
Abstract
The relationship of adipocytokine with the development of HIV-related lipodystrophy was investigated in a case-control study. Adipocytokine, lipid, and glycemic parameters were measured at every visit. Logistic regression analysis was used to assess the HIV-LD risk factors and the Spearman correlation coefficients test was used to assess the correlation between adiponectin with other metabolic variables. Most of the patients (96.3%) developed HIV-LD after month 12. Comparing the baseline adiponectin, the adiponectin concentration of the HIV-LD group rose by month 6 and began to decrease substantially by month 18; this reduction was maintained until month 30 (p < 0.05). Comparing the HIV-NLD group, the adiponectin concentration at months 18, 24, and 30 were significantly lower in the HIV-LD group. The leptin concentration of both the HIV-LD and HIV-NLD groups remained stable. Patients in the lower concentration of baseline adiponectin and greater adiponectin change rate at month 18 presented with increased odds ratio for HIV-LD. The adiponectin level had a correlation with serum triglycerides (r = −0.616, p < 0.0001), serum insulin concentration (r = −0.494, p = 0.001), and HDL-C (r = 0.673, p < 0.0001). The adiponectin concentration of HIV-LD began to decrease substantially by month 18. The lower baseline concentration of adiponectin and the greater change rate at month 18 were independent risk factors of HIV-LD. The adiponectin level had a correlation with serum triglycerides, serum insulin concentration, and HDL-C, suggesting that adiponectin may link the metabolic abnormalities and HIV-LD.
Introduction
HIV-
The dominant change of HIV-LD is reduction in subcutaneous adipose tissue (SAT). 6,7 Adipocytokine, fat-derived cytokines, were reported to link the changes in adipose distribution and the metabolic abnormalities in lipodystrophies in non-HIV-infected patients. 8 Therefore, we wish to investigate the relationship of adipocytokine and adipose distribution and the metabolic abnormalities of HIV-LD in this 30-month prospective study.
Materials and Methods
Subjects
Fifty-two consecutive, ambulatory, HIV-infected patients were recruited through the Infectious Diseases Clinic of the Peiking Union Medical College (PUMC) hospital in the study. Written informed consent was obtained in all cases. Patients with any active opportunistic infection, neoplasm, or wasting syndrome were excluded from the study. At baseline, all subjects were antiretroviral therapy (ART) naive.
Follow-up
All patients were evaluated before the initiation of HAART and every 6 months up to 30 months. All patients have been followed up for efficiency, adherence to highly active antiretroviral therapy (HAART), and side effects, especially the development of HIV-LD. The subjects returned to repeat the baseline assessments, which included body weight, height, total cholesterol, triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C), adipopectin, leptin, insulin, CD4 cell count, and viral load (VL). When HIV-LD was considered, dual-energy X-ray absorptiometry (DEXA) was taken to quantify the body fat composition.
Lipodystrophy definition criteria
Clinical evaluation of lipodystrophy was obtained in every case, and diagnosis was based on the concordance between the opinion of two clinical examiners and that of the patient. A questionnaire on fat distribution with four possible answers was used: no alterations, mild, moderate, and severe changes. Different body parts were examined: the face, the extremities, and the dorsocervical and abdominal regions. Body fat changes included subcutaneous lipoatrophy (hollow cheeks, prominent superficial veins in the limbs, or flattening of the buttocks) and central obesity (increased abdominal girth, breast enlargement, or dorsocervical fat pad). When concordance between the patient's opinions and that of the clinical examiner with at least moderate changes within the same anatomical location was reached, the diagnosis of lipodystrophy was considered. 9 –11
Individuals with HIV infection were divided into two groups based on the results of the patient's opinion and that of the clinical examiner. Those subjects who meet this diagnosis criteria of HIV-LD were placed in the lipodystrophy group (HIV-LD) and other patients were placed in the nonlipodystrophy group (HIV-NLD).
When the diagnosis of lipodystrophy was considered, the patient's body fat distribution was examined by DEXA (GE Lunar Prodigy Advance, Madison, WI). The percentage of limb fat was calculated as the total fat in the arms and legs expressed as a percentage of total body fat.
Laboratory measurements
Blood was drawn from each subject after an overnight fast on the morning of the study visit. Blood samples were immediately centrifuged at room temperature after collection. Total cholesterol, triglycerides, HDL-C, and LDL-C were determined by enzymatic methods using commercial kits (using previously published methods). CD4+ lymphocyte cell count was analyzed by three-color flow cytometry (Epics XL flow cytometry, Beckman Coulter, USA). Whole blood was incubated with monoclonal antibodies (MAb) against CD3 and CD4 (Immunotech, France). Absolute counts of CD3+CD4+ T cells were then calculated using the results from the complete blood cell and lymphocyte differential counts. Human immunodeficiency virus 1 VL was measured on frozen EDTA-plasma samples by a branched DNA assay (version 3.0, Bayer, USA). The limit of detection of the assay is from 50 copies/ml to 50,000 copies/ml. The plasma levels of insulin, leptin, and adiponectin were measured by in-house enzyme-linked immunosorbent assays (ELISA), which were all developed in the laboratory of the Department Endocrinology, Peking Union Medical College Hospital. The detection limit of the insulin assay was 0.8 pmol/liter, with no crossreactivity to proinsulin (<0.01%), and the assay had an interassay CV of <9.0%. Leptin sensitivity is 0.2 ng/ml with interassay CV <9.3%, respectively. The detection limit of the adiponectin assay was 0.5 ng/ml and the interassay CV was <10%. 12 –14
Statistical analysis
Statistical analysis was performed using SPSS 11.5. Continuous variables are presented as means and SDs or medians. Data of viral load were logarithmically transformed to obtain near normality before analysis. Because some data were not normally distributed, as determined with the Kolmogorov-Smirnov test, Wilcoxon rank sum was used to compare variables that were not normally distributed. A χ2 test was used to compare categorical variables. Risk factors for HIV-LD were assessed using a stepwise logistic regression analysis. Associations among adiponectin, leptin, anthropometric variables, metabolic variables, CD4 count, and HIV RNA were determined using the Spearman correlation coefficients test. A p value of 0.05 was used to test for statistical significance, and all statistical tests were two tailed.
Results
At baseline, all the 52 ART-naive subjects were without alteration in fat distribution. The baseline characteristics in the subjects are summarized in Table 1. During the follow-up period of 30 months, 27 subjects developed HIV-LD; the other subjects remained HIV-NLD. Comparing to those who remained HIV-NLD, subjects who developed HIV-LD had a lower level of CD4 cells and lower adiponectin concentration at baseline (p < 0.05). Age and viral burden were not significantly different between the HIV-LD and HIV-NLD groups. The metabolic parameters BMI (body mass index), total cholesterol, HDL-C, LDL-C, triglycerides, leptin, and insulin were not significantly different between the two groups.
Data are measured as n ± SD or median (interquartile range).
p value with sex adjusted.
Of the 52 subjects, 35 patients (67.3%) commenced stavudine (d4T) with didanosine (ddI) as their nucleoside reverse transcriptase inhibitors (NRTI) backbone and 5 subjects (9.6%) started with d4T plus lamivudine (3TC). In all, 40 subjects (76.9%) commenced a d4T-containing regimen. Twelve patients (23.1%) began with a zidovudine (ZDV)-containing regimen [nine subjects (17.3%) with 3TC and three subjects (5.8%) with DDI]. Only one patient used a protease inhibitor (PI)-containing regimen (indinavir), while the others used either nevirapine (NVP) (76.5%) or efavirenz (EFV) (21.5%) as their nonnucleoside reverse transcriptase inhibitors (NNRTI) backbone. Of subjects (26/27) who developed HIV-LD 96.3% used a d4T-containing regimen and 56% of the subjects (14/25) who remain HIV-NLD used a d4T-containing regimen. The percentage of patients using d4T was significantly different between the two groups (p = 0.001, Table 1).
During the follow-up period of 30 months, one patient developed HIV-LD at month 12 and four patients developed HIV-LD at month 18. Most of the patients (96.3%) developed HIV-LD after month 12 and 81.5% of the patients developed HIV-LD after month 18. When the diagnosis of lipodystrophy was considered, the patient's body fat distribution was examined by DEXA. The results of DEXA are shown in Table 2. Total fat and total fat percentage of subjects who developed HIV-LD were significantly lower than that of subjects who remained HIV-NLD (p < 0.05). Compared with the HIV-NLD group, extremity fat and extremity fat percentage were significantly lower and trunk fat percentage was significantly higher in the HIV-LD group. There was no difference in the trunk fat in the two groups. The extremity fat:trunk fat ratio was lower in the HIV-LD group (p < 0.05).
Comparing the baseline adiponectin concentration, the adiponectin concentration of the HIV-LD group rose by month 6. The adiponectin concentration of the HIV-LD group decreased substantially by month 18 and this reduction was maintained until month 30 (p < 0.05). However, the adiponectin concentration of the HIV-NLD group remained stable (Fig. 1). As Fig. 1 shows, comparing the HIV-NLD group, the adiponectin concentration at months 18, 24, and 30 was significantly lower in the HIV-LD group.
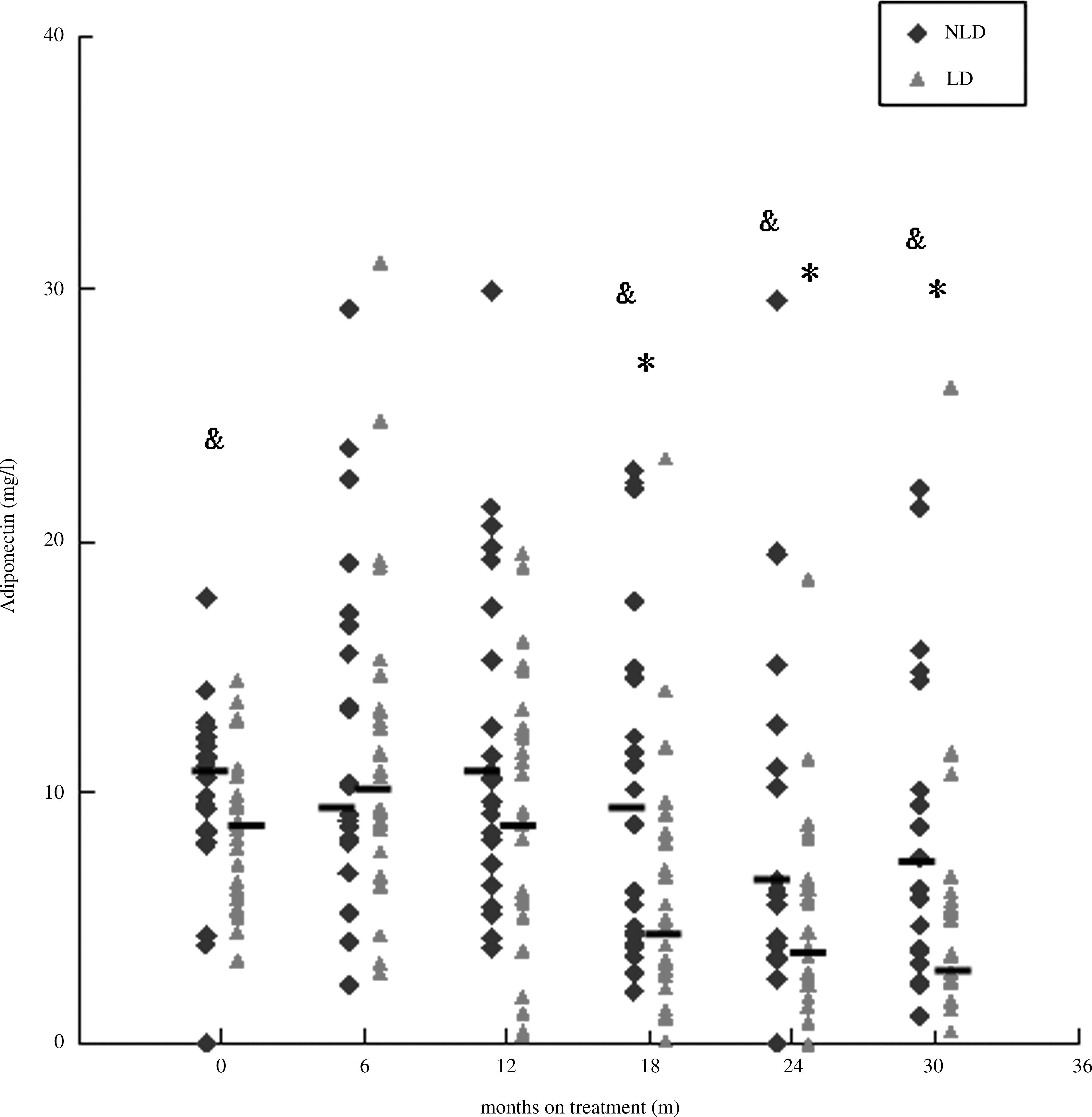
Adiponectin in relation to HIV-LD. LD, HIV-related lipodystrophy patients; NLD, HIV non-LD patients. *Levels at 18, 24, and 30 months versus baseline level in the HIV-LD group, p < 0.05; &HIV-LD versus the HIV-NLD group, p < 0.05.
The leptin concentration of both the HIV-LD and HIV-NLD group remained stable (Fig. 2). The leptin concentration of the HIV-LD group at month 12 was lower than the baseline leptin concentration; however, it had not reached statistical significance.

Leptin in relation to HIV-LD. LD, HIV-related lipodystrophy syndrome patients; NLD, non-LD patients. &HIV-LD versus the HIV-NLD group, p < 0.05.
Factors associated with HIV-LD are presented in Table 3. We found that there is a significant difference of adiponectin between the HIV-LD group and HIV-NLD group, with most of the HIV-LD occurring after month 12; this step logistic regression analysis model also included adiponectin concentration and changing rate at month 6, month 12, and month 18 in addition to other metabolic parameters on baseline line. Change rate of adiponectin was expressed as (adiponectin – baseline adiponectin) baseline adiponectin. The resulting analysis showed that baseline adiponectin concentration and change rate of adiponectin at month 18 were both risk factors associated with the development of HIV-LD.
ADP, adiponectin.
We also found that adiponectin had an inverse correlation with serum triglycerides (r = −0.616, p < 0.0001) and serum insulin concentration (r = −0.494, p = 0.001). We also found a positive correlation with HDL-C (r = 0.673, p < 0.0001). No significant associations were noted between adiponectin and leptin, total cholesterol, LDL-C, CD4, and viral load (Table 4).
Discussion
The prevalence of HIV-related lipodystrophy in patients on HAART is approximately 40% 15 and may reduce adherence to HAART, while the metabolic abnormalities, such as dyslipidemia and insulin resistance, are reported to increase the risk of cardiovascular disease. 16
d4T is regarded as one of the medications that can induce HIV-LD. In China, there are 650,000 people who are living with HIV infection, including about 75,000 AIDS patients. The Chinese government provides seven kinds of free antiretroviral drugs; d4T, one of these drugs, is still in extensive use in China. In this study, the development of most of HIV-LD was mainly related to the use of d4T. The DEXA data in our study indicated that the dominant change of HIV-LD is reduction of extremity fat. Our data show that most of the HIV-LD occurred after month 12 (96.3% after month 12 and 81.5% after month 18), which was consistent with the study of Kingsley et al. and Mahajan et al. 17,18
Our results indicated that the adiponectin concentration of the HIV-LD group decreased substantially by month 18 and this reduction was maintained until month 30. Adiponectin is a 30-kDa protein solely produced by adipocytes secreted by differentiated adipocytes. 19,20 Recent studies have shown that adiponectin expression is higher in subcutaneous fat than visceral fat in humans. Subcutaneous adipose tissue (SAT) accounts for approximately 85–90% of adipose tissue in lean individuals and SAT may produce the majority of circulating adiponectin. This adiponectin deficiency becomes prominent with peripheral fat loss and thus loss of the adiponectin supply. Therefore, subcutaneous fat loss may actually be responsible for the decreased adiponectin level in the HIV-LD group. A decreased level of adiponectin has been seen in animal models of lipoatrophy. 21 Our data also show that the adiponectin concentration of the HIV-LD group rose by month 6. The reason for the increase in the adiponectin level after a few weeks or months of therapy was probably a compensatory response from the adipose tissue through a negative feedback mechanism at least at the initial stages of the metabolic dysregulation.
Since plasma adiponectin was related to the total content of subcutaneous tissue in HIV-infected patients and the dominant change of HIV-LD is reduction in SAT, the correlation of the low level of adiponectin and the development of HIV-LD is that of a covariate, rather than a cause. Adiponectin has also been reported to be inversely associated with rare forms of congenital and acquired lipodystrophies in non-HIV-infected patients. Addy et al. found that adipnectin levels were significantly lower in the HIV-infected patients exhibiting fat redistribution changes. 22 However, this was a cross-sectional study and cannot show the dynamic change of adiponectin during the course of HAART.
The mechanism of the correlation of adiponectin and HIV-LD has not been well understood. HIV-LD have been associated with high circulating levels of TNF-α. 23 Increased TNF-α gene expression has also been found in subcutaneous fat from patients with HIV lipodystrophy. 24 TNF-α inhibits adiponectin gene expression and secretion from adipocytes in vitro. 25 Therefore, this cytokine may play a role in the reduced adiponectin concentrations. In vitro, stavudine has been shown to reduce adiponectin secretion from adipocytes. 26 The independent association of stavudine use with low adiponectin levels suggests that stavudine may not only reduce fat, but also alter adipocyte function.
The previous study data on leptin are complex. Some cross-sectional studies suggest leptin level remain proportional to total adiposity in HIV-LD. When patients with HIV lipodystrophy have total body fat mass similar to controls, leptin levels are similar to those of both HIV-infected and healthy controls. 27,28 However, when lipodystrophy is accompanied by lower total body fat mass, leptin levels are lower compared to controls. 26 Our observation of stable leptin concentration in patients with HIV-LD is not consistent with these observations in cross-sectional studies. In our study, patients with HIV-LD also have lower total body fat weight than the HIV-NLD group, although leptin levels are still similar to that of the HIV-NLD group. The reason why it is different from the previous study is still not very clear and needs further research.
It has been reported that the development of lipodystrophy syndrome is clearly influenced by the type of ART and the duration of treatment and that d4T is strongly associated with the loss of subcutaneous fat. 29 –31 Older age 32 and low nadir CD4 cell count 33 have both been identified as risk factors for lipodystrophy. The results of our study indicated that baseline adiponectin and the change in rate of adiponectin at month 18 were independently associated with the development of HIV-LD. The inverse correlations of the development of HIV-LD with low baseline adiponectin and greater change rate of adiponectin at month 18 suggest that individuals with lower pretreatment adiponectin levels or with adiponectin decreasing more significantly are more likely to experience HIV-LD.
Serum adiponectin levels demonstrated a strong negative relationship with indices of insulin resistance such as fasting insulin and triglycerides in the study of diabetes and rare lipodystrophy in non-HIV-infected patients. Our data showed a similar inverse correlation between adiponectin level and serum triglycerides and insulin concentration in HIV-LD. We also found a positive relation between adiponectin and HDL-C concentration. Therefore our result suggests that reduced serum adiponectin levels may contribute to metabolic complications in patients with HIV-LD and might link the metabolic abnormalities and the changes in adipose distribution in HIV-LD.
Our study has a number of limitations: the sample size was relatively small and only representative of those infected with HIV-1 in China, where d4T with ddI is one of the most commonly used medication combinations as an NRTI backbone. The question of whether these associations have the same predictive power in more diverse populations commencing other ART regimens remains unanswered. Given the exploratory nature of our analysis, these findings need further validation in routine clinical care models.
Footnotes
Acknowledgments
We thank Yi Dai for evaluating the patients in the Infectious Diseases Clinic of the Peiking Union Medical College hospital. This study was supported by the National Key Technologies R&D Programme for the 11th Five-year Plan (2008ZX10001-006), Ministry of Health Clinical HIV/AIDS Research Grant (2007–2009), and Beijing Science and Technology Program Fund (D0906003040491).
Disclosure Statement
No competing financial interests exist.