
Abstract
The effect of enfuvirtide (ENF) in 11 HIV-1 heavily antiretroviral-experienced children and adolescents enrolled in the HIV-1 Paediatric Spanish cohort was further investigated. Patients who received ENF with novel drugs (etravirine, darunavir, and/or tipranavir) reached and maintained undetectable plasma HIV-1 RNA levels and showed immunological recovery within the first 3 months of therapy that was maintained during the follow-up. Viremia was not fully suppressed in patients who did not combine ENF with novel drugs but interestingly, immunological benefit was observed in half of these patients. Therefore, ENF showed a greater and more stable efficacy when administrated with novel drugs.
Introduction
A
Enfuvirtide (ENF) is the first HIV fusion inhibitor approved for the treatment of HIV-1 infection in antiretroviral-experienced adults and children aged >6 years. It is active against HIV-1 B 1 –3 and non-B subtypes. 4 Its potent ARV activity in HIV-1-infected pretreated pediatric patients has only been reported in clinical trials. 5,6 Therefore, additional information on the effect of ENF in HIV-1-infected children and adolescents in clinical practice is necessary.
Our aim was to evaluate the use of ENF in multiresistant HIV-1 pediatric patients with almost no available therapeutic options. Herein, we have assessed the virological, immunological, and clinical response to ENF in combination with nucleoside reverse transcriptase inhibitors (NRTIs), NNRTIs, and/or PIs in 11 vertically HIV-1-infected pediatric patients with previous virological failure during a follow-up of over 2 years.
Materials and Methods
The baseline was considered ENF initiation. A weight-adjusted dose of 2 mg/kg twice daily was chosen. 6 Demographic parameters were recorded. Plasma HIV-1-RNA levels and CD4+ T cell counts were measured at baseline and every 3–6 months for over 2 years. The background regimen administered with ENF was recorded and a physical examination including the evaluation of infection site reactions and adverse events related to ARVs was performed at baseline and during follow-up. To prevent local injection site reactions all patients received a Eutectic Mixture of Local Anesthetics (EMLA), topical mild massage, and hydrating skin care products. Patients were divided into two categories: children (6–12 years old) and adolescents (13–19 years old). Several samples were kindly provided by the Spanish HIV BioBank belonging to the Spanish AIDS Research Network (RIS). 7 Blood samples were processed following standard procedures and frozen immediately after their reception. Written informed consent was obtained from all patients' mothers and ethical clearance from the Institutional Ethical Committees was given. The administrative censoring date was considered May 2009. Values were recorded as absolute numbers/percentage and median with interquartile range (IQR).
Plasma HIV-1 RNA was measured using the commercial quantitative Amplicor Monitor assay (Roche Diagnostic Systems, Brandenburg, NJ), which has a lower limit of detection of 50 copies/ml. CD4+ T cells were counted by flow cytometry (Coulter, Madrid, Spain) using specific fluorescein-labeled antibodies. All samples included in the study were processed immediately after blood extraction.
Results
Overall, 11 vertically HIV-1-infected pediatric patients belonging to the HIV Paediatric Spanish Cohort (CoRISpe) were enrolled at five referral pediatric Spanish hospitals (Acknowledgments). Five were children [median age: 10 years (7–11)] and six were adolescents [15 years old (14–16)] (Table 1). They were born between August 1988 and March 2002 from HIV-1-infected women who acquired the virus mainly through sexual contacts (n = 7) and less frequently following intravenous drug use (n = 4). Ten were boys and their geographic origin was Spain (n = 9), sub-Sahara Africa (Mozambique) (n = 1), and Central America (Guatemala) (n = 1). Only the child from Mozambique harbored an HIV-1 subtype C virus.
ART, antiretroviral therapy; ENF, enfuvirtide; ABV, abacavir; ATV, atazanavir; AZT, zidovudine; ddI, didanosine; DRV, darunavir; d4T, stavudine; EFV, efavirenz; ETV, etravirine; FTC, emtricitabine; LPV/r, lopinavir and ritonavir; RTV, ritonavir; SQV, saquinavir; TDF, tenofovir; TPV, tipranavir; 3TC, lamivudine. N, absolute numbers; ND, data not available.
Potentially active drugs administrated with ENF are in bold characters.
At baseline, median plasma HIV-1-RNA was 71,331 (4.9 log) copies/ml (34,652–74,700) in children and 234,000 (5.4 log) copies/ml (129,775–287,827) in adolescents. The median CD4+ T cell count was 221 (13.5%) cells/mm3 (130–406) and 226 (7%) cells/mm3 (68-301), respectively. Among children (n = 5), three presented a severe immunological suppression (<200 cells/mm3), one a moderate immunological suppression (200–499 cells/mm3), and one no evidence of immunological suppression (≥500 cells/mm3). Two of six adolescents presented severe suppression before ENF administration, whereas four had moderate immune suppression. The clinical stage was B in four cases (one child and three adolescents) and C in seven cases (four children and three adolescents).
Before ENF treatment, all patients were heavily pretreated with highly active antiretroviral activity (HAART) and developed multiple drug resistance mutations to NRTI, NNRTI, and PI. In addition to ENF, ARV regimens included at least another active drug, containing the new NNRTI etravirine in two patients and the PIs darunavir and tipranavir in eight patients (Table 1). Three subjects received an NRTI + NNRTI + PI regimen, seven a PI-based regimen, and one had three NRTI (Table 1). The median time of follow-up with ENF was 108 weeks (70–151 weeks).
Four out of 11 patients achieved undetectable plasma HIV-1-RNA (≤50 HIV-1-RNA copies/ml): two children within the first 2 months and two adolescents after 4 and 24 months of ENF therapy. Two of them (one child and one adolescent) maintained suppressed plasma HIV-1-RNA and continued ENF administration until the end of the study. The third patient, a child, experienced an increase of plasma HIV-1-RNA up to 2 logs at the end of the follow-up. Finally, the fourth subject who achieved undetectable plasma HIV-1 RNA died during the study. He was 17 years old and died shortly after hepatic transplantation due to a recurrence of hepatitis C. He was coinfected with hepatitis C virus and cytomegalovirus, both acquired through vertical transmission. Notably, the background regimens of the two patients who achieved plasma HIV-1-RNA suppression within the first 2 months of follow-up included etravirine (ETV) + tipranavir (TPV) or darunavir (DRV) (Table 1). Immunological recovery of CD4+ T cell counts in patients with undetectable plasma HIV-1-RNA (n = 4) was achieved in one child (Δ350 cells/μl) and one adolescent (Δ531 cells/μl), whereas the immunological status remained stable in the others (Fig. 1).
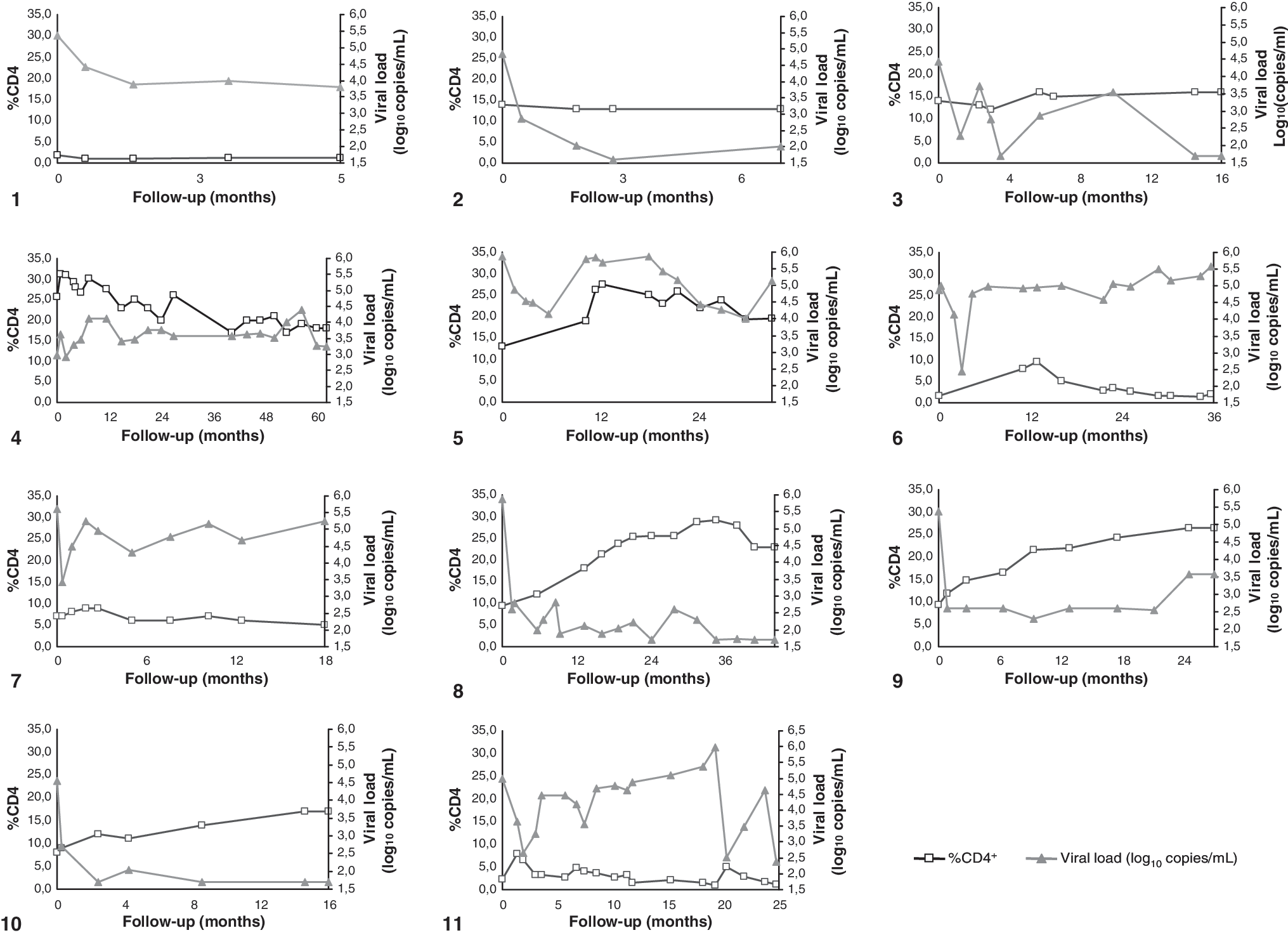
Follow-up of CD4+ T cell counts and viral load in all patients studied.
The potent antiretroviral activity of ENF, when added to an optimized HAART, did not fully suppress plasma HIV-1-RNA in 7 out of 11 subjects (three children and four adolescents). However, a decrease of plasma HIV-1-RNA ≥1 log in two cases and ≥2 logs in five cases was achieved during follow-up. Immunological recovery was observed in three of seven patients who did not achieve undetectable plasma HIV-1-RNA (Δ75 cells/μl), differing in the decrease (–Δ34 cells/μl) observed in the rest (n = 4).
During ENF administration, two patients experienced one change in their regimen: the first adolescent replaced efavirenz with lopinavir/ritonavir whereas the second child withdrew tenofovir.
ENF administration was interrupted in seven patients: two children and one adolescent who disliked injections and elected not to continue the study, one child due to ART failure, two adolescents who experienced virological failure, and one adolescent who died at age 19 years and who suffered from acute respiratory insufficiency caused by Streptococcus pneumoniae. Four of seven patients switched to HAART salvage therapy including ETV + DRV or TPV after failing ENF background regimens. Interestingly, at the end of the study, no patient showed ENF resistance mutations. Local site reactions and aversion to injection resulted in poor adherence in three of seven patients who finally decided to interrupt ENF administration at week 25, 33, and 36, respectively. In all but one (the child harboring HIV-1 subtype C) patient, ENF caused grade 1 to 2 local site reactions 3–4 days after the injection, such as bruising, edema of more than 2 cm of diameter, swelling, erythema, induration, and pain. No patient experienced any systemic adverse event related to ENF during follow-up.
Discussion
Increasing numbers of HIV-1-infected children and adolescents are currently failing the available treatment options. Until new data regarding novel drugs are available in the pediatric population, ENF could be a therapeutic option. Although randomized controlled trials evaluating ENF efficacy and safety have previously been carried out, 5,6,8,9 this is the first epidemiological study characterizing the clinical, virological, and immunological response to ENF in a heavily pretreated HIV-1-infected pediatric cohort followed for over 2 years in a clinical setting. In pediatric patients efficient HIV-1 replication control is limited by their immature immune system.
Our study has shown that four patients reached virological suppression (≤50 copies/ml) during the follow-up. These data are consistent with clinical trials. The P1005 clinical trial conducted by Church et al. 6 found a virological suppression of ≤50 copies/ml in 21.4% (3/14) of cases and ≤400 copies/ml in 43% (6/14). Wiznia et al. 9 also noted that 21.2% (11/52) of patients achieved ≤400 copies/ml in the T20-310 clinical trial. Many factors may contribute to the failure of ARV regimens, hampering good adherence to the prescribed regimens. 10 The virological failure observed in our patients treated with predictably effective and potent regimens likely reflects this challenge.
The present study shows that ENF therapy regimens exerted a greater benefit when combined with at least a novel active drug. By contrast, ENF was not totally effective when administrated as the only complete active drug. Side effects related to ENF were mild and transient. Injection site reactions were very frequent as previously observed. 3 However, no systemic adverse events related to ENF have been observed in our patients. The limited size of the study population could be considered a shortcoming. However, it should be noted that this limitation is also present when evaluating clinical trials in pediatric patients. 6 In conclusion, ENF shows a greater and more stable efficacy when administrated with novel drugs.
Footnotes
Acknowledgments
Spanish Group of Paediatric HIV Infection: participating hospitals and personnel staff in this article. Hospital General Universitario “Gregorio Marañón”: C. Palladino, V. Briz, J.M. Bellón, S.J. de Ory, D. García Alonso, M.D. Gurbindo, M.L. Navarro, and M.A. Muñoz-Fernández. Hospital Universitario “12 Octubre”: M.I. González-Tomé. Hospital Infantil Unversitario “Virgen del Rocío”: J.A. León Leal. Hospital Universitario “La Paz”: M.I. de José, F.J. Climent. Hospital Universitario de Getafe: J.T. Ramos. Special thanks to Santiago Jiménez de Ory for his support and contribution to this study.
Spanish paediatric hospitals of the multicenter network: Hospital Universitario “Doce de Octubre,” Madrid (five patients); Hospital Virgen del Rocio, Sevilla (three patients); Hospital General Universitario “Gregorio Marañón,” Madrid (one patient); Hospital Universitario “La Paz,” Madrid (one patient); and Hospital Universitario de Getafe, Madrid (one patient).
This work was supported in part by grants from Red Temática de Investigación Cooperativa Sanitaria ISCIII (RED RIS RD06/0006/0035), Fundación para la Investigación y Prevención del SIDA en España, FIPSE: 240800/09, Fondo de Investigación Sanitaria (PI09/02029), Fundación Caja Navarra, and the Pediatric European network for treatment of AIDS (PENTA). Claudia Palladino is supported by a grant from Istituto Pasteur, Fondazione Cenci-Bolognetti, Università degli Studi di Roma “La Sapienza,” Rome, Italy. Verónica Briz is supported by a grant from Fondo de Investigación Sanitaria (FI05/01046).
Author Disclosure Statement
No competing financial interests exist.