
Abstract
Southern Brazil has the highest prevalence rate of AIDS in the country and is the only region in the Americas where HIV-1 C prevails. Metropolitan areas and harbor cities have been evaluated, but limited information is available for small towns and specific populations. We studied women attending the obstetric outpatient clinic of Criciuma, State of Santa Catarina in 2007 to evaluate the molecular epidemiology of HIV-1 among pregnant women living with HIV/AIDS. Forty-two cases had partial pol gene sequenced and additional partial gag and/or env genes from nine women. HIV subtyping was evaluated by phylogenetic methods and antiretroviral (ARV) drug resistance mutations (DRMs) at the Stanford Database. DRMs to one or more ARV class was observed in 20/42, 48% of cases, with 15/41, 37% with viral load <500 copies/ml. Subtype C at pol was identified in 33/42, 78.6% (95% CI: 64–89%), C mosaics (CB, CF) in 2, 4.8% (95% CI: 0.8–19%), F in 4, 9.5% (95% CI: 3–21%), and B in 3, 7.1% (95% CI: 1.8–18%). Discordance in concatenated gag/pol/env or intraregion mosaic was observed in 1/9, 11% of HIV-1 C genomes. The proportion of HIV-1 C in this study is the highest rate described in the Americas. Molecular surveillance in specific populations is instrumental for a better understanding of the Brazilian HIV epidemic.
D
The study was open to all pregnant women in this period and to 20 mothers of children living with HIV/AIDS with previous obstetric follow-up. These women agreed to participate and signed an informed consent form. TCD4 count and HIV RNA viral load were obtained from the local Reference Laboratory. Biological material (plasma and/or PBMCs cell) was collected and preserved at −20°C until transport in dry ice to the Retrovirus Laboratory of Adolfo Lutz Institute (State of São Paulo) for genetic sequencing. HIV RNA was extracted using the Quiamp viral RNA mini kit (Quiagen, Germany) according to the manufacturer's instructions. Complementary DNA synthesis was performed with the SuperScript III enzyme (Life Technologies, USA). HIV polymerase fragments spanning the entire protease (PR) gene and partial reverse transcriptase (RT, codons 1–235, relative to HXB2) were obtained by nested PCR, 12 and gag and envelope 13,14 were obtained from some cases with subtype C at the pol gene. Purified products were sequenced in an automatic ABI 3100 Genetic Analyzer (Applied Biosystems, USA). Chromatograms were assembled with Sequencher software and manually edited to identify nucleotide mixtures. Screening for HIV-1 subtypes was done with NCBI and REGA HIV-1 web-based subtyping tools and further characterized by phylogenetic analysis. Multiple alignments were performed using Clustal W with a reference set available in the Los Alamos HIV-1 database, using outgroup HIV-1 OSEMP1300. Neighbor joining (NJ) and maximum likelihood (ML) trees were constructed based on nucleotide substitution models (Modeltest v3.7), tested with a hierarchical likelihood ratio test using PAUP (v4b10). Zero length and bootstrapping were performed using the stepwise addition algorithm for 1000 replicates.
A representative NJ tree (GTR + I + G model) is depicted in Fig. 1. Sequences showing discordant genomic subtyping, outlier behavior on NJ trees, or any non-B signal in NCBI were selected for bootscanning analysis using SIMPLOT 2.5 to evaluate recombination breakpoints and inspection of signatures. The mutation profile was analyzed at the Stanford HIV Drug Resistance Database and tropism prediction by the 11/25 rule and at two websites, Geno2Pheno (Max Planck Institute,

Representative neighbor-joining phylogenetic tree of partial pol region sequences of the study (in bold), generated with the GTR + I + G model, using Paup 4.0. Reference HIV-1 subtypes were obtained from the Los Alamos HIV Sequence Database. Bootstrap values above 70% in key branches are depicted, with branches with zero length test significant values of *p < 0.05 and **p < 0.01. A shadow box highlights the clustering of the query sequence (BR07SC338, underlined) with HIV CRF_31 BC references.
HIV sequences were analyzed from 42 individuals: 24 woman pregnant at collection and 18 previous clinic clients, 14 woman and 4 unrelated children. Children's material was processed and amplified whenever the child's mother presented an inadequate sample for sequencing. The median age was 27 years old, the median TCD4 was 504 cell/mm3, and the median viral load was 3.57 log10. Table 1 describes demographic and laboratory data of the study population. Among the women, all referred to sexual intercourse as the source of infection, with a median age of 15 years at the first sexual relationship. Poor adherence to antiretroviral therapy (ARV) medication was reported by 33% of cases. Additional sociobehavioral information may be found elsewhere (S.A. Manenti et al., unpublished observations) HIV-1 subtype C at pol was observed in most cases, 33/42, 78.6% (95% CI: 64–89%). Mosaic genomes were observed in 2/42, 4.8% (95% CI: 0.8–19%) with one CB and one CF. The CB mosaic at pol showed a small B segment at RT with breakpoints compatible to that of CRF_31BC (Figs. 1 and 2). Subtype F at pol was observed in 4/42, 9.5% (95% CI: 3–21%) and B pol in 3/42, 7.1% (95% CI: 1.8–18%). HIV gag and env from a subset of subtype C at pol were additionally sequenced.

(
ID, sample identification.
POP, study populations groups: PW for women pregnant at time of collection, W for women with previous pregnancy, and C for children from a previous pregnancy of women with material not available for analysis, all females except for two male children (301_07 and 305_07).
HIV diagnosis, year of HIV diagnosis.
CDC clinical staging.
Viral load (copies/ml) and fTCD4 count (cell/mm3) at last observation before collection.
ARV, antiretroviral in use, either for prophylaxis of MTCT or previous treatment.
Mutations (W for wild or DRM at resistance-associated codon) and ipredicted drug susceptibility (S, susceptible; PLLR, potential low level resistance; LLR, low level resistance; IR, intermediate resistance; and HLR, high level resistance), defined by the Stanford database at protease (PR) or reverse transcriptase (RT).
HIV subtype by region (Gag, Pol, Env) and lpredicted tropism.
NA, information not available.
—, sequence not available.
All env sequences had a predicted R5 tropism (Table 1). Discordant gag/pol/env regions were observed in 1/9, 11% of cases with more than one region evaluated. Figure 3 depicts the partial pol amino acid alignment of international consensus B and consensus C (NCBI), our dataset 9,11,12 of southern Brazil consensus C and study C sequences from nontransmitting pregnant women and transmitting mothers (nontransmitting pregnant women for study participants pregnant at the time of the study with an HIV-negative child on follow-up evaluation and transmitting mother for women participating in the study with a previous HIV-positive child). Typical clade C amino acid polymorphisms at protease (Fig. 3a) were observed, but our sequence set had amino acid signatures present in the south Brazil subtype C consensus but not in the international NCBI subtype C consensus (S12T, I19L, N37K, and K41N), the two first present in clade B consensus. L63P are observed in the majority of pregnant women, all with use of protease inhibitors. At reverse transcriptase (RT) (Fig. 3b) the southern Brazil data set and study sequences showed differences from the international consensus (E39D and G123D) and polymorphisms at A173T, V317L,and I326V were observed among pregnant women.
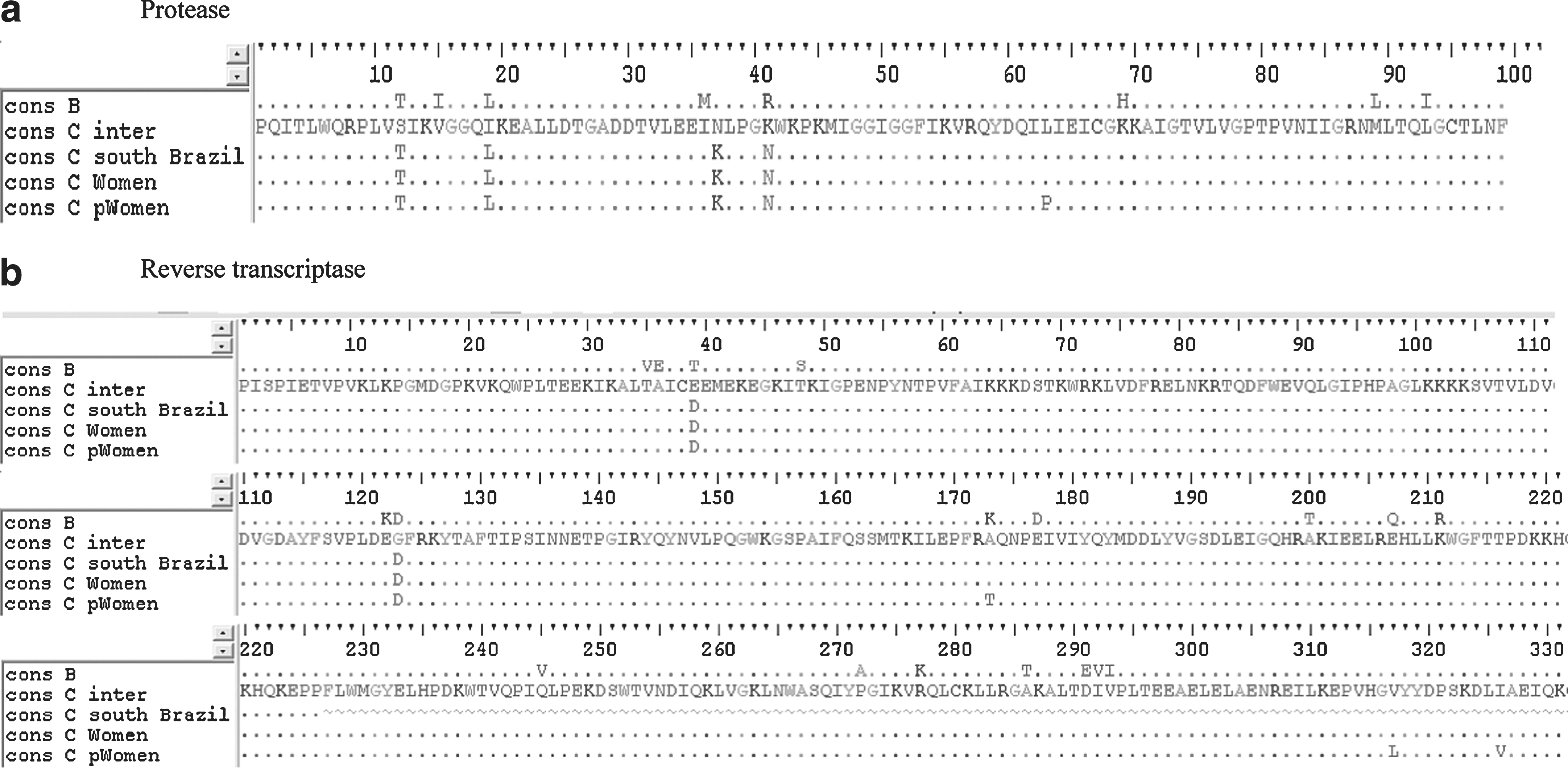
Partial pol amino acids alignments. (
All pregnant women received either ARV treatment or prophylaxis for prevention of vertical transmission. Follow-up information has revealed that no cases of HIV transmission were observed among these pregnant women. As for the mothers enrolled, all had one or more HIV-positive offspring. In most cases the ARV medication constituted an NRTI backbone (zidovudine + lamivudine) with nevirapine or one PI, lopinavir or nelfinavir (Table 1). Although HAART has been used (either for treatment or prophylaxis) at the time of collection, only 15/41, 37% of cases, had a plasma viremia below 500 copies/ml. The most common mutation observed to the NRTI class was M184V in 11/40, 27.5% of cases, and to NNRTI the codon K103N (5/40, 12.5%). At PR, the major resistance mutation, L90M, was observed in 3/41, 7.3% of cases. Drug resistance mutations (DRMs) to one class were observed in 4/42, 9.5%, to two classes 13/42, 31%, and triple class resistance in 3/42, 7.1%. Table 1 depicts the DRM and predicted ARV susceptibility observed in this study.
This is the first report of a molecular epidemiological evaluation of young women living with HIV/AIDS identified at an obstetric clinic serving small communities in south Brazil. A low proportion of subtype B (7%) was observed. Even when considering the confidence interval (95% CI: 1.8–18%), large due to the small sample size, such a low estimate for subtype B pol genomes has not been reported in any study in the Americas. Some polymorphisms are observed, most common to other HIV-1 C sequences from south Brazil. Our small sample size is a major drawback for the interpretation of these findings. However, as we evaluated a small community, in fact that sampling comprises almost all available pregnant women at the time when study participants were recruited.
With a total population of about 220,000 inhabitants in the major city and nearby villages, and considering the national estimates for HIV infection (0.61), the estimation for the number of individuals living with HIV/AIDS in this area would be of 1342 individuals. With a prevalence estimate for females of 0.42% (0.8% among males), and assuming that females correspond to about half of the population, we could estimate that about 462 women would be HIV infected in the area. In this setting, the small sample not only represents most women living with HIV/AIDS visiting the obstetric clinic at the time of the study but almost 10% of the HIV-infected female population at the region. Another limitation is the limited access to quality samples for analysis. In some cases where it was not possible to obtain an HIV genome sequence from the women, material from their offspring was studied instead. All these cases were confirmed as mother-to-child transmission (data not shown).
Although the preponderance of clade C in this population might somehow be modulated by an increase in vertical transmissibility of clade C, studies in the region 15 and abroad 16 do not support a differential transmissibility of HIV clades so we can assume that the data from their children represent the HIV clades from their mother. In fact, the proportion of clade B among these children is higher than that observed among adult females. Therefore, our data might document the actual predominance of clade C among HIV-infected young females in this area.
Resistant mutations were present in most treated women. NNRTIs and NRTIs were more common in this population. This is in accordance with the literature 17 in which cases failing therapy based on lopinavir, resistance mutations to this drug are less often observed. It is noteworthy that only 37% of cases had a viral load below 500 copies/ml at the time of collection, highlighting the fact that although Brazil has free access to HIV medication for treatment or prophylaxis, and extensive effects have been deployed to foster mother-to-child transmission control, additional efforts in medication adherence are needed.
To improve the comparability with other studies, we have applied a methodology similar to that used in other cities in South and Southwest Brazil. As in other towns, recombinants have been frequently observed. In this population two samples showed recombination at pol and one discordant gag/pol/env genome. It is noteworthy that one pol recombinant structure shows a breakpoint compatible to the CRF-31, suggesting the presence of this variant in the region. A CRF_31-like recombinant pattern is common in some areas of the largest metropolitan area in the region, Porto Alegre. 12 Moreover, it has been detected in other areas of the States of Rio Grande do Sul 18 and Santa Catarina. 11 This may suggest that either this breakpoint constitutes a recombinant hotspot or the variant may have some fitness advantage that favors its spread in the region. Another finding of potential interest is the fact that in this small sample, frequent mosaics (8.6%) were observed among clade C genomes.
The fact that the gene regions studied comprised only part of the HIV genome suggests that the actual figure would be higher. Frequent B/F mosaics, reflecting the decades of B and F coexistence in areas of Brazil such as São Paulo and Rio de Janeiro, have been documented by different groups. 4, 5 Although not proof of the advantage of the HIV-1 C clade over the others, the historical data of a mostly B epidemic in the area in the 1990s, along with the presence of CF and CB mosaics, might suggest that the C clade prevails in the area after a period of a few decades of B/C/F coexistence. Monitoring the expansion of the HIV-1 C and its mosaics to other regions is an important issue in the surveillance of the dynamic of the HIV epidemic in Brazil.
Footnotes
Acknowledgments
This work was supported by the Brazilian AIDS Program (914/BRA/1101-UNESCO/CFA/178/04; FAPESP 2006/61311-0) and Adolfo Lutz Institute, Disease Control Coordination, Secretary of Health, São Paulo, Brazil.
Author Disclosure Statement
No competing financial interests exist.