
Abstract
There is limited information on the prevalence and pattern of HIV drug-resistant mutations (DRMs) among HIV-1-coinfected tuberculosis (TB) patients before and after antiretroviral treatment. Patients with HIV-1 and TB were recruited into a clinical trial from two different once-daily antiretroviral regimens and followed for a period of 6 months after ART initiation. Patients were treated with standard short-course anti-TB treatment (2EHRZ3/4RH3) and were randomized to receive ddI/3TC with either nevirapine or efavirenz, once daily. Genotypic drug resistance (DR) testing was carried out for the pol gene at baseline and at the time of virological failure. At baseline, major DRMs with respect to NNRTIs (G190GA) and TAMs (T215S and I) were observed in 3 out of 107 patients. Of 15 treatment failures, 14 had more than one major NRTI and NNRTI mutation. V106M was the major NNRTI mutation that emerged in EFZ and Y181C in the NVP group. Among NRTI mutations, M184V was the commonest followed by L74I/V. Primary drug resistance to antiretroviral drugs was low among HIV-1 co-infected TB patients in south India. A once-daily regimen of ddI/3TC/EFZ or NVP results in a specific pattern of NNRTI mutations and negligible thymidine analog mutations (TAMs).
The 3 by 5 initiative of the World Health Organization (WHO) rapidly increased access to antiretroviral (ARV) therapy in resource-limited settings worldwide. The National AIDS Control Program (NACO) of India initiated provision of free ARV therapy to human immunodeficiency virus (HIV)-infected patients in April 2004, scaling up rapidly to include >200,000 patients by May 2009. The WHO recommended first-line ARV regimen, provided under the program, contains two nucleoside reverse transcriptase inhibitors (NRTIs): stavudine (d4T) or zidovudine (ZDV) with lamivudine (3TC), and one nonnucleoside reverse transcriptase inhibitor (NNRTI): nevirapine (NVP) or efavirenz (EFZ). Most patients are initiated on a generic three-drug fixed dose combinations containing NVP while EFZ is reserved for patients with intolerance or other contraindications to NVP use as well as those with tuberculosis. 1 The success of therapy depends on susceptibility of the virus to drugs used as well as adherence to ARV therapy. A high adherence rate (>95%) is required to prevent the emergence of HIV drug resistance. Most infections in India are caused by subtype C, while the other subtypes B, A, and recombinant forms account for <2% of infections. 2 –4
Drug resistance (DR) is a major limitation to antiretroviral treatment (ART), therefore DR testing is increasingly important for clinical management. The presence of DR before starting a new treatment regimen is an independent predictor of virological response to that regimen. 5 Situations in which ARV drugs are used in the private sector in an inappropriate manner favor the emergence of drug-resistant viruses and represent an obstacle to the long-term effectiveness of ART. Drug resistance surveillance (DRS) is useful to obtain an estimate of the transmission and circulation of resistant viral mutants among untreated patients. 6 Tuberculosis (TB), the commonest infection occurring in HIV-infected patients in most countries in Asia and Africa, is responsible for a substantial proportion of HIV-associated morbidity and mortality. 7 In India and many countries of sub-Saharan Africa, HIV-coinfected TB patients form a substantial part of the patients referred for ART. 8 There are a few reports describing the prevalence of HIV drug resistance mutations (DRMs) among ART-naive 2,3,9,10 and ART-experienced 11,12 HIV-1-infected persons in India but none in a prospective cohort followed after initiation of ART among ART-naive patients with TB as well as the pattern of mutations developing during the simultaneous treatment of both infections.
Our aim was to study the prevalence of HIV DR mutations in a group of ART-naive HIV-1-infected TB patients in south India initiating ART and follow them up prospectively for development of new mutations. Patients were enrolled in a randomized clinical trial at the Tuberculosis Research Centre (TRC), Chennai to evaluate the safety and efficacy of two different ART regimens along with antituberculosis treatment (ATT) (NCT No. NCT00332306). The first 107 patients screened for recruitment to this trial were studied to determine the prevalence of DR mutations among ARV-naive patients in this region. Further, we compared the pattern of mutations emerging in patients failing an NVP-based versus and EFZ-based regimen with the same NRTI backbone. This population of HIV-1-infected TB patients studied by us is unique, both in terms of the impact of active TB on HIV replication, diversity, and DR as well as the impact of ART when given concomitantly with ATT, in terms of efficacy.
Patients referred to the TRC clinics at Chennai, Madurai, and Vellore with symptoms suggestive of HIV and/or tuberculosis were counseled about the study procedures, informed consent was obtained, and HIV testing was done in addition to the investigations for TB. Patients who were >18 years of age with newly diagnosed pulmonary or extrapulmonary TB with HIV-1 infection and CD4 count <250 cells/mm3 and who fulfilled other eligibility criteria were recruited to the study. Patients with a previous history of ATT or ART, pregnant and lactating women, patients with HIV-2 infection, and those with major complications of HIV disease were excluded. Patients with newly diagnosed TB and HIV were randomized to start either regimen (ddI +3TC + NVP or ddI + 3TC + EFZ) at the end of the intensive phase (2 months) of ATT. The anti-TB regimen used was the standard intermittent three times weekly 6-month regimen (2EHRZ3/4RH3) used in the Revised National TB Control Program of India. Patients were given treatment under direct observation three times a week and were reviewed every month. The primary outcome was death or a detectable viral load (>400 copies/ml) at 6 months of ART.
CD4 count and viral load were measured at baseline (BL), at initiation of ART, and again after 1, 4, and 6 months of treatment. Plasma was separated within 6 h of collection and stored at −80°C in aliquots until further processing. CD4 lymphocytes were counted with a FACS Count Flow cytometer (BD Biosciences, San Jose, CA), and viral load was measured using the COBAS Amplicor HIV-1 monitor, version 1.5 (Roche Diagnostics, Indianapolis, IN).
DR testing was performed using an in-house method published earlier.
2
The extraction of viral RNA was done with a QIAamp viral RNA mini kit (Qiagen, Valencia, CA). Reverse transcription and amplification of the RNA were done for the reverse transcriptase (RT) and protease (PR) genes using the primer sets listed in Table 1. The amplified products were purified by the 80% isopropanol method and were sequenced on both strands with the Big Dye Terminator sequencing kit and an automated sequencer (3100-Avant Genetic analyzer; Applied Biosystems). The derived nucleotide sequences were aligned using Seqscape software version 2.5 with known reference strains of M and N pooled from the HIV-1 gene databank (
Sequences of the Consensus Primers Used for the Amplification of RT and Protease
One hundred and seven HIV-1-coinfected TB patients who were screened for recruitment to the clinical trial were included in this substudy and DR testing was done at the baseline time point. The demographic details of the study participants are provided in Table 2. The fate of patients admitted to the study and followed up for a period of 6 months after ART initiation including deaths and defaulters as well as the patients excluded from the study are described in Fig. 1.

Fate of patients screened and recruited to the trial.
Baseline Demographic Characteristics of Study Population
Phylogenetic trees (not shown here) for the HIV-1 polymerase (RT and PR) gene confirmed that the majority of the isolates were clustered within subtype C with the exception of one, which belonged to subtype A1. Few sequences in the PR and RT regions of the patients were found clustered near subtype B in either of the genes, suggesting the presence of BC recombinants.
Sequences for RT and PR were successfully obtained from 104 and 99 patients at baseline, respectively. The polymorphisms observed in the RT and PR region among the ARV-naive patients are summarized in Table 3. In the RT region, more than 50% of the sequences exhibited amino acid substitutions at one or more of the codons 35, 36, 39, 48, 60, 121,135, 162, 173, 177, 200, 207, 211, 214, and 245. Major DR mutations with respect to NNRTIs (G190GA) and TAMs (T215S and I) were observed in three patients at baseline. One patient showed a V108I mutation, which is associated with possible resistance to NNRTI. Of these four ART-naive patients with DR mutations, one was not recruited to the trial, two when followed up to 6 months did not develop virological failure, and one patient developed failure at month 6 of treatment.
Amino Acid Substitutions in the RT (Top) and PR (Bottom) Genes at Baseline a
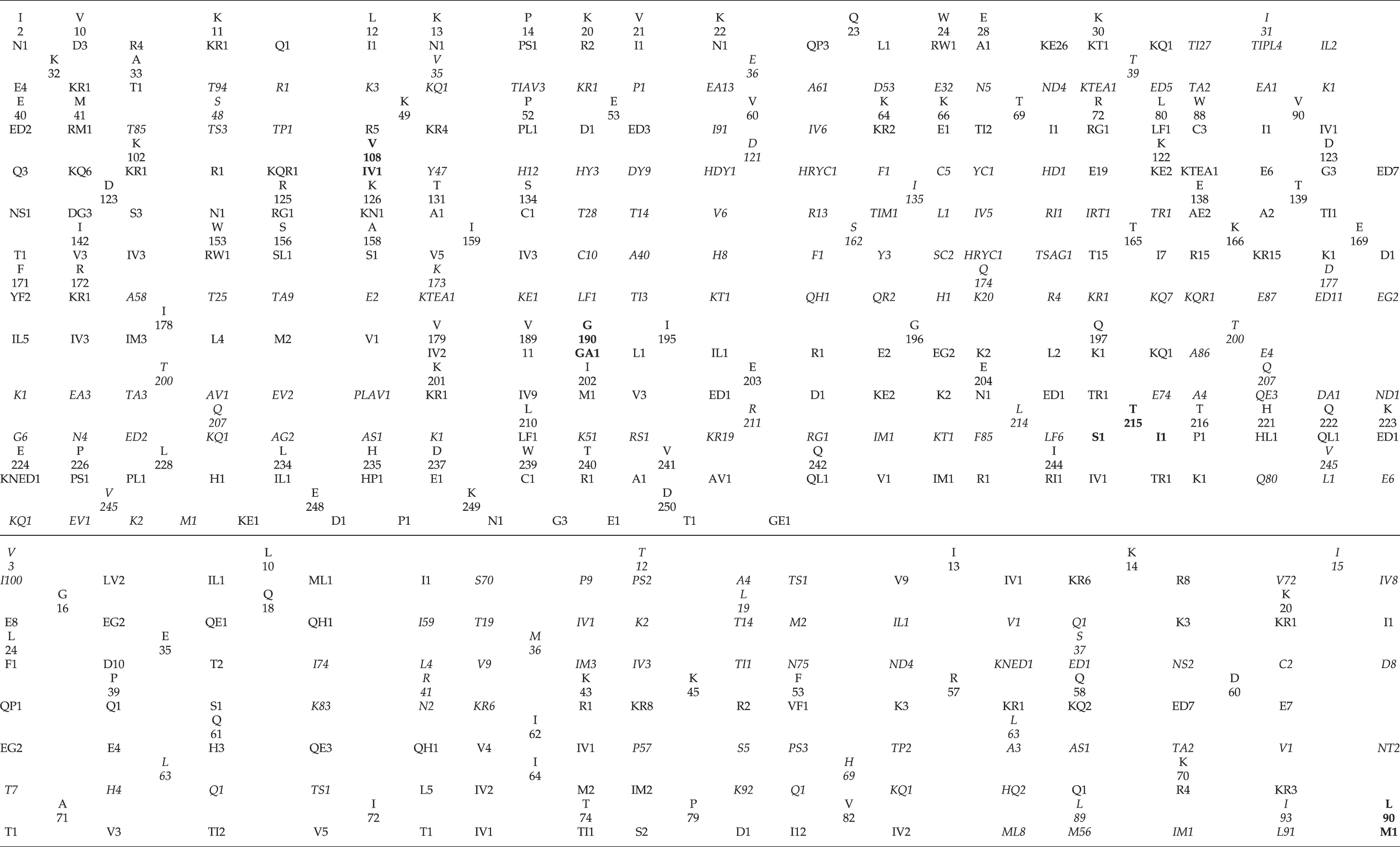
The columns in italics are significant polymorphisms at positions of potential resistance to subtype B observed more frequently. The columns in bold are the major drug-resistant positions.
With respect to the PR gene, 50% of the sequences showed polymorphisms at codons 12, 19, 41, 89, and 93. Substitutions at secondary mutation positions were frequently observed at codons 3, 12, 15, 19, 36, 37, 41, 63, 69, 89, and 93 with 100% of substitution at codon 3. One patient with an unknown previous treatment history had the L90M mutation.
Of the 87 patients admitted to the study and followed up for a period of 6 months, 18 developed virological failure. Out of the 18 virological failures (5 in the EFZ arm and 13 in the NVP arm), DR patterns were available for 15. None of these patients had a major PR mutation. With respect to the RT gene, all except one had more than one major DR mutation conferring resistance to NRTI and NNRTIs (Table 4). On comparing the pattern of emerging DR mutations with respect to the RT inhibitors, Y181C was the major NNRTI mutation seen in the NVP failures while V106M was observed among EFZ failures.
Mutations in the RT Gene at the Time of Virological Failure
Sequencing was possible in 12 and 3 patients in the NVP and EFZ regimens, respectively: 14 patients had one or more DR mutations.
In our cohort of HIV-1-coinfected TB patients, the prevalence of baseline DRMs was found to be low. Of the 107 patients three had viruses with resistance to NRTI or NNRTI while one had a mutation (V108I) that is associated with possible resistance to NNRTI. According to the WHO ResNet criteria, the presence of less than 5% of a transmitted DR mutation in a population is indicative of low prevalence. We calculated the calibrated population resistance (CPR) using the tool in the HIV Stanford Drug resistance database for our sequences. The CPR was 0.1% each for the PR, NNRTI, and NRTI mutations. A borderline or suspicious mutation prevalence of 0.3% was found in the RT gene (CPR Reference No. 16542_1227078407). It is evident from these ratios that the rate of transmission of viruses with resistance to drugs used in the first-line regimen is relatively low in the south Indian population. These findings are in agreement with previous studies from India among ART-naive adults and with our own observations in children. 2,3,9,10 Reports of high rates of transmitted drug resistance in the United States (10%) and Europe (19.2%) indicate the necessity of continued surveillance among populations exposed to ARV drugs. 13,14
One of the regimens used in this study, ddI/3TC/EFV, is widely used in South Africa for patients with TB and HIV infection 15 and in this trial we used it as the control regimen to study a new once-daily regimen of ddI/3TC/NVP. Data were collected on virological and immunological response to treatment as well as adherence and blood levels of the NNRTIs, which we could correlate with treatment failure and development of drug resistance. A sequencing profile of the RT and the PR gene was available for 15 of the 18 subjects who had virological failure. There were no major mutations observed in the PR gene in any of the virological failures. In the RT gene more than one resistant mutation was observed against both NRTI and NNRTIs in 14 subjects. Only one patient did not demonstrate any mutation in spite of a high viral load. We repeated the sequencing of the RT gene twice and also analyzed the proviral DNA from this patient for the presence of any latent mutant virus, but no mutation was observed even in the proviral DNA. This patient had stopped ART completely for about 40 days before the final assessment, due to psychosocial problems. Hence, the absence of detectable mutations probably reflected the complete lack of ARV drugs in the recent past, leading to replication of the wild-type virus.
The results of the clinical trial and efficacy of the ARV regimens are being reported separately. In this substudy, we compared the type of mutations developing in patients randomized to the two regimens. The presence of V106M was observed in all the EFZ-treated failure patients while Y181C was the major mutation in the NVP-treated patients. The Y181C mutation is selected by the NRTI nevirapine and confers high-level resistance to this drug with low-level resistance to efavirenz, 16 but there are reports stating that the Y181C resistance mutation may be selected, not only by NNRTIs, but also by d4T. This may be of particular significance in developing countries where treatment with Triomune, a fixed combination of d4T, 3TC, and NVP, is common. 17
The V106M mutation, potentially conferring cross-resistance to all NNRTIs and usually associated with EFZ treatment, was observed in all patients who failed with an EFZ-containing regimen. The presence of the V106M is in concordance with an earlier study that observed that resistance to EFZ in clade C viruses can develop in vitro due to a natural GTG polymorphism at codon 106 that is distinct from the NVP-associated mutation at position 106 (i.e., V106A) commonly seen in clade B viruses. 18 Physicians should be aware of the V106M mutation and its potential impact on virological responsiveness. Other than these two NNRTI mutations, we also observed the presence of G190A and K103N in some failure patients. However, K103N was not the commonest NNRTI mutation emerging, a fact relatively underappreciated by physicians.
With respect to the NRTI mutations, M184V was observed in almost all the patients failing therapy followed by the L74I/V mutation, conferring high-level resistance to 3TC and ddI, respectively. A recent report from South Africa found mutations to NRTI and NNRTIs, especially V106M and TAMs, observed in patients failing first-line or second-line drug regimens similar to ours. Unlike their study, however, the rate of TAMs emerging was very low in our population. Furthermore, we had only one K65R emerging after treatment. These findings have implications for second-line treatment in resource-poor countries. To preserve NRTIs such as zidovudine for use with boosted protease inhibitors, one option is to use ddI/3TC or FTC in the first-line regimen. Apart from the advantage of once-daily usage, the low emergence of TAMs would help preserve more NRTI options for later use.
The strengths of our study are the prospective nature of the cohort, randomization to the two different ARV regimens being compared, and good adherence and follow-up. Our study is also unique in that we included patients with active TB, high viral loads, and severe immunosuppression. This population is likely to have very high viral diversity and possibly more natural mutations. The relatively small number of patients with virological failure is the limitation. A larger cohort needs to be studied to look at the various mutations and the response of these patients to second-line regimens.
Our findings also confirm that the most prevalent HIV-1 subtype in south India is subtype C. The majority of the sequences clustered with subtype C strains of Indian origin and one with subtype A1, while a few sequences clustered with B and C in the RT and PR genes. These could be recombinants that need to be confirmed by sequencing the envelope gene. This is the first report of a subtype A1 HIV-1 strain in the south Indian population, though subtypes A and BC recombinants have been reported in the north Indian population. 2 –4
Our findings have implications for treatment of HIV-infected patients in India and other developing countries. In summary, we have found a low baseline prevalence of drug resistance mutations to NRTIs and NNRTIs among HIV-infected TB patients in south India. The emergence of the Y181C mutation after nevirapine treatment and its implications regarding resistance to other drugs in its class need further study. We have added to the knowledge on the many polymorphisms in the RT and PR gene observed in the Indian clade C virus. Finally, we observed a low rate of emergence of TAMs in this population treated with a ddI/3TC backbone.
Accession Numbers
The pol gene sequences of HIV-1 isolates have been deposited in GenBank with the following accession numbers: FJ59245–FJ59475.
Footnotes
Acknowledgments
The authors are thankful to the doctors, nurses, health visitors, and laboratory staff of the Department of Clinical Research at the Tuberculosis Research Centre (Chennai, India) for their help in patient management and for their constant support. The authors owe their thanks to Dr. V. Kumaraswami, Scientist ‘F’ and Officer In-Charge, Tuberculosis Research Centre for his encouragement and support throughout this study. The authors thank the International Centre for Excellence Research (ICER) for its award of a Senior Research Fellowship to Ms. Lakshmi. We acknowledge Prof. Herve. J. Fleury, University Victor Segalan, Bordeaux, France for his generous support in providing the training for drug resistance testing and his time. The authors thank all the trial participants. Ms. Rajesh Lakshmi, M.Sc., performed the laboratory procedures, data analysis, and interpretation and drafted the manuscript. Mr. Karunaianantham Ramesh, M.Sc., assisted with the laboratory procedures. Dr. Paranji R Narayanan, Ph.D., supervised and guided the overall conduct of the study. Dr. Soumya Swaminathan conceived the study and participated in data interpretation and critical revision of the manuscript.
Disclosure Statement
No competing financial interests exist.