
Abstract
The National Government HAART Program (NGP) for the provision of HAART to uninsured HIV-infected persons in Mexico began in 2001. The objective was to describe the virologic outcome of patients enrolled in the NGP in a large HIV treatment center in Mexico City. HIV-infected persons, naive or ≤6 months on HAART, who entered the NGP from 2001 to 2005 were included. Patients with virological suppression were compared to those with virologic failure (VF) during follow-up. Of 377 patients enrolled, 191 where eligible for analysis. The median age was 35.9 (18–75 years) and 85% were male. The median baseline CD4+ T cell count was 183 cells/mm3; 63.9% had <200 cells/mm3 and/or an AIDS-defining event. During follow-up (median: 17.77 months), 55 patients (28.7%) changed their first regimen: 8.3% because of VF and the remaining due to toxicity. The probability of VF at 48 months was 20%. VF was associated with age <30 years (p = 0.003, RR 4.7, IC 95% 1.5–14.4). The use of NNRTI was associated with lower risk of VF (p = 0.042, RR 0.3, IC 95% 0.12–0.99). Nadir CD4+ and AIDS-defining at baseline were not associated with VF. Implementation of NGP for HAART access in a specialized care setting in Mexico resulted in an excellent virologic response. Younger age was a significant risk factor for VF.
Introduction
T
The objective of the study was to assess the virologic effectiveness, durability, and outcomes of the first regimen of HAART in HIV-infected patients in Mexico who received their medication through the Program for free access to HAART financed by the Government (from here on described as the Government HAART Program, NGP) and who were seen at the HIV Clinic of the INCMNSZ in Mexico City.
Materials and Methods
Study design
We conducted a retrospective cohort study in the HIV Clinic of the Department of Infectious Diseases at INCMNSZ, which is a reference center for adults. Children as well as pregnant women are referred to other centers specialized in the treatment and care of these populations.
Study population
Patients eligible for inclusion in this study were those seen at the HIV Clinic between January 1, 2001 and September 30, 2005. For inclusion in the study patients had to be ≥18 years old and had to be antiretroviral (ARV) naive and receiving their ARV medication through the Government HAART Program. Only patients who initiated treatment once admitted to our clinic or for a maximum of 6 months before were evaluated. The reason for excluding patients who initiated treatment before that period is the unreliable information on ARV history and baseline characteristics in such cases. Other patients excluded were those who were already in a second or subsequent HAART regimen on admission and those who had no CD4+ values at baseline.
The first regimen of ARV prescribed was decided by the health care provider seeing the patient. Because this is an academic institution most of the providers were Infectious Disease trainees who follow international and national treatment guidelines with no particular restriction based on availability. Additionally, there is supervision by senior Infectious Disease staff members.
For effectiveness evaluation, only patients with at least 6 months of HAART and one or more HIV-1 viral load determination after 6 months were included. Patients who changed regimen because of toxicity were not considered as virologic failures in the analysis.
Data collection
The information was obtained by queering the database available at the HIV/AIDS clinic at INCMNSZ. This database has been prospectively collecting data from all patients seen at the clinic since the year 2000. It includes demographic characteristics (age, gender, nationality, educational level, occupation) and information related to HIV infection itself (date of diagnosis, route of transmission, care and treatment history). All information is collected during scheduled visits by the treating physician and evaluated for quality control. In every visit the physician in charge completes the following information for each patient: clinical stage of HIV, current treatment, if there was any change in treatment and the reason, and if the patient has had missed doses of ARVs (addressed in number of days omitted; no adherence questionnaires are applied routinely). Also, the last CD4+ count and viral load are registered. Viral load and CD4 determinations are drawn according to the physician's criteria in our center ideally every 3–6 months.
The following data were extracted for analysis: date of entry to the program, age, gender, route of transmission, educational level, as well as initial and subsequent HIV viral load and CD4+ count determinations, initial HAART regimen (focused on the third agent of the regimen) changes, and reasons for change during follow-up.
Definitions
We defined virologic failure (VF) as an HIV-1 viral load >500 copies/ml after 6 months of starting HAART while taking ARV drugs. For this analysis subjects who died were considered to be virologic failure. Failure of retention in the NGP was defined as those patients who did not attend a medical visit for >18 months. For outcome analysis purposes (virological failure) only patients who were followed for at least 6 months were included.
Poor medication adherence was defined as a patient who declared in any medical visit that they omitted one or more days of their ARV medication.
Statistical analysis
SPSS program version 12 was used. For the evaluation of the distribution of variables Kolmogorov-Smirnoff was used. Continuous variables were expressed in mean and standard deviation, or median and range minimum and maximum, depending on their distribution. Categorical variables were expressed in percentage. For the comparison between groups χ2 and the exact Fisher test was used. A Kaplan–Meier analysis was performed to evaluate the probability of retention to the NGP and the time to virological failure. For risk factors associated with virological failure and death, the following variables were used: age, gender, transmission route, educational level, basal immunologic status, first ARV regimen used, and basal viral load of HIV. Odds ratios were estimated with confidence interval at 95%. All p < 0.05 was considered significant.
The study was approved by the Bioethical Committee Board of the Instituto Nacional de Ciencias Médicas y Nutrición, Salvador Zubirán.
Results
During the study period 377 patients accessed ARVs through the Government HAART Program and 191 of them met the inclusion criteria (see Fig. 1). The number of patients who started HAART was 20 in 2001, 33 in 2002, 47 in 2003, 40 in 2004, and 51 in 2005. Eleven patients (5.7%) were considered failure to retention in the NGP during the period of time of this study. The median follow-up was 17.7 months (range: 0–55 months) and the probability of retention in the NGP was >80% at 4 years according to Kaplan–Meier analysis.
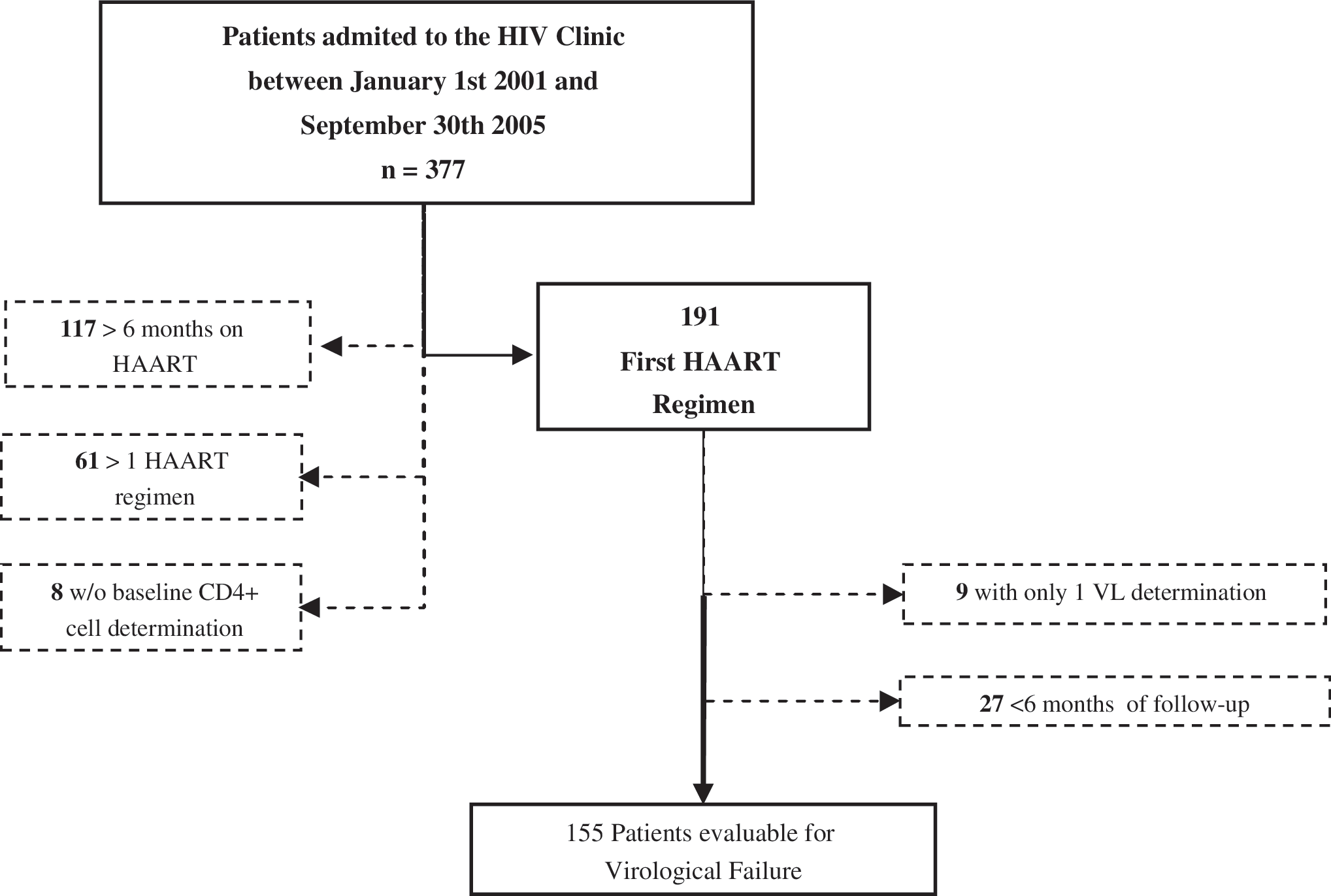
Study design and patient disposition.
Baseline characteristics
The baseline characteristics of the patients included in the study are shown in Table 1. The median age was 35.9 (range: 18–75 years) and most were male (85.3%); 66.5% had an educational level of 12 years or more, with only six of the 191 patients (3.2%) having no education at all. The most frequent risk factor for HIV infection was men who have sex with men (64.5%) followed by heterosexual transmission (33%). Only 3 of the 191 subjects had a history of injection drug use. The median CD4+ T cell count at baseline was 183 cell/mm3 (range: 4–541) with 63.9% of the cohort having a CD4+ T cell count less than 200 cell/mm3 and/or an AIDS-defining event at the time of HAART initiation. An HIV-1 viral load was available in 81.1% prior to starting HAART and in 91% of these viral load determinations were performed at the virology laboratory of Instituto Nacional de Ciéncias Médicas y Nutrición where the upper limit of the assay used is ≥75,000 copies/ml. The proportion of patients with an HIV-1 viral load of ≥75,000 copies/ml at baseline was 56%.
MSM, men who have sex with men; IVDU, intravenous drug users; VL, viral load.
Antiretroviral therapy
Nonnucleoside reverse transcriptase inhibitors (NNRTIs) were the most frequently prescribed third agent used as initial therapy (67%), mostly efavirenz-based therapy [n = 125 (65%)], followed by boosted protease inhibitors (PIs) (30.4%). Only 2.6% started with a combination of three NRTIs. In 2001, NNRTIs were prescribed in 40% of patients, but their use as a third agent increased from 40% in 2001 to 67% by 2005. Likewise, PI use in the first ARV regimen decreased from 55% in 2001 to 33% in 2005. In the past 2 years, no patients began HAART with three NRTIs (see Fig. 2). Among women, the use of NNRTIs as a third agent was less frequent (44.8% vs. 71% for men; p = 0.006). A total of 137/191 (71.7%) used zidovudine and lamivudine as the backbone of their first regimen, followed by stavudine and lamivudine (12.5%) and abacavir and lamivudine (10.4%). During the study period, 52 patients changed their first regimen (27.4%), 32 due to ARV toxicity, 16 patients because of VF, and 4 for other reasons. Of the 32 patients who changed their regimen because of toxicity, anemia was the most common reason (30.5%), followed by hypertriglyceridemia (25%), renal disturbances (16.6%), and rash (8.3%). Other reasons for changes were regimen optimization (mostly the change of three NRTIs to a regimen with either NNRTI or PI, n = 2) and potential drug interaction (n = 2; tuberculosis in patients on PIs). Nineteen patients experienced a toxicity event leading to discontinuation during the first 6 months on HAART. Of these patients, 2 did not achieve the 6 months of follow-up required for analysis of virological failure. The median duration for the first regimen was 19.3 months (range: 1–52).
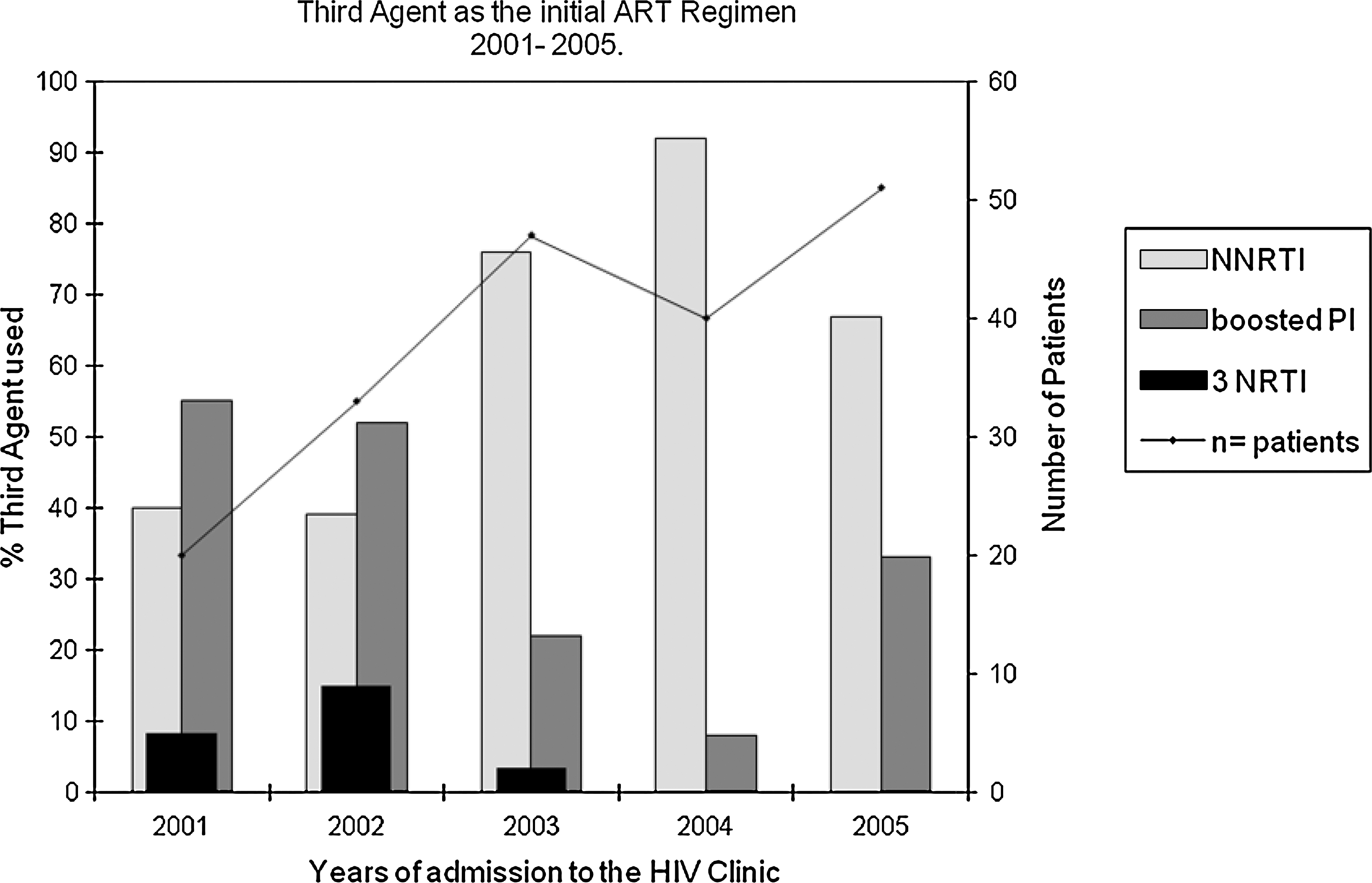
Third agent used as initial HAART and the number of patients admitted to the HIV clinic.
Virological failure (VF)
Ninety-five percent of patients (182 out of 191) had at least one viral load measurement after starting HAART and 142 of them (78%) had an HIV-1 viral load of <50 copies/ml at their last medical visit. The probability of having VF at 4 years of follow-up was <20% by Kaplan–Meier analysis (see Fig. 3). One hundred and fifty-five patients had more than 6 months of follow-up with their first HAART regimen. Sixteen of them developed VF (10.3%). None of the patients who changed their first regimen because of toxicity developed VF during the period of time of the study. In univariate analysis, age <30 years (p = 0.003, RR 4.7, IC 95% 1.5–14.4) and the voluntary interruption of ARVs during follow-up (p = 0.001, RR 6, IC 95% 1.8–19.8) were strongly associated with VF. On the other hand, the use of NNRTI as a third agent was associated with lower risk of VF (p = 0.042, RR 0.3, IC 95% 0.12–0.99). Female gender was marginally associated with VF compared with male gender, (p = 0.051; RR 3.3 CI 95% 1.0–7.14). Other factors, such as baseline CD4+ count, baseline viral load, the presence of an AIDS-defining event, and educational level, were not found to be associated with VF in our cohort (Table 2).
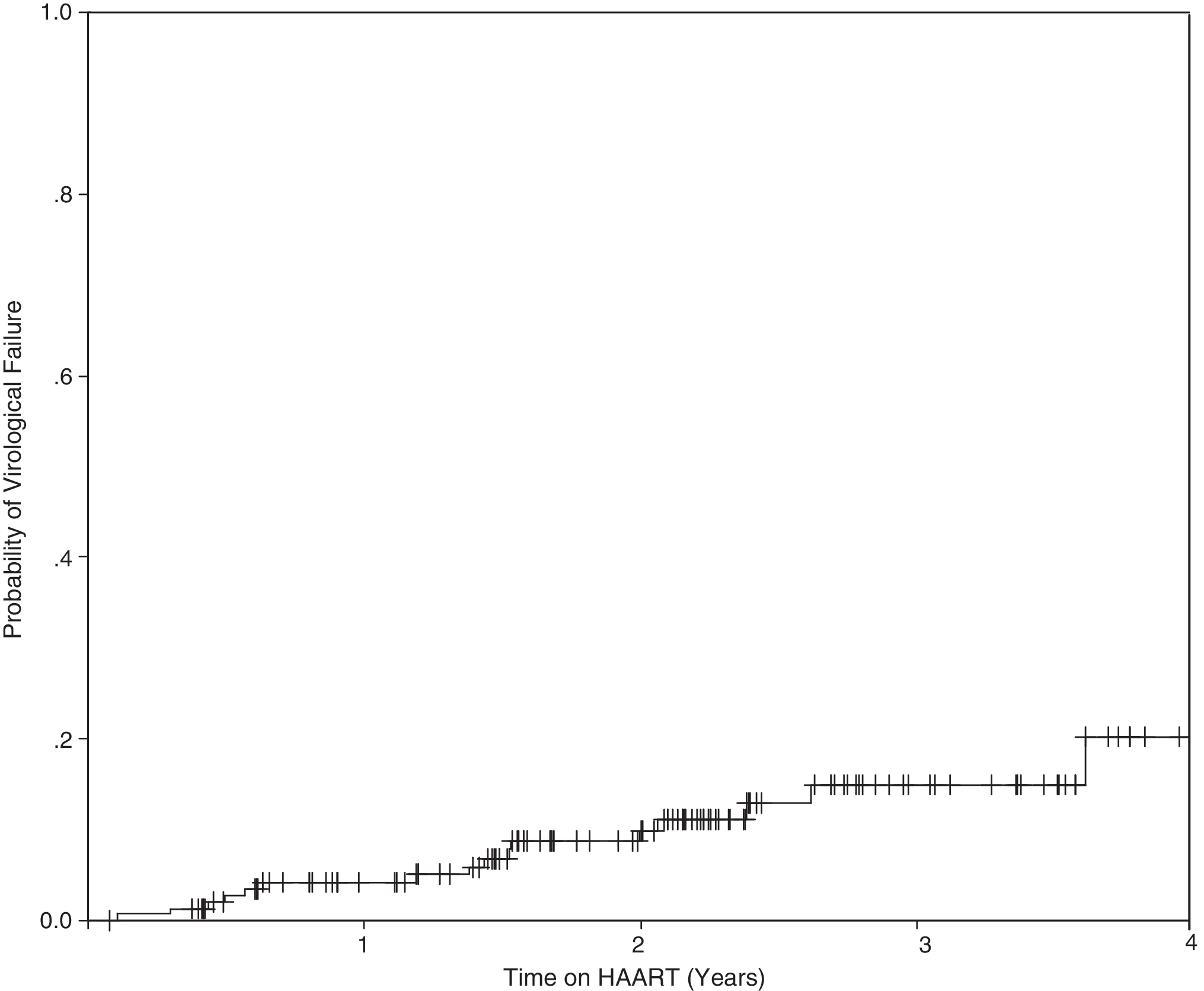
Probability of virological vailure (viral load >500 copies/ml after 6 months on HAART) by Kaplan–Meier analysis. Total of evaluable patients, n = 155. Patients with virological failure, n = 16 (10.3%), median of follow-up 20.6 months (6– 55 months).
VF, virological failure; VS, virological success.
Patients who voluntarily interrupt HAART one or more times.
Mortality
Five patients died during follow-up (mortality index of 0.046 per 1000 days/patient). The median of time to death was 2.9 months (1–34). The causes of death included sepsis (two patients), upper gastrointestinal hemorrhage associated with intestinal lymphoma (one patient), hepatic failure of unknown etiology (one patient), and unknown in one case. When the risk factors for death were analyzed, only starting therapy at an older age was associated with death compared to those who did not (45 vs. 34 years; p = 0.034). Baseline CD4+ count, HIV-1 viral load, having an AIDS-defining event, or developing VF, were not associated with death in our cohort.
Discussion
This is the first study evaluating outcomes among patients who started HAART through the recently created ARV government access program in Mexico. Our results show a very high retention rate and low frequency of virological failure and death in a well-characterized population of patients initiating therapy in Mexico. This population was composed mostly of men who had acquired HIV through homosexual contact and who presented with advanced HIV disease. Since the expansion of government programs for free access of HAART around the world, many reports have been published to show their effectiveness. 2 –7
In Mexico, the free ARV government program started in the year 2000 and became widely implemented throughout the country in 2003. At INCMNSZ, the program started in 2001. 8,13 Presentation with advanced disease, as defined as CD4+ counts lower than 200 cells/mm3 or the occurrence of an AIDS-defining illness, is a well known risk factor for early mortality and virologic failure among individuals initiating HAART. 14,15 The frequency of advanced disease in our population is similar or even higher than cohorts reported from low-income countries, even though Mexico is considered a middle-income country. 14,16 The trend we observed with a shift from boosted PIs to NNRTIs as the preferred third drug as part of the first HAART regimen has been observed in many other cohorts. 17
In our study, the use of NNRTI as the third ARV in the first HAART regimen was found to decrease the incidence of virological failure. Factors associated with virological failure were age below 30 years and poor medication adherence. Although women were more likely to be found in the population who developed virological failure this did not reach statistical significance. The index of mortality among our population study was very low compared to other cohorts of low- and middle-income countries, especially if we take into consideration the high prevalence of advanced disease at baseline in our patients. 16,18
Limitations of our study are the small size of the population analyzed, especially those who developed VF. Therefore, risk factors associated with VF during follow-up could be biased. The fact that the laboratory that did the viral load testing for most of the patients uses a cut-off of 75,000 copies/ml of HIV-1 RNA did not allow us to examine the influence that a viral load above or below 100,000 copies/ml had on virologic outcomes, a variable that has been found to be important in other studies.
The use of HAART has clearly demonstrated benefits in decreasing HIV-associated morbidity and mortality, even in areas with limited resources where programs for free access of HAART funded by international organizations such as the Global Fund or PEPFAR or funded by national governments have been implemented. The former programs have been demonstrated to be effective in a variety of settings including high-, middle-, and low-income countries. 14 Nevertheless, the implementation costs of these programs are very high and sustainability is still a concern. 19,20 The few studies that have tried to evaluate the effectiveness and outcomes of the ARV program in Mexico have questioned their effectiveness in the present health care system. 12
In this study we demonstrated that the use of HAART in a specialized health care setting in Mexico achieves high rates of effectiveness despite a high prevalence of advanced disease at baseline. 14,15 However, it is necessary to conduct similar evaluations in other settings in Mexico in which a large proportion of patients is receiving care for HIV in order to compare and understand the problems and needs of different settings. We believe, based on previous observations, 12,19 that quite possibly such evaluations would not show results as good as those found in this study. Currently there is an ongoing debate in Mexico as well as in other countries trying to decide if HIV care should occur at a primary care level of in specialized centers. Data from this study as well as future evaluations conducted at other health centers in the country caring for HIV/AIDS patients will be decisive in supporting or not supporting a move toward a more specialized based care for HIV/AIDS in Mexico.
Footnotes
Acknowledgments
We thank Rocío Velázquez Pastrana for data management. The study was supported in part by the NIH/AIDS International Training and Research Program of Emory University (D43 TW01042)
Author Disclosure Statement
B. Crabtree-Ramírez has a research grant from Merck and is a speaker for BMS. A. Villasis-Keever is a speaker for MSD, Pfizer, BMS, and Schering-Plough. Carlos del Río received grant support for his research from Merck and Co., Sanofi-Pasteur, the CDC, and the NIH. He has served as a consultant or member of the advisory committee for Merck, BMS, and Abbott. Juan G. Sierra Madero has received research grants from Pfizer, Merck, BMS, Abbott, Tibotec, Roche, and Boeringher Ingleheim. He is speaker for Merck, Pfizer, BMS, and Tibotec and has received advisory fees from Pfizer, Merck, and Stendahl.