disclosure Statement
No competing financial interests exist.