
Abstract
The molecular epidemiology of subtypes and intersubtype recombinants (IRs) of human immunodeficiency virus type 1 (HIV-1) in Mexico has not been characterized fully. Understanding its regional distribution, prevalence, adaptability, viral fitness, pathogenicity, and immunogenicity is decisive for any design of an effective HIV vaccine. The aim of this study was to describe the presence of IRs types BG and BF in a Mexican population. Protease and reverse transcriptase regions of the pol gene were sequenced using an automated sequencing system. A phylogenic tree was constructed and genetic distances were calculated using MEGA 3.1. Recombination analysis was done by bootscan using SimPlot software. Two hundred and twenty-three HIV-1-positive individuals were enrolled in the study. At baseline, the mean plasma viral load was 285,500 HIV-1 RNA copies/ml and the mean CD4 cell count was 213 cells/ml. Subtype B was found in 220 (98.6%) samples, whereas IRs were found in three patients (1.4%): two (0.9%) with BG and one (0.45%) with BF. IRs were observed in 2/124 (1.6%) samples from treated patients and in 1/99 (1.0%) from naive patients. The presence of these HIV forms at low frequency points to the need for research on the diversity, geographic distribution, and evolution of other subtypes including circulating recombinant forms and IRs to understand the molecular epidemiology and tendencies of the HIV infection in Mexico.
Introduction
G
Phylogenetic analysis of HIV samples has led to the classification of HIV-1 into three genetic groups: M (major), O (outlier), and N (non-M, non-O). Most HIV-1 infections globally are caused by group M viruses; variation between subtypes is approximately 25–35%.
4,5
Group M viruses have developed an extraordinary degree of genetic diversity, and most can be segregated into nine subtypes, more than 43 circulating recombinant forms (CRFs), and intersubtype recombinants (IRs) (
Variations in the viral protease (PR) and reverse transcriptase (RT) genes entail 10–12% of nucleotides encoding 5–6% of amino acids. 6 Recombination among genetically distinct strains and between subtypes of HIV-1 is increasing in the worldwide AIDS epidemic. It has been estimated that recombination of HIV-1 contributes to infections in 10–40% of patients in Africa and 10–30% in Asia. 2
Structural differences between subtypes allow for various phenotypic properties including viral transmissibility and ability, progression of infection, mortality rates, and patterns of mutations, among others. 3 Identification of the geographic distribution of viral subtypes can help in establishing epidemiological predictions concerning the spread of HIV, therapeutic strategies, and the design of vaccines. 7
Despite universal access to antiretroviral therapy and the use of national guidelines for antiretroviral treatment, 8 Mexico has had 130,969 AIDS cases up to March 2009, with a dampened growth trend. 9
Subtype B is currently the most studied. As in the rest of the Americas and Western Europe, Mexico is HIV-1 subtype B predominant; however, the molecular epidemiology of the HIV-1 IR forms is unknown in this country. 10,11 This information is essential to developing and forming a preventive strategy 4 and pathogenicity. 12
Migration from Central American countries to the United States and tourism between other Latin American countries such as Cuba, Argentina, and Brazil, 13 where there are subtypes B and C and the IR variant BF, could contribute to introducing other subtypes to Mexico and the United States. The aim of the current study was to describe the frequency of IRs in Mexico.
Materials and Methods
Sample collection
Samples were obtained between 2002 and 2008 from patients enrolled in clinical research for resistance testing in the course of the evaluation and care of HIV infections. A prospective study was conducted in three large public medical centers in the western region of Mexico. Samples were collected from antiretroviral-naive and antiretroviral-treated patients. After participants of the study had signed an informed consent form, in accordance with Mexican public health legislation, a plasma sample was obtained and stored at −85°C until used. Quantification of HIV-1 RNA levels was performed using the Amplicor HIV monitor (Roche Molecular Systems Inc., Belleville, NJ) according to the manufacturer's instructions. CD4 and CD8 lymphocyte cell counts were determined by flow cytometry.
Virus isolation and sequencing
Viral RNA was extracted from patient plasma using QIAamp viral RNA kits (Qiagen, Hilden, Germany). Viral RNA was transcribed into complementary DNA, followed by polymerase chain reaction for the PR (codons 1–99) and RT (codons 39–244) genes using the TruGene assay (Siemens, Toronto, Ontario, Canada). Amplification products were directly double-stranded sequenced using a Long Read Tower automated sequencing system (Siemens). All chromatograms were inspected visually and compared with the wild-type sequence of the reference strain (HIV-B-LAV1; GenBank accession number M19921) using GeneLibrarian software (Siemens).
Sequence analysis
A representative genome for each major subtype was downloaded from the Los Alamos database (
Sequences were aligned using Clustal W (
Statistical analyses
Differences between naive and treated patients and between the outcomes of patients with subtype B and those with non-B were evaluated using the chi square test and Yates' corrected chi square test, and Fisher's exact test was used for expected sample sizes of five or fewer. The data were first tested for normality of distribution and the Student's t-test was then used to compare the means of CD4 counts and viral loads. Statistical analysis was performed using SPSS version 13 (SPSS Corp., Chicago, IL).
Results
Two hundred and sixty HIV-1-positive individuals were eligible for continuous inclusion in the study. From these patients, 223 samples were amplified successfully. Thirty-seven patients were excluded [15 had incomplete sequences (only PR or RT) and 22 were discounted due to incorrect preservation of the plasma samples at the participating medical center]. At the time of sequence analysis, the mean HIV-1 RNA level was 285,500 copies/ml (range 400–750,000), and the mean CD4 cell count was 213 cells/ml (range 3–1,117). Overall, 220 isolates (98.7%) were subtype B (Fig. 1), and there were three IRs (1.4%). Among these patients, there were two BG type IRs (0.9%) and one BF (0.45%; Figs. 2 and 3). There were no significant differences in the mean viral loads or CD4 cell counts between patients with subtype B and those with IRs.
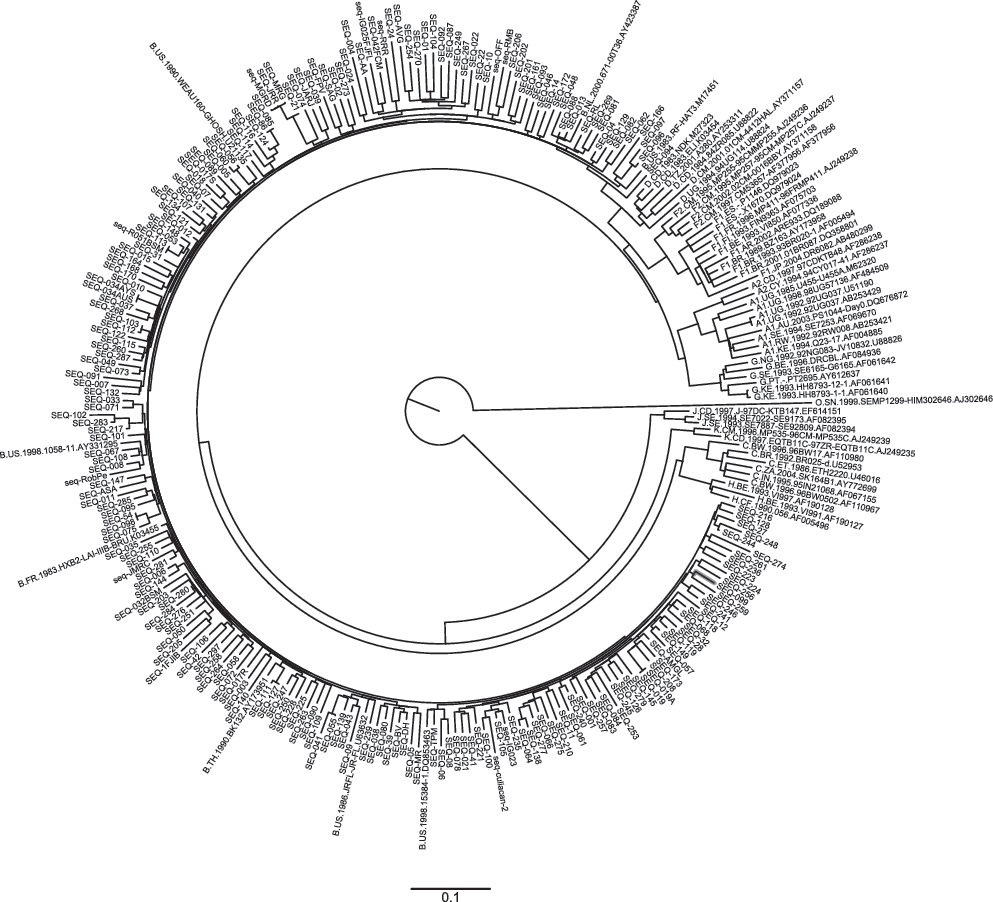
Phylogenetic tree of a pol region of the subtype B isolates. The neighbor-joining tree was constructed using Kimura two-parameter distance matrices. The robustness of these relationships was tested by the bootstrap method, using 1000 replications, and analyses were conducted using Mega software version 3.1.
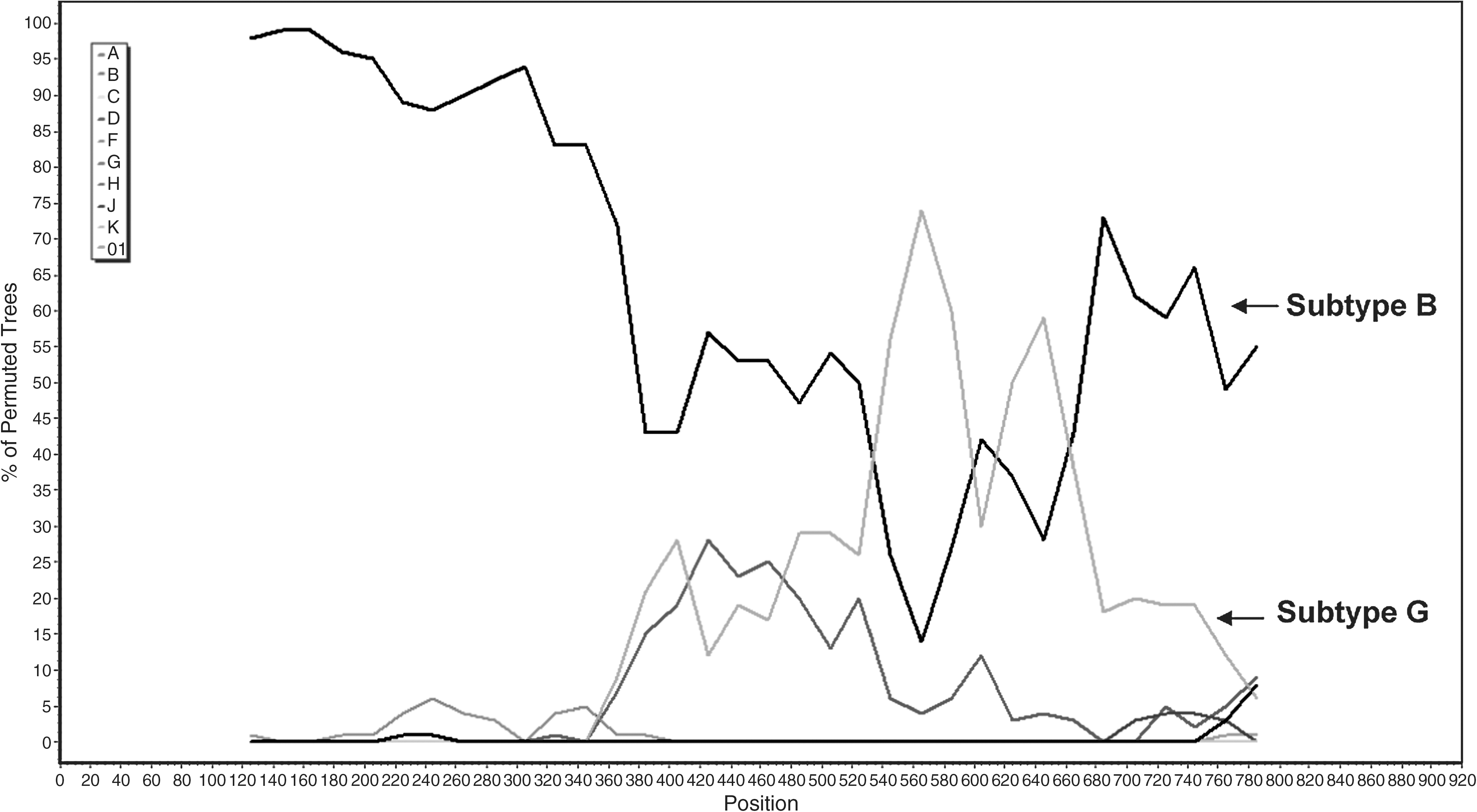
Intersubtype recombination BG of PR-RT region isolates from Mexico was analyzed by bootscan using SimPlot version 3.5.1 software, with a window size of 250 bp and a step size of 20 bp. A 70% bootstrap support was considered definitive for assigning any recombination.
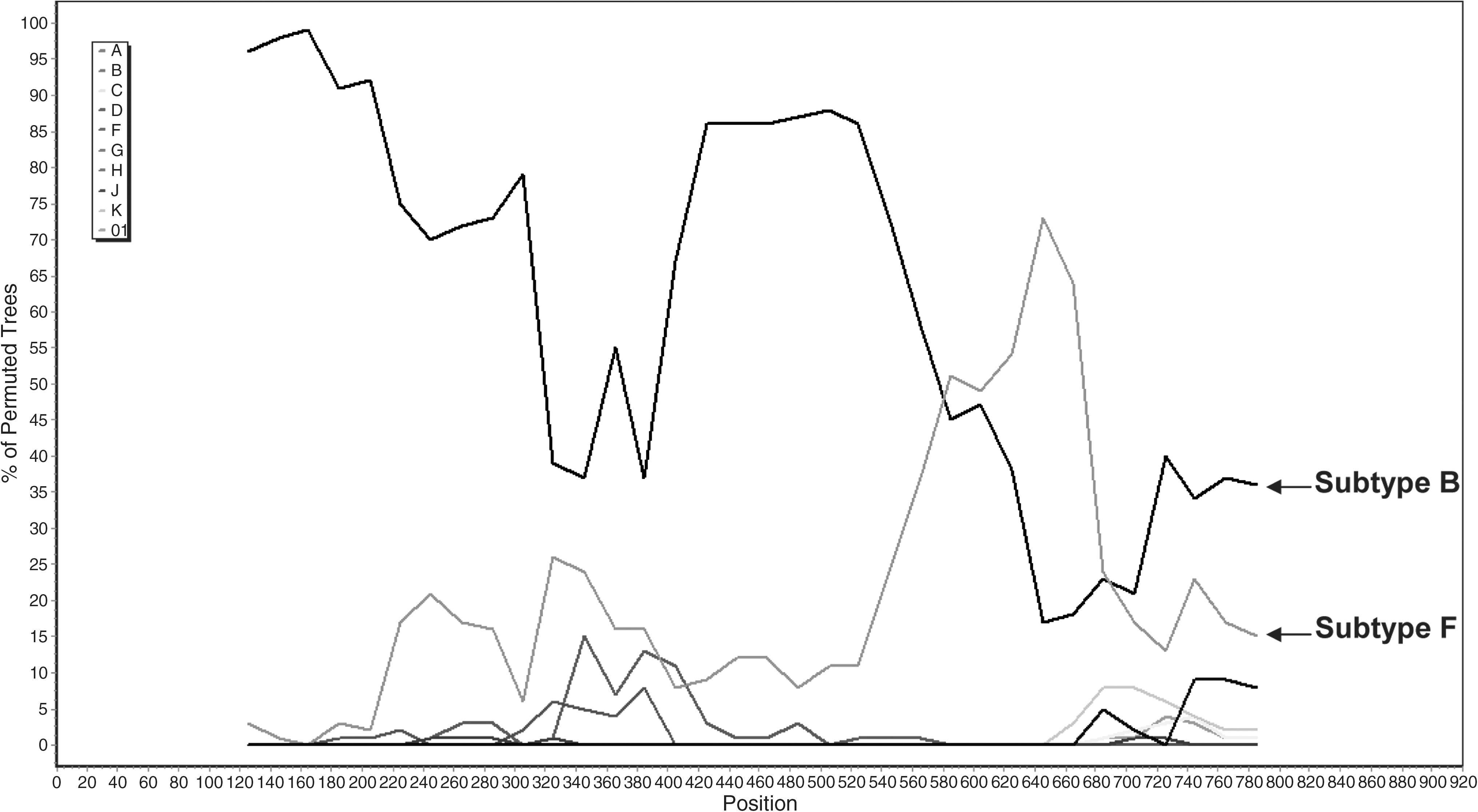
Intersubtype recombination BF of PR-RT region isolates from Mexico was analyzed by bootscan using SimPlot version 3.5.1 software, with a window size of 250 bp and step size of 20 bp. A 70% bootstrap support was considered definitive for assigning any recombination.
Patients with treatment
One hundred and twenty-four patients (109 men and 15 women) received highly active antiretroviral therapy. The mean HIV-1 RNA count was 237,543 copies/ml (range 704–750,000), and the mean CD4 cell count was 218 cells/ml (range 3–1117). There were two patients with an IR virus in this group: one with the BG type (0.8%) and one with BF (0.8%).
Naive patients
Ninety-nine patients were naive to antiretroviral treatment (89 men and 10 women). The mean HIV-1 RNA count was 344,162 copies/ml (range 400–750,000), and the mean CD4 cell count was 200 cells/ml (range 4–779). Subtype B was observed in 98 (99%) of the samples and IR type BG was found in one (1%). There were no significant differences between treated and untreated groups in terms of the incidence of IRs.
Epidemiological data
Of the 223 eligible subjects, 58 (26%) came from the northwestern area of Mexico (the states of Jalisco, Michoacán, Colima, Nayarit, and Sinaloa) and 165 (74%) came from the central east (Mexico City and the states of México, Morelos, Puebla, and Veracruz). They had a mean age of 42.89 ± 10.3 years with ages ranging from 19 to 84 years old. All were infected by sexual transmission. Of them, 170 (76.2%) were men who have sex with men (MSM), 28 (12.6%) were heterosexual men, and 25 (11.2%) were heterosexual women.
All three IRs were identified from MSM who were from the central region of the country and who received specialist medical care in a hospital. Among the patients who had taken antiretroviral treatment, one had received bitherapy with nucleoside analogues, zidovudine (AZT)/lamivudine (3TC), and a second biotherapy patient received bitherapy with different nucleoside analogues, AZT, 3TC, didanosine, zalcitabine, stavudine, and a nonnucleoside analogue (nevirapine). Neither of the patients had received triple therapy or PR inhibitors.
Only the patient who had received treatment with antiretrovirals presented resistance mutations M184V and Y181C. The other two showed no genotypic resistance mutations, either primary or secondary. It is unknown whether any of these men had a history of travel outside of Mexico or of having sex with foreigners.
Discussion
Here we report the intersubtype recombination identified in HIV isolates from western Mexico with a preponderance of HIV-1 subtype B, where IR types BG and BF had not been previously reported. The presence of IRs in Mexico was probably caused by the prior introduction of subtypes F and G and their recombination with subtype B, prevalent in this country. Alternatively, the IRs might have been imported. 16 Both scenarios can be verified or discarded only if it is possible to do a phylogenetic reconstruction of the transmission events in order to identify the origin of these BF and BG recombinants. 17
The worldwide prevalence of IRs in HIV is 18%, 5 and most countries are monitoring their evolution, including subtypes and CRF prevalence, in an effort to understand the molecular epidemiology and to support the global program for vaccine development. 17
In this region of Mexico, we found a prevalence of 0.45% for the BF type of IR, less than that reported for other Latin American countries such as Argentina (40–60%), 18,19 Brazil (8–22.7%), 20,21 Chile (15%), 22 and Cuba (11.6%). 23
The BG variant related to syncytium formation induced by the CXCR4 coreceptor 24 has been reported in Germany, Spain, and Cuba. In Spain, especially in Galicia, this IR and the CRF14_BG were encountered among injecting drug users. 25 In Cuba, three CRFs were encountered from a common ancestral recombinant of the B and G subtypes, with parental strains circulating in the Caribbean region. 23,26 The absence of subtype G in Mexico makes it unlikely that the BG variant of IR arose from Mexican parental strains. Therefore, the findings probably indicate a recent introduction of subtype G from Spain or Cuba, where BG is prevalent. However, clarifying this requires a retrospective study of viral evolution. Germany has a low rate of migration to Mexico, which reduces the likelihood that the IR came from that country.
We found a similar frequency of IR among the patients with and without treatment, unlike previous suggestions that IRs arise from selective pressures produced by antiretroviral drugs. 27 Because the overall prevalence of IR found in this study was low, it will be necessary to increase the sample size and include other regions of the country. Phylogenetic analysis and sequencing of the entire genome, or alternatively at least two distant genomic regions, including the pol and env genes, are complementary to discriminate between IR and CRFs.
In conclusion, the presence in Mexico of the IR variants BG and BF at low frequencies among HIV-1 positives supports the need for further research on the diversity, geographic distribution, and evolution of other subtypes, CRFs, and IRs to understand the molecular epidemiology of HIV infection in Mexico.
Sequence data
The sequences have been deposited in GenBank with the following accession numbers: EU045452–EU045456, EU045458–EU045461, EU045463, EU045466, EU045468–EU045480, EU045481, EU045487–EU045488, EU045490–EU045495, EU045497–EU045500, EU045503, EU045506, EU045509–EU045521, EU045524, EU045532–EU045533, GU291863–GU291875, GU291877–GU291952, GU291954–GU291955, GU382757–GU382851, and GU437199–GU437200.
Footnotes
Acknowledgments
This research was supported in part by the Fundación Mexicana para la Salud, Capítulo Jalisciense, A.C.
Author Disclosure Statement
No competing financial interests exist.