
Abstract
Antiretroviral therapy (ART) has improved the survival of HIV patients but is also associated with unique manifestations of disease in some subjects during the initial months of therapy. Immune reconstitution inflammatory syndrome (IRIS) is a disorder among individuals starting ART, with no evidence-based treatment and management guidelines. We characterized HIV-1 and determined drug resistance among 14 Kenyan patients with suspected IRIS after ART initiation in 2005. Polymerase chain reaction, sequencing, and phylogenetic analysis of viral pol and env showed the following HIV-1 subtypes: A1/A1/A1 (pol-RT/gp41/C2V3), 5; A1/C/A1, 1; A1/D/A1, 2; D/A1/A1, 1; D/C/A1, 1; D/D/A1, 2; D/D/D, 1; and D/A1/A2, 1. Three patients had viruses with major drug resistance-associated mutations. These included nucleoside reverse transcriptase inhibitor (RTI) mutations: M41L, K65R, D67N, K70R, M184V, and K219Q, and nonnucleoside RTI mutations: K101P, L100I, K103N, and Y181C. Twelve patients harbored viruses that are predicted to use chemokine coreceptor 5 (CCR5) whereas two had variant viruses predicted to use the CXCR4 coreceptor. Drug resistance may not be the only cause of ART adverse events. HIV-1 characterization would be important before and during HIV therapy to avoid treatment failure.
H
Despite the success of ART, drug resistance is a consequence that limits successful treatment. 5 With rapid scale-up of ART in resource-poor settings and the lack of proper ART monitoring infrastructure, most adverse events associated with ART would be misclassified as treatment failure with a consequent change of regimen as the best option.
In Kenya, free ART was introduced in 2003 and its availability to those in need has steadily increased, having reached 54% of the estimated people in need by June 2008 (
Several anti-HIV drugs have been tested and their efficacy determined and approved; drug resistance mutations associated with these drugs have also been documented. 6 The use of alternative drugs with novel targets remains to be explored for better management of patients to avoid the emergence of drug resistance. For instance, the recently approved entry inhibitor maraviroc—active against HIV virus that exclusively uses the chemokine coreceptor 5 (CCR5)—is promising, despite the shifting nature of HIV tropism in the cause of disease. 7 This calls for determination of coreceptor usage before its administration, which can be inferred genotypically or by phenotypic assays. 8
As the rates of HIV-1 infection, recombination, and drug resistance among the infected in resource-poor settings increase, so should alternative measures be undertaken to counter this effect in the management of patients through available, affordable, feasible, and accessible strategies. To address this, and further establish whether HIV-1 diversity and drug resistance are major factors associated with ART adverse events, the current study aimed at characterizing HIV-1 and associated drug resistance mutations among individuals suspected of having developed IRIS after the initiation of ART. It was hoped that the findings would provide additional evidence to guide National ART programs on the selection of effective regimens to combat emerging challenges in the provision of ART.
Blood samples were collected from 175 HIV-1-positive patients. They were over 18 years of age and provided informed consent before enrollment in the study. The patients sequentially presented themselves to a care clinic in April and May 2005. Those below 18 years of age and those who did not consent were excluded from the study. Demographic data, such as age and gender, together with the ART history for each individual were obtained using a self-reporting questionnaire. Five milliliters of blood was collected from each participant and tested for anti-HIV-1 antibodies using Unigold (Trinity Biotech, NY) and Determine (Abbott, IL). HIV-1 antibody positivity was further confirmed by enzyme-linked immunosorbent assay (ELISA) (Enzygnost, Dade
Baseline CD4+ T cell counts were performed using a FACSCalibur flow cytometer (Becton-Dickinson, NJ). Individual test results were reviewed to confirm the accuracy of the analysis. Baseline viral loads were determined using Nuclisens EasyQ (Biomérieux, Marcy l'Etoile, France), with a lower limit of quantitation of 50 (1.69 log10) copies/ml of plasma, according to the manufacturer's instructions. This was done at baseline and follow-up as necessary.
Peripheral blood mononuclear cells (PBMCs) were obtained from 5 ml of blood by Ficoll-Hypaque density gradient centrifugation. Proviral DNA was extracted from uncultured PBMCs using DNAzol lysis and ethanol precipitation. Nested polymerase chain reaction (PCR) amplification was performed using AmpliTaq DNA polymerase (Roche Molecular Systems, Branchburg, NJ). Segments of the HIV-1 reverse transcriptase (RT), gp41, and env-C2V3 regions corresponding to HIV-1HXB2 nucleotides 2480–3180, 7850–8310, and 6975–7520, respectively, were amplified as previously described. 9,10 Resulting amplicons were bulk-sequenced in the sense and antisense direction with a set of nested primers. All sequencing reactions were performed using an optimized assay on an automated ABI 3100 genetic analyzer machine as previously described. 11 Neighbor-joining phylogenetic trees, including reference sequences from the Los Alamos database, were constructed using Clustal W version 1.83 and then drawn using TreeView PPC, version 1.6.6 (Institute of Biochemical and Life Sciences, Scotland, UK). Bootstrap resampling (1000 data sets) of multiple alignments was performed to test the statistical robustness of the trees.
The predicted coreceptor usage of HIV-1 was determined based on the env-V3 loop amino acid sequences, where CCR5 (R5) and CXCR4 (X4) variants were identified according to (1) the 11/25 amino acid rule [uncharged residues at position 11 of V3 (mostly serine, S/glycine, G), negatively charged residues at position 25 (mostly glutamic acid, E/aspartic acid, D), and a net charge of the V3 loop less than +5 have been reported to predict CCR5 usage. Conversely, positively charged residues at position 11 or 25 (mostly arginine, R/lysine, K) and a net charge of the V3 loop equal to or more than 5 have been reported to predict CXCR4 usage, and (2) the net charge of the V3 region, which was calculated by subtracting the number of acidic amino acids (D and E) from the number of basic amino acids [lysine (K), histidine (H), and arginine (R)]. A net charge of equal to or less than +5 in the V3 region has been shown to predict CCR5 usage (R5 variants), whereas a net charge of more than +5 has been shown to predict CXCR4 usage (X4 variants). 12 In this study, a net charge of +5 or less was considered to predict an R5 phenotype. Genotypic drug resistance was defined as the presence of one or more resistance-related mutations, as specified by the consensus mutation figures of the International AIDS Society-USA. 6,13 The emergence of amino acid substitutions associated with resistance to RTIs and PIs has been characterized extensively, and these substitutions can be classified into major and accessory/minor (modifying) mutations. 13
In this preliminary analysis, it was found that 14 of 175 patients (8%) developed adverse events after 4 months on ART. All the patients had received ART for over 2 months as of August 2005 when samples for this study were collected. There was no statistically significant difference in HIV-1 RNA copy numbers and CD4+ T cell counts between those with (n = 14) and without (n = 161) IRIS (t test p values of 0.36 and 0.55, respectively). Baseline characteristics of all the patients are shown in Table 1.
IRIS, immune reconstitution inflammatory syndrome.
t-test.
Count for 158.
Count for 134 patients.
Of the 14 samples from suspected IRIS patients, sequence data showed the following HIV-1 subtypes among the patients: A1/A1/A1 (pol-RT/gp41/C2V3), 5; D/A1/A1, 1; A1/C/A1, 1; A1/D/A1, 2; D/D/D, 1; D/C/A1, 1; D/D/A1, 2; and D/A1/A2, 1. HIV-1 subtype A1 was the most prevalent. The virological and immunological characteristics of patients suspected of having developed IRIS are shown in Table 2. Phylogenetic trees for the HIV-1 RT, gp41, and env-C2V3 regions are shown in Fig. 1.

Neighbor-joining phylogenetic trees of HIV-1 reverse transcriptase (
Obtained at approximately 4 months after initiation of ART.
Paired t-test.
Twelve patients harbored viruses that are predicted to use chemokine coreceptor 5 (CCR5) whereas two had variant viruses predicted to use the CXCR4 coreceptor. The V3 amino acid sequence alignments, coreceptor usage, and predicted phenotype of the sequences are shown in Fig. 2.
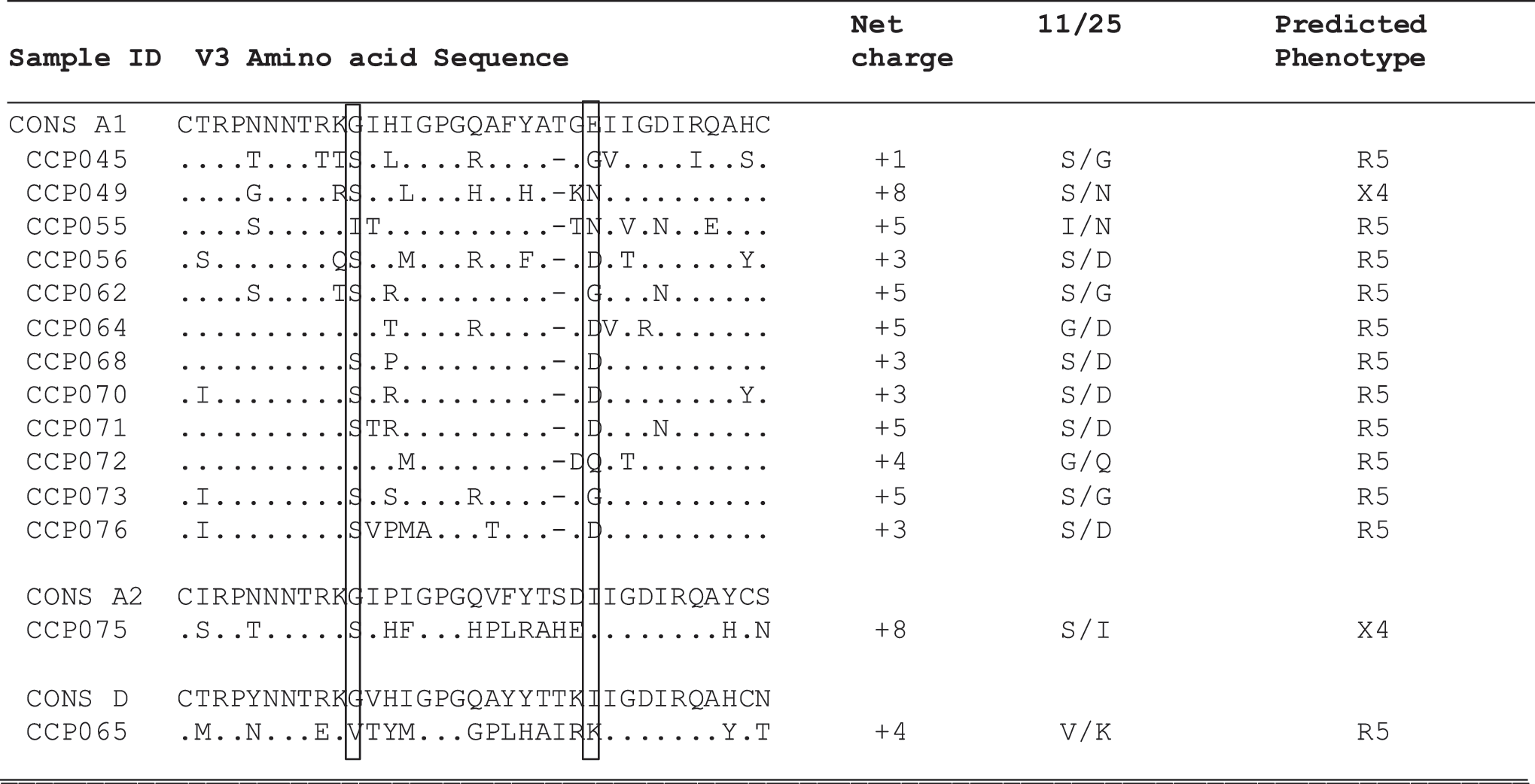
Coreceptor usage as determined genotypically from the HIV-1 env-C2V3 sequences. All letter designations for amino acids conform to the standard International Union of Pure And Applied Chemistry code. The consensus V3 amino acid sequence for each subtype is given in its entirety. Dot: identity with consensus amino acid; dash: gap inserted to maintain alignment. Replacements are indicated by appropriate code letters. Residues at positions 11 and 25 are boxed to highlight substitutions noted. The net amino acid charge of the V3 region was calculated by subtracting the number of negatively charged amino acids (D and E) from the number of positively charged ones (K, R, and H). CONS, consensus.
Analysis of the pol gene showed that three patients had viruses with major drug resistance-associated mutations. These included major NRTI mutations, M41L, K65R and NNRTI mutations, K101P, K103N from a 37-year-old male patient and D67N, K70R, K219Q together with L100I, K103N in a 28-year-old female patient. Other mutations observed were M184V and Y181C in a 25-year-old female patient (Table 3). There were no major PI resistance mutations. This reflected resistance to the current first line regimens alone.
NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitors. F, female; M, male. None, no resistance mutation was detected. Italics, minor mutations and/or polymorphisms with little or no effect on drug susceptibility.
In this study, 8% of study patients were suspected of having developed IRIS after initiation of ART. This was lower than the 20–25% that has been predicted in resource-poor settings, 14 in which patients initiated ART when CD4+ T cell count levels were too low (<200 cells/μl). This confirms findings that IRIS rarely occurs in persons starting ART with relatively high CD4+ T cell counts, i.e., >350 cells/μl. 15 Our study patients were initiated on ART at relatively higher CD4+ T cell counts (average 423 cells/mm3) and fairly high viral loads (average log10 4.46 copies/ml). This difference in outcome may be attributed to an awareness of available ART among infected individuals in our setting, which has been made easy through provision of free treatment. A general remarkable decrease in viral loads—baseline versus follow-up (p value = 0.0001)—and a drastic increase in CD4+ T cell counts (p value = 0.0157) were observed. Such drastic changes in immunological/virological parameters have been reported to be risk factors for IRIS. 15,16
In this study, major RTI-resistant mutants were detected in three patients. In particular, two patients had multiple NRTI drug resistance mutations. There were no major PI resistance-associated mutations found; only two polymorphisms, L10V and L24S, were found. Whereas L10V is a natural polymorphism associated with all available PIs, L24S is an atypical mutation. Because the first line ART in Kenya is a combination of two NRTIs (d4T and 3TC) and one NNRTI (NVP or EFV), most mutations, de novo or transmitted, would be associated with the widely available regimens. However, we did bulk sequencing of proviral DNA to investigate drug resistance mutations in the archived viruses, although the use of plasma viral RNA is the gold standard for drug resistance testing. This method, though reliable for detecting mutations in replication-competent virions in lymphocytes, may compromise the detection of a minor population of HIV-1 drug-resistant variants, which may exist in low copy numbers in some patients. Under such circumstances, detection of minor viral variants using more sensitive methods, such as allele-specific PCR, single-genome amplification, and clonal or deep sequencing, would be more ideal.
Our findings were particularly limited by the fact that no baseline drug resistance analyses were done before the start of ART; neither was baseline viral tropism determined. As such we could not elucidate whether the observed mutations were acquired or developed during therapy. However, in concordance with a report by Burman et al., 16 our sample size was small and was limited to the characterization of HIV-1 among suspected IRIS patients, i.e., we did not target IRIS as a primary endpoint and did not make much of a comparison between those with successful ART and those suspected of having IRIS. This is a subject of further research. Furthermore, the self-reporting system adopted in our setting might have compounded our findings as related to ART history and other therapies that the patients might have had prior to enrollment. Because of the nature of IRIS-associated infections, there is a need for more focused investigations into the syndrome, especially among the infected in resource-poor settings. This would be very important and is being considered in future analyses.
The HIV-1 subtypes among the patients studied were A, C, and D together with their related recombinants (Table 3), which is in agreement with previous findings in Kenya. 9,17 However, although we employed a commonly used subtyping methodology, the absence or presence of recombination in the analyzed gene fragments does not exclude the possibility of recombination elsewhere. Hence, we could have underestimated the proportion of patients harboring recombinant HIV-1. In terms of coreceptor usage, two patients had CXCR4 viral variants. Should resistance to available standard regimens emerge, the CXCR4 variants would pose difficulties in management as the patients harboring these viruses would not be eligible for the CCR5 antagonist—maraviroc—which is useful only in patients with CCR5 variants. However, the bulk sequencing methodology and genotypic determination of coreceptor use may be limited since some viral variants exist in low copy numbers, which would be better determined using more sensitive assays. In such circumstances, phenotypic assays would be more ideal.
In conclusion, this study characterized HIV-1 subtypes and drug resistance among individuals with suspected IRIS. However, the observed percentage of patients suspected of developing IRIS was low. The use of CXCR4 as a coreceptor has been associated with advanced/severe disease and it was therefore expected that most of the IRIS patients would harbor X4 variants. Furthermore, only three patients out of the 14 with suspected IRIS harbored resistant virus. Therefore, drug resistance may not be the sole cause of ART adverse events; other factors, including host genetic makeup and immunology, may be involved. There is a need for further studies to elucidate this. With increased molecular techniques in HIV research, there is a need to concurrently monitor and evaluate virological, immunological, as well as clinical causes and profiles of IRIS in the majority who, seemingly, harbor different HIV subtypes with different courses. HIV-1 characterization would be important before and during HIV therapy with envisaged treatment failure among patients who are increasingly presenting with diverse viral subtypes.
Sequence data
The sequences generated in this study were deposited at GenBank under the following accession numbers: pol: FJ599482–FJ599498, FJ599390–FJ599399; env-C2V3: FJ599374–FJ599378, FJ599381–FJ599389.
Footnotes
Acknowledgments
This work was carried out at the Kenya Medical Research Institute (KEMRI), Kenya. The study was funded by the Center for Virus Research/KEMRI. We thank the study participants for their invaluable support by consenting to the use of their samples in the study. Laboratory personnel in CVR, KEMRI played a key role in initial sample processing.
Author Disclosure Statement
No competing financial interests exist.