
Abstract
Current laboratory methods to detect recent HIV-1 infection for the estimation of incidence have various limitations, including varying performance in different subtypes or populations. Therefore, new methods are needed to detect recent infections with increased specificity. We developed a recombinant protein, rIDR-M, that covered divergent sequences from the immunodominant region (IDR) of gp41 from all major subtypes and recombinants of HIV-1 group M and expressed in Escherichia coli. The rIDR-M protein was highly reactive with HIV antibodies in sera from different subtypes and equivalently detected antibodies to divergent subtypes B and AE from Thailand, in contrast to individual gp41 peptides derived from respective subtypes, suggesting that it can be used for incidence assays. The protein was used in two different assay formats to measure antibody avidity: (1) a two-well avidity index assay (AI-EIA) and (2) a new one-well limiting antigen avidity assay (LAg-avidity EIA), both with a pH 3.0 buffer to dissociate low-avidity antibodies present during early infection. Limiting the amount of antigen allowed detection of recent HIV-1 infection, with or without dissociation buffer, but the detection was most efficient when the pH 3.0 dissociation buffer was included. When a well-characterized 41-member seroincidence panel (20 recent and 21 long-term) was used, both the two-well AI-EIA and one-well LAg-avidity EIA efficiently distinguished recent and long-term infections. The new avidity-based assays using rIDR-M antigen may improve the accuracy of detecting recent HIV-1 infection and allow a better estimation of incidence in diverse HIV-1 subtypes.
Introduction
A
In 1998, Janssen et al. 13 described the development of a modified, less-sensitive enzyme immunoassay, 3A11-LS EIA, for detecting recent HIV seroconversion. After the 3A11 assay was discontinued by the manufacturer, another commercial assay (Vironostika-EIA) was modified to develop the Vironostika-LS EIA. 14 The simple modifications of the commercial assays allowed detection of recent seroconverters from long-standing infections permitting the estimation of incidence in cross-sectional populations. 19 –23 The LS-EIAs indirectly measure the relative HIV antibody titers that are low in persons with early infections but are high in persons with long-standing infections. When these methods were further applied in divergent subtypes, the duration of recency (or window period) varied substantially. 24,25 Subsequently, we and others investigated several different approaches 5,10 for detecting recent HIV-1 infections. In 2002, we reported the development of the BED-capture EIA, which used a synthetic antigen containing sequences from multiple subtypes and a simple capture format to allow the measurement of an increasing proportion of HIV antibodies following seroconversion. 8 The assay is now commercially available and has been used in several studies. 17,26 –32 Recent studies indicated that approximately 5–6% of HIV-1-infected people with >1 year of infection were misclassified by the BED assay; accordingly posttest adjustments have been proposed to improve the accuracy of incidence estimates. 33,34
Several different approaches for detecting recent infections have been described, including detection of antigen-specific antibodies, 5,15 detection of the IgG3 isotype to p24, 12 modification of simple and rapid tests, 3,4,6,16 and antibody avidity. 7,35 None of the assays has been adequately evaluated in longitudinal seroconverter specimens or in cross-sectional populations to assess their usefulness. However, recent data suggest that most methods overestimate HIV-1 incidence, especially in African populations. 36 This overestimation could result from HIV-1 subtype variability, population differences, or high levels of total IgG in African population (B.S. Parekh, unpublished data). Other factors, such as long-term antiretroviral therapy or coinfections with other pathogens such as malaria or tuberculosis (TB), could also affect the performance of the incidence assays.
In our continued efforts to develop better laboratory methods to detect recent HIV-1 infection, we describe here the development of a multisubtype gp41 recombinant antigen and its application in two avidity-based assays. The avidity index assay was developed by using a traditional two-well approach and the new one-well avidity assay was developed by using limiting amounts of the antigen.
Materials and Methods
Design and development of recombinant protein, rIDR-M
A review of the Los Alamos HIV sequence database indicated that there are three major variants of gp41 immunodominant regions among the HIV-1 group M viruses, especially the core amino acid sequence from DQ–CT (Fig. 1A). The first sequence was most common among subtypes A, B, C, F, G, H, J, and K and recombinants AG, AB, AC, BF, and BG. 37 The second sequence was most common only in subtype AE from Thailand, and the third sequence was most common among subtypes D and recombinant AD. The recombinant protein was designed to include all three variant sequences. A set of nucleotide primers (Table 1) was synthesized and used to amplify, in multiple steps, the complete double-stranded DNA sequence for rIDR-M coding sequences. RNA, extracted from representative HIV-1 subtype culture supernatants, was used to amplify the regions of interest using the three sets of gp41 primers (Table 1A). Two intervening hydrophilic sequences were inserted using the primers shown in Table 1B. The sequences were engineered in the expression vector pQE80L (QIAgen, Valencia, CA), with an added His tag (6-mer) to the N-terminal end of the recombinant protein to facilitate affinity purification of rIDR-M. Three gp41 sequences (shown in bold) were separated by hydrophilic sequences with charged amino acids (underlined) to increase the yield and solubility of rIDR-M (Fig. 1A). The protein was expressed in codon-optimized Escherichia coli BL21-CodonPlus DE3-RP (Stratagene, La Jolla, CA). The E. coli cells were lysed in 6 M guanidine hydrochloride (GuHCl) with intermittent sonication over ice and purified by using an Ni-NTA affinity column (QIAgen, Valencia, CA). The bound protein was eluted at pH 3.5 (Fig. 1B). Purified protein was dialyzed against 0.1 trifluoroacetic acid, lyophilized, dissolved in dimethyl sulfoxide at a concentration of 5 mg/ml, and stored at −70°C until use.
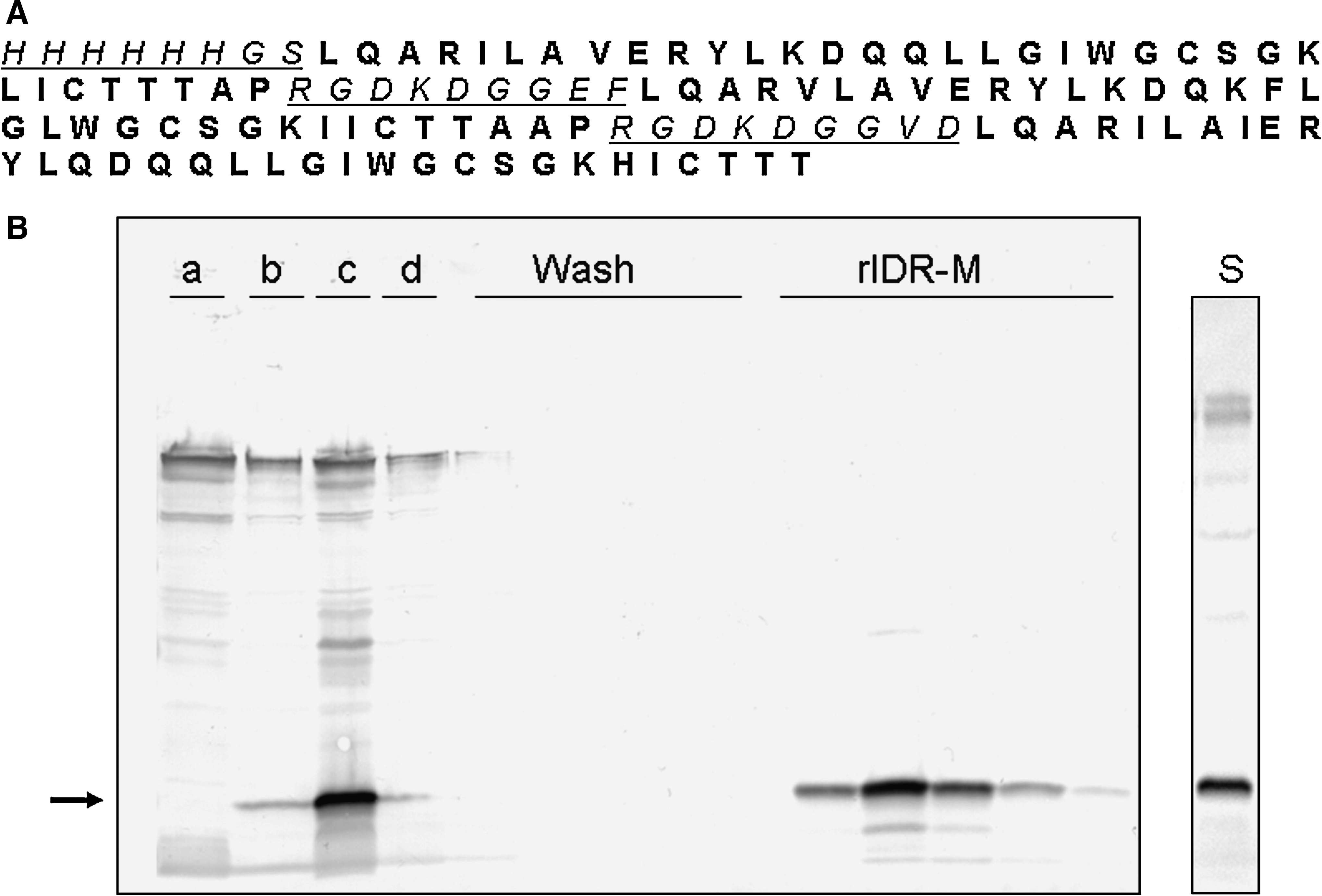
Amino acid sequence of rIDR-M protein (
F, forward; R, reverse.
Serum specimens
An HIV-1-positive plasma specimen (J19) purchased from a commercial source (Boston Biomedica Inc., Waldham, MA) was used to perform the Western blot and to monitor the purification of rIDR-M. Serum specimens from 12 Thai subjects known to be infected with the HIV-1 subtype B (n = 6) and subtype AE (n = 6) viruses were used to evaluate subtype bias of gp41-B peptide, gp41-AE peptide, or rIDR-M protein. The specimens were from known incident infections collected about 1 year after infections and were part of serial specimens collected from a longitudinal cohort study of injecting drug users in Bangkok conducted between 1995 and 1998 as part of a joint collaboration between the U.S. Centers for Diseases Control and Prevention (CDC) and the Bangkok Metropolitan Administration. 38 In addition, 580 HIV-seropositive specimens (573 HIV-1 and 7 HIV-2), collected from different countries, were used to assess immunologic reactivity of the recombinant protein. The specimens are part of the well-characterized specimen panel collected for HIV test evaluation in our laboratory at the CDC in Atlanta, Georgia. The specimens were from Cameroon (n = 41), South Africa (n = 159), Kenya (n = 64), Ivory Coast (n = 130), Thailand (n = 132), Uganda (n = 20), and the United States (n = 34). Their HIV status was confirmed by the FDA approved EIA (Genetic Systems HIV-1-2-O EIA) and Cambridge Biotech HIV-1 Western blot (Maxim Biotech, Rockville, MD) testing algorithm. Suspected HIV-2 specimens were further tested with the Multi-spot HIV-1/HIV-2 rapid test (Bio-Rad Laboratories, Hercules, CA).
Initial optimization of the incidence assay conditions (see below) was performed using a small panel, termed BBI-5 [two recent (<6 months), three long-term (>1 year)], from a commercial source (Boston Biomedica Inc., Waltham, MA). The serum specimens were from different individual donors. Subsequently, a 41-member seroincidence (SI) panel (21 long-term infections and 20 recent infections) was used for further evaluation. Twenty specimens from recently infected individuals were chosen from multiple seroconversion panels (Boston Biomedica Inc.). Additional details about this panel have been described earlier. 5
Enzyme immunoassays (EIA)
To assess the immunologic reactivity of the rIDR-M protein, Immulon II microwell plates (Dynex, Chantilly, VA) were coated with 2.5 μg/ml of rIDR-M in 0.1 phosphate buffer saline, pH 7.4 (phosphate-buffered saline, PBS) by overnight incubation. Plates were washed with PBS containing 0.1% Tween-20 (PBS-Tween) and blocked with 5% nonfat dry milk powder in PBS-Tween (milk buffer). Plates were washed again, covered with a sealer, and stored frozen with desiccant in Ziplock bags at −30°C until use. The regular EIA protocol included the following steps. A 100-μl aliquot of diluted specimen (1/400 in milk buffer) was added to appropriate wells and incubated for 1 h at 37°C. The plate was then washed four times with 300 μl/well of PBS-Tween. One hundred microliters of goat-antihuman IgG peroxidase, diluted 1:5000 in milk buffer (BioSource, Mountain View, CA), was added and incubated at 37°C for 30 min, followed by four washes with 300 μl/well of PBS-Tween. One hundred microliters of tetramethyl benzidine (TMB) was added and incubated at 25°C for 15 min. The color development was stopped by the addition of 100 μl of 1 N H2SO4 to each well and the optical density (OD) was read at 450 nm.
Avidity index assay (AI-EIA)
Two-well avidity index assays were performed using plates coated with 2.5 μg or 1.25 μg/ml of rIDR-M protein. Each diluted specimen was added to the two wells. Following the first incubation to allow binding of HIV antibodies, one well (treated) was incubated with pH 3.0 buffer (dissociation buffer) while the second well (control) was incubated with wash buffer at 37°C for 15 min. Following the wash, the remaining steps were the same as described earlier. The avidity index was calculated as a ratio of OD of the treated well divided by the OD of the control well, expressed as a percent. The final avidity index of a specimen was calculated as an average of two separate measurements on two distinct runs.
Limiting antigen avidity EIA (LAg-avidity EIA)
For optimization experiments, varying amounts of rIDR-M (2.5–0.08 μg/ml) were coated onto microwells of 96-well plates. The specimens were diluted 1/100 in milk buffer. Subsequent incubation and wash steps were essentially the same as the regular EIA (control, no treatment) or with one additional step that included a 15-min incubation with a dissociating reagent (4 M urea or 0.1 M citrate buffer, pH 3.0) following specimen incubation. As an additional control experiment, we also included a set with 15-min incubation with PBS following specimen incubation. Subsequent experiments were conducted by using the best combination of conditions, which included rIDR-M coating at 0.62 μg/ml and a dissociation step with pH 3.0 citrate buffer. The optical density values were used directly to observe the separation of recent and long-term infections. This single well assay was run in triplicate and average values were used for comparison purposes.
Results
Recombinant protein, rIDR-M
The rIDR-M protein (molecular weight 15 kDa) was purified by using an Ni-NTA affinity column and dissociating the bound protein with a low pH 3.5 buffer. The fractions were monitored by Western blotting by using an HIV reactive specimen (Fig. 1B). The protein had a high purity of >90% as observed by staining the gel (Fig. 1B lane S). Trace amount of contaminating proteins with high molecular weight did not react on Western blot suggesting that they were E. coli proteins copurifying with the rIDR-M. The rIDR-M protein was purified consistently from multiple lots with a yield of about 5 mg/liter of E. coli culture.
To ensure that the purified protein was immunologically reactive and that it could be used for the development of the HIV-1 incidence assays, we tested 573 HIV-1 specimens from different geographic regions with standard EIA (antigen coating at 2.5 μg/ml). Five hundred and fifty-eight (97.2%) of 573 HIV-1-positive specimens had strongly reactive antibodies in rIDR-M EIA (mean OD = 3.523, standard deviation = 0.916). A total of 15 specimens (2.8%) did not react with rIDR-M EIA; all had partial and/or weak Western blot banding pattern, often with no gp41 band, suggesting recent HIV-1 infections (not shown). All 15 specimens were classified as recent HIV-1 infections by the BED assay 8 (not shown) suggesting they have low or no antibodies to gp41. Seven HIV-2 specimens were nonreactive with rIDR-M. This finding was expected because the protein was derived from the immunodominant region of HIV-1 gp41, a region often used to distinguish HIV-1 and HIV-2.
In addition, to demonstrate the equivalent detection of different subtype antibodies by rIDR-M, we tested 12 specimens from individuals infected with Thai subtype B (n = 6) or AE (n = 6) to determine their end-point titer on rIDR-M EIA (Fig. 2). For comparison, end-point titers on gp41-B peptide or gp41-AE peptide are also shown for the same specimens, which were taken approximately 1 year following seroconversion. 8 Our results demonstrate that antibody titers were higher in subtype B sera than in AE sera when gp41-B peptide was used as the antigen. Conversely, antibody titers were higher in AE sera than in B sera when gp41-AE peptide was used as the antigen. Therefore, neither the B-specific nor AE-specific gp41-peptide is sufficient to equivalently detect antibodies in B or AE-infected individuals. However, rIDR-M protein detected antibodies equivalently in both B and AE-infected individuals because the divergent subtype sequences were included in this protein (right panel). This suggests that the protein should work well for antibody-based incidence assays, which are typically quantitative in nature and should quantify antibody-based parameters equivalently in different subtypes.
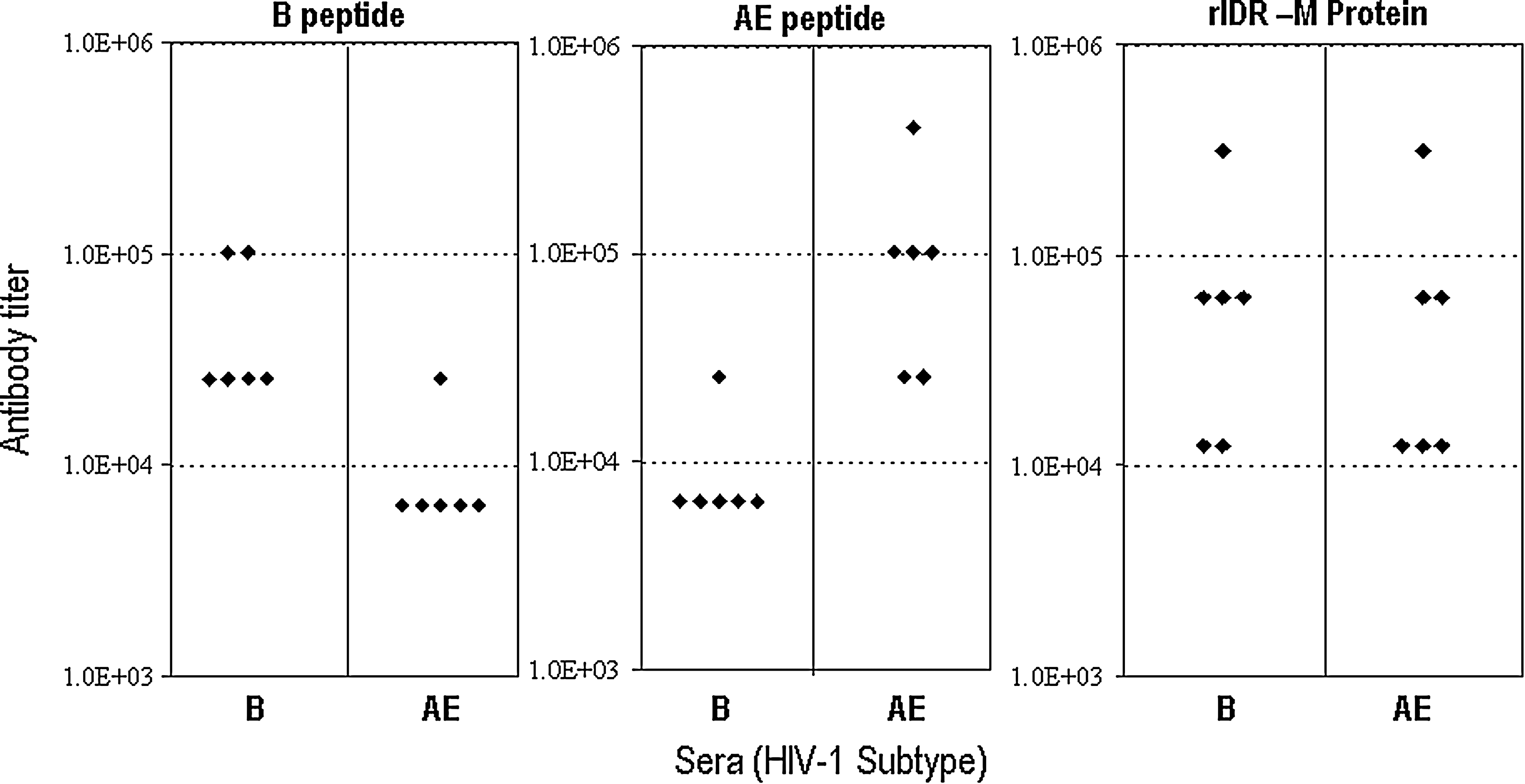
End-point titers of HIV antibodies in sera from six subtypes B and six subtypes AE-infected individuals from Thailand collected 1 year after infection. Antigens used were gp41-B peptide (left panel), gp41-AE peptide (middle panel), or rIDR-M protein (right panel).
Avidity index EIA (AI-EIA) and limiting antigen avidity EIA (LAg-avidity EIA)
The principles behind the traditional avidity index assay and limiting antigen avidity assay are shown schematically in Fig. 3 (left and right panels, respectively). The traditional avidity index assay (left panel) uses two wells; one is treated with a dissociation reagent while the second one is untreated and is used as a control well. The avidity index is then calculated by using the formula shown. We used 0.1 M citrate buffer at pH 3.0 to dissociate the low-avidity antibodies. Low pH buffer is routinely used to aid in the elution and purification of antibodies. 39 The same strategy can be exploited to dissociate low-avidity antibodies.

Schematic representation of principles underlying two-well avidity index EIA (left panel) and one-well limiting antigen EIA (right panel).
The one-well limiting antigen avidity assay is based on the following principle (Fig. 3, right panel). At high concentrations of antigen, both high- and low-avidity antibodies can bind and the binding can occur with both binding sites because of the high density of antigen. Lowering the coating concentration of antigen should permit binding of only high-avidity antibodies. Moreover, because the antigen is not available to bind both binding sites simultaneously low-avidity antibodies will not be able to bind strongly to wells with low antigen density. Therefore, this approach may be able to differentiate recent and long-term infections based on antibody avidity, with or without dissociation treatment.
LAg-avidity EIA with or without dissociation reagents
Using a well-characterized panel of five specimens (two recent, three long-term), we tested the effect of gradually lowering the amount of antigen coated on the wells, with or without any dissociation treatment (Fig. 4). As shown in Fig. 4A, we could not discriminate between recent and long-term infections at saturating concentration (2.5 μg/ml) of antigen. However, as the antigen amount was lowered on the microwell plate, there was progressive discrimination of recent and long-term infections and the most effective separation was achieved at 0.16 μg/ml of antigen coating without any dissociating reagent. The results were similar with PBS control, in which PBS was used for treatment instead of the dissociating reagent (Fig. 4B). When 4 M urea was used as a dissociation step (Fig. 4C), there was some reduction of binding of antibodies from recently infected individuals, but the effect was not substantial. However, when pH 3.0 buffer was used to dissociate low-avidity antibodies at varying antigen levels, the effect was substantial; separation between the recent and long-term infected individuals was most efficient at 0.62 μg/ml of antigen (Fig. 4D).
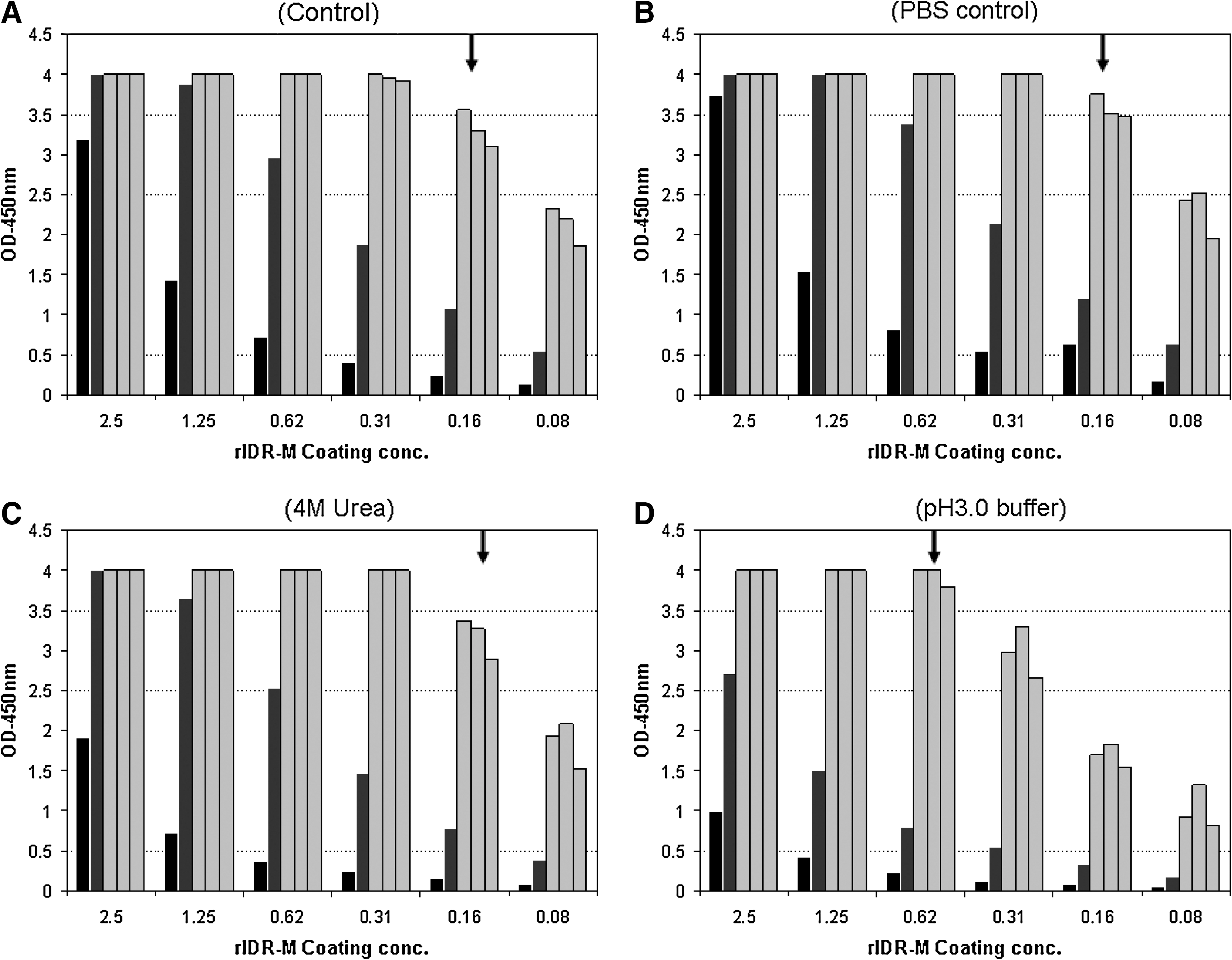
Detection of recent HIV-1 seroconversion using a known panel of five specimens (two recent, solid bars, and three long-term, gray bars) in an EIA format. Different treatments and varying concentrations of rIDR-M, as indicated, were used to coat the microwell plates. (
We compared the best conditions, with or without various treatments, to each other and to the results obtained by the BED assay for these five specimens (Fig. 5). In addition, we also include results from the two-well avidity index assay performed using the rIDR-M antigen and pH 3.0 dissociation buffer for comparative purposes (right panel). These results show that the avidity-based assays can be used in multiple ways to distinguish recent from long-term infections. The limiting antigen avidity EIA at 0.62 μg/ml, with pH 3.0 dissociation buffer, resulted in the best separation of recent and long-term infections.

Comparison of optimal EIA conditions with varying treatments using rIDR-M antigen at indicated concentrations as shown. For comparison purposes, the results of the BED-capture EIA and the two-well avidity index assay (right panel) are also shown. The same panel of five specimens (two recent, solid bars, and three long-term, gray bars) was used as in Fig. 4. The best condition (0.62 μg/ml with pH 3.0 dissociation buffer) is indicated by an arrow.
Comparison of two-well AI-EIA and one-well LAg avidity EIA
We subsequently used the SI panel consisting of 41 specimens (20 recent and 21 long-term infections) to evaluate the performance of two-well AI-EIA and one-well LAg-avidity EIA. This panel was used earlier in our previous study to assess the performance of 16 different approaches. 5 Results of two-well AI-EIA at antigen concentrations of 2.5 μg/ml and 1.25 μg/ml are shown in Fig. 6A and B, respectively, and demonstrate effective separation of the two groups. Results of one-well LAg-avidity EIA, which were conducted at antigen concentration of 1.25 μg/ml and 0.62 μg/ml, are shown in Fig. 7A and B, respectively. Recent and long-term infections of the SI panel can be distinguished effectively at both concentrations of antigen, although the cutoff would be lower at a lower concentration of rIDR-M.

Two-well avidity index assay using rIDR-M-coated wells at 2.5 μg/ml (
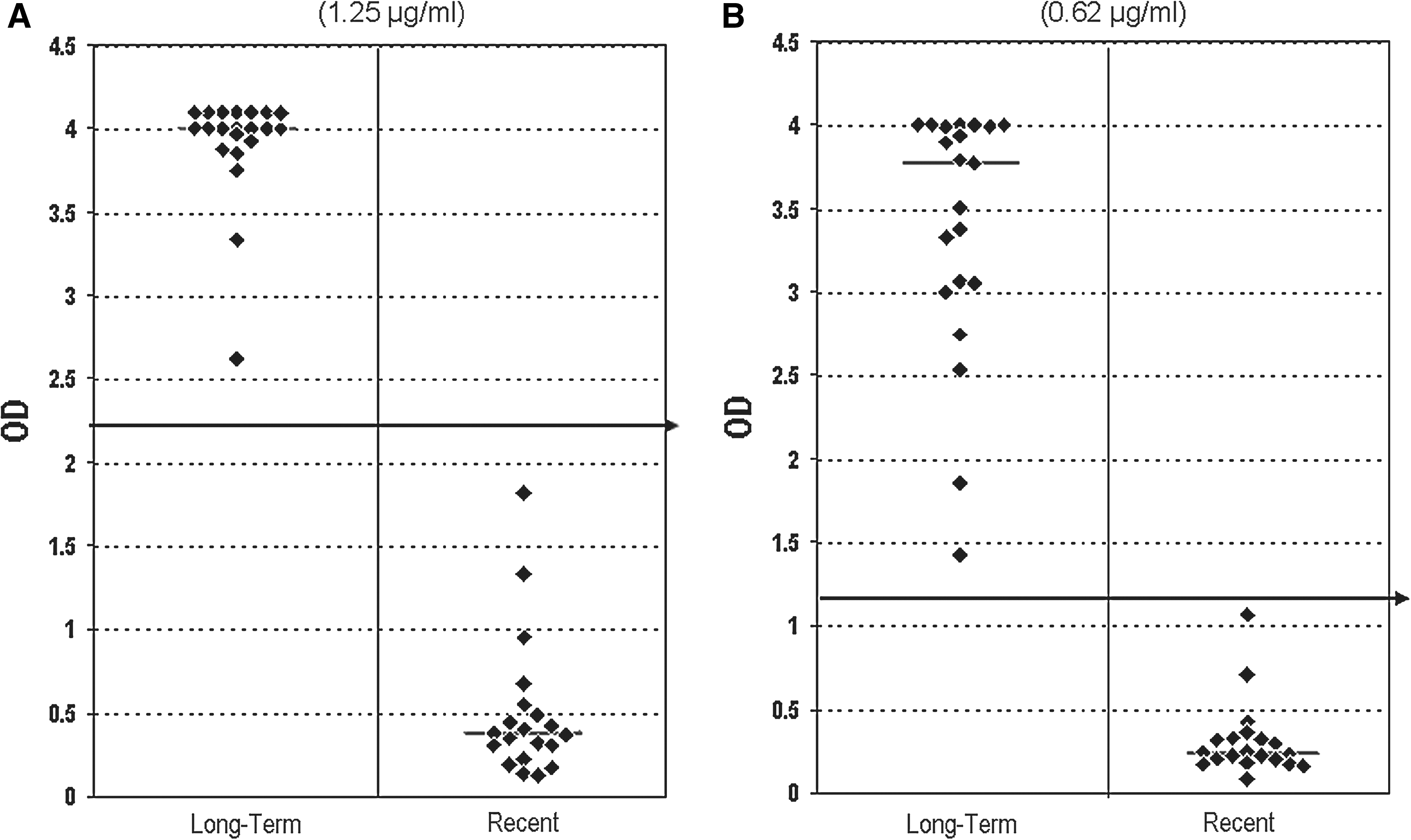
One-well limiting-antigen avidity EIA with pH 3.0 dissociation buffer using rIDR-M-coated wells at 1.25 μg/ml (
The cutoff lines shown (horizontal arrows) are arbitrary based on this small panel of specimens. The actual cutoff and associated duration of recency (i.e., window period) will be determined after extensive study with more specimens, including longitudinal specimens from seroconverters.
Discussion
We describe here the development of two avidity-based laboratory assays using a multisubtype gp41 recombinant protein: (1) a traditional two-well avidity index assay and (2) a new one-well limiting antigen avidity assay. Two-well avidity index assays, which usually include modifications of commercial diagnostic assays, have been described for HIV, CMV, and other infections to detect early infections. 35,40 –44 We developed a similar two-well in-house AI-EIA but used a multisubtype gp41 protein. In addition, we have used the same protein in a new one-well assay LAg-avidity EIA to distinguish recent and long-term infections. We also report the use of pH 3.0 buffer to dissociate low-avidity antibodies, instead of high concentrations of urea, guanidine, or other chemicals that can compromise the equipments and/or complicate the disposal.
Earlier reports described modifications of commercial HIV-1/2 EIAs to measure the avidity index of HIV antibodies and detect recent infections. 7,35,44 However, use of commercial assays may result in subtype-specific performance, as found earlier for LS-EIA, 24,25 and significant differences in duration of recency in divergent subtypes for detecting recent seroconversion. The use of the multisubtype protein, as described in this report, is critical for equivalent performance in different subtypes, as demonstrated in Fig. 2. The multisubtype antigen is important for assays that detect recent infections because of the quantitative nature of measurements, although it may not be essential or apparent for HIV diagnostic assays. Therefore, the use of rIDR-M should permit broader application of the avidity-based assays in populations infected with divergent HIV-1 subtypes. Our results on a limited but well-characterized set of specimens demonstrate that two-well AI-EIA and one-well LAg-avidity EIA are quite comparable (Figs. 6 and 7).
Janssen and others 13,14 described the use of less-sensitive assays for detecting recent HIV-1 infection. The approach required predilution of the specimen to 1/20,000, thus limiting the available HIV antibodies to detect recent seroconversion. However, the dilution process had to be performed in three steps and therefore was cumbersome and prone to error and variability. The LAg-avidity EIA instead uses a limiting amount of antigen on the wells, which allows use of a 1/100 dilution of specimen to distinguish recent from long-term infections. It is interesting to note that dissociation treatment was not necessary to identify specimens with recent HIV-1 infections (Fig. 4). Lowering the amount of coating antigen to 0.16 μg/ml was sufficient to identify recent seroconvertors. We found that the separation between recent and long-term infections can be improved when a pH 3.0 buffer step was included for dissociation of low-avidity antibodies. This one-well LAg-avidity EIA is a new concept that also may be applied to detect recent infections for other diseases.
The one-well LAg-avidity EIA will permit more specimens to be tested than the two-well AI-EIA. To increase the precision of the assay, we plan to use a calibrator specimen as part of the LAg-avidity EIA, which should allow normalization of the optical density values, similar to the BED assay. 45 Our experience with the BED assay has demonstrated that normalization of OD values significantly increased the reproducibility of the assay. We are in the process of defining a calibrator specimen for the LAg-avidity EIA to help reduce interassay variability and assist in the determination of an appropriate cutoff when longitudinal specimens from seroconverters are tested.
Based on the results of a five-member panel, we chose to use the limiting antigen amount in combination with pH 3.0 buffer for effective separation. Our data also demonstrate that the dynamic range of both assays and, hence, the possible cutoff can be shifted up or down on the basis of the coating concentration of the antigen (Figs. 6 and 7). We emphasize that the cutoff lines (arrows) shown in Figs. 6 and 7 are tentative based on limited number of specimens tested here and do not represent a definitive cutoff associated with a specific seroconversion duration for these assays. More work needs to be done to further optimize both AI-EIA and Lag-Avidity EIA and characterize essential parameters, such as mean duration of recency (mean window period) in different subtypes. 8,13,24,25 In addition, we need to determine the extent of false recent classification among known long-term infections 33,34 and the effects of antiretroviral therapies of varying length.
These assays are based on the functional property (avidity = binding strength) of developing HIV antibodies as opposed to LS-EIA and the BED assay, both of which measure a passive parameter such as the increasing levels of HIV antibodies. The assays measuring antibody avidity are less likely to be affected by disease states, low CD4, or viral load than the BED assay, as reported previously. 46 Further studies will help determine the impact of these factors on the new assays and will provide further guidance for their use for incidence estimates or risk factor analysis. In fact, use of an algorithm that involves two different assays based on two different principles should improve the predictive value of detecting recent HIV infection and the accuracy of incidence estimates. However, selected assays must have similar mean window periods in the population being tested. We plan to explore the utility of LAg-avidity EIA and AI-EIA individually, and in a multitest algorithm with another assay, to detect recent HIV-1 seroconversion.
Footnotes
Acknowledgments
The authors would like to thank Dr. J. Steven McDougal for his support, Drs. Chin-Yih Ou and Shambavi Subbarao for critical comments, and Drs. Kachit Choopanya and Suphak Vanichseni and the staff of the Bangkok Metropolitan Administration, Bangkok, Thailand for subtype B and AE specimens.
Disclosure Statement
No competing financial interests exist.
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.