
Abstract
Etravirine (ETR) has previously shown potent in vitro activity against different primary HIV-1 isolates and demonstrated durable efficacy in treatment-experienced, HIV-1-infected patients in the Phase III DUET studies. The antiviral activity and efficacy of ETR against HIV-1 subtypes B and non-B were further investigated. The effect of HIV-1 subtype on ETR fold change in EC50 value (FC) was analyzed in HIV-1 recombinant clinical isolates from 673 treatment-naive patients enrolled in other Tibotec studies. Subgroup analyses from the DUET studies of the effect of HIV-1 subtype on the proportion of patients with viral load (VL) <50 HIV-1 RNA copies/ml were also conducted using pooled week 48 data. Genotype/subtype and phenotype determinations were performed using the vircoTYPE HIV-1 and Antivirogram assays, respectively. In vitro results from treatment-naive patients indicated comparable median ETR FC in virus isolates from patients infected with subtype B or non-B (1.1 vs. 1.2, respectively). HIV-1 subtype data were available for 594 and 595 patients in the ETR and placebo groups of the DUET studies, respectively; 94% of patients harbored subtype B. Baseline characteristics were similar across the different subtypes, with the exception of a higher number of sensitive NRTIs used in patients with subtype non-B. At week 48, virological responses in the ETR group were higher in patients with subtype non-B versus B (73% vs. 60%, respectively). ETR was equally effective in suppressing viral replication in patients infected with HIV-1 subtype B or various HIV-1 non-B subtypes.
H
The present exploratory analysis was undertaken to examine the antiviral activity and clinical efficacy of ETR in various HIV-1 subtypes. Antiviral activity was investigated using a panel of recombinant clinical isolates from treatment-naive subjects coming from different geographic origins to provide additional insight into the natural distribution of phenotypic susceptibility (i.e., in the absence of acquired resistance-associated mutations) of the different HIV-1 subtypes to ETR. The clinical efficacy of ETR in different HIV-1 subtypes was also explored using the pooled data from the DUET studies.
DUET-1 and DUET-2 (TMC125-C206 and TMC125-C216) are two randomized, double-blind, placebo-controlled, global Phase III studies that evaluated the efficacy, tolerability, and safety of ETR when given with a background regimen (BR) in treatment-experienced, HIV-1-infected patients. Patients were randomized 1:1 to ETR [200 mg twice daily (bid)] or placebo, both in combination with a BR of darunavir (DRV) with low-dose ritonavir (DRV/r), investigator-selected nucleoside reverse transcriptase inhibitors (NRTIs), and optional enfuvirtide (ENF). 6,7 The DUET-1 and DUET-2 analyses showed that ETR-based antiretroviral (ARV) treatment provided significant and durable improvement in virological and immunological parameters, compared with placebo, after 48 weeks of therapy in treatment-experienced patients. 8,9 In the pooled DUET analysis, 61% of patients in the ETR + BR group achieved undetectable viral load [<50 HIV-1 RNA copies/ml, time-to-loss of virological response imputation algorithm (TLOVR) 10 ] vs. 40% in the placebo + BR group. 11
Exploratory subgroup analyses were conducted to assess the effect of the subtype of HIV-1 on the proportion of patients with viral load <50 HIV-1 RNA copies/ml (TLOVR). Genotype and phenotype determinations were performed using the vircoTYPE HIV-1 and Antivirogram assays (Virco, Mechelen, Belgium), respectively. HIV-1 subtype was determined by Virco as the best match between the protease/reverse transcriptase nucleotide sequence and the corresponding subtype consensus sequences from the LANL subtype reference subset. 12 The number of patients infected with subtype non-B was small (and did not allow powerful and/or precise statistical analyses). Results were interpreted using the ETR clinical cut-offs (CCOs), previously described by Peeters et al. 13
In vitro phenotyping was performed on a panel of HIV-1 recombinant clinical isolates from treatment-naive patients (n = 673) infected with different HIV-1 subtypes. The distribution of subtypes in this panel included 47% HIV-1 subtype non-B comprising 18% C, 16% AE, 4% A1, 3% BF, 2% AG, 1% F1, and 3% others. The in vitro results showed a comparable median ETR FC in isolates from treatment-naive patients infected with either subtype B: 1.1 (interquartile range 0.8–1.6) or non-B: 1.2 (interquartile range 0.8–1.7), with no difference between the non-B subtypes. Furthermore, the 95th percentile remained below the lower CCO for ETR (FC ≤ 3), irrespective of HIV-1 subtype (Fig. 1).
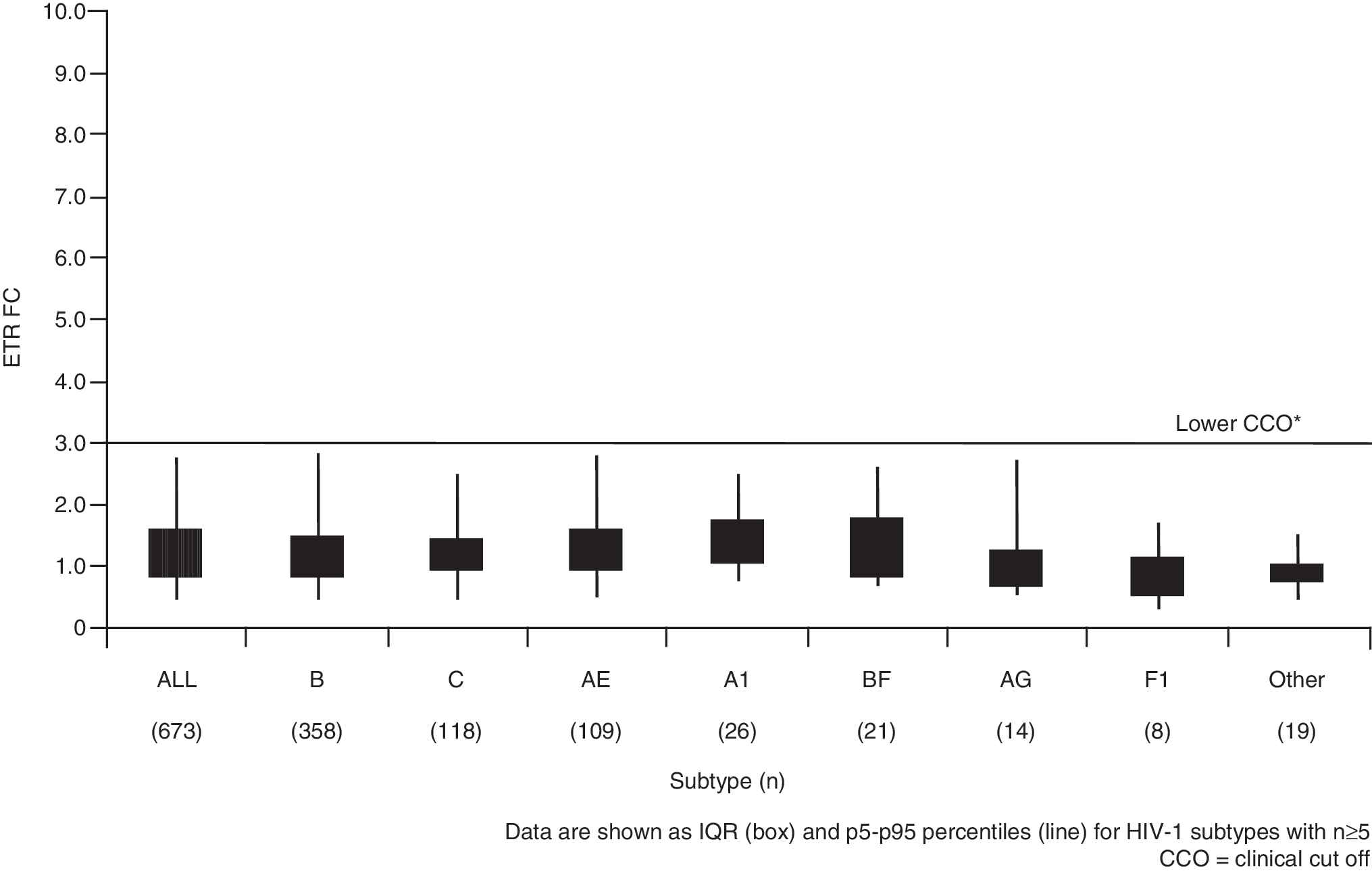
Fold change in EC50 values for etravirine in B and non-B subtypes from treatment-naive HIV-1 recombinant clinical isolates. Data are shown as IQR and p5–p95 percentiles (line) for HIV-1 subtypes with n ≥ 5. *CCO, clinical cut-off.
Pooled DUET HIV-1 subtype information was available for 594 and 595 patients in the ETR and placebo arms, respectively. The majority of these (93.8%) harbored HIV-1 subtype B (Table 1). Among the non-B subtypes, BF (2.1%), F1 (1.2%), and AG (0.8%) were most prevalent. Baseline disease characteristics [viral load, CD4+ cell count, ETR fold-change in 50% effective concentration (FC) and DRV FC] were similar between patients with different subtypes, except for a higher number of sensitive ARVs among those with HIV-1 subtype non-B, either by phenotypic sensitivity score (PSS) or by nucleoside (nucleotide) reverse transcriptase inhibitor (N[t]RTI) sensitivity only (Table 1) in both arms of the study. Of note, the number of sensitive NRTIs used in the BR was not a significant predictor of response in the ETR + BR group. 14
Note that patient numbers are small; n for other non-B subtypes is too small for individual data to be shown; p-values were not calculated due to small patient numbers for subtype non-B.
For the PSS calculation, DRV was considered as fully sensitive if FC ≤ 10. NRTIs were considered sensitive if the FC was ≤ cut-off used in the Antivirogram assay. ENF was considered sensitive if used de novo. ETR was not included in this calculation.
ETR, etravirine; BR, background regimen; FC, fold-change in 50% effective concentration; DRV, darunavir; PSS, phenotypic sensitivity score; ENF, enfuvirtide.
For ETR + BR versus placebo + BR, respectively, virological responses (<50 HIV-1 RNA copies/ml) at week 48 were 60% (336/561) vs. 40% (219/554) for HIV-1 subtype B and 73% (24/33) vs. 39% (16/41) for HIV-1 subtype non-B (Table 2). Virological responses at week 48 in the most prevalent non-B HIV-1 subtypes (i.e., BF, F1, and AG) were also investigated, with the caveat that these patient subgroup numbers were small (Table 2). For ETR + BR versus placebo + BR, respectively, virological responses were 69% (9/13) vs. 42% (5/12) for BF, 40% (2/5) vs. 22% (2/9) for F1, and 83% (5/6) vs. 67% (2/3) for AG. Taken together, these results suggest that the additional contribution of ETR on virological response as compared to placebo was similar in patients infected with HIV-1 subtype B or various HIV-1 non-B subtypes.
Note that patient numbers are small; n for other non-B subtypes is too small for individual data to be shown; p-values were not calculated due to small patient numbers for subtype non-B. ETR, etravirine; BR, background regimen.
Recently, a weighted genotypic score was developed for ETR using data from the DUET studies. 15 Briefly, each mutation known to be associated with reduced virological response to ETR and/or increased ETR FC was assigned a relative weight factor according to its effect on response and/or FC. These relative weight factors were then summed for all patients to give the weighted score. Weighted scores of 0–2, 2.5–3.5, and ≥4 are associated with highest, intermediate and reduced response rates, respectively. In the present analysis patients in both treatment groups with weighted score <4 achieved the highest response rate (Table 2). Of note, the high virological responses generally observed in the ETR-treated patients with non-B subtype were also evident when the results were analyzed by weighted genotypic score.
In the analysis of phenotypic susceptibility to ETR among a large collection of HIV-1 subtypes B and non-B recombinant clinical isolates from treatment-naive patients, comparable median ETR FC values were observed in both groups. These results provide additional insight into the natural distribution of phenotypic susceptibility of different HIV-1 subtypes to ETR. In addition, based on the pooled results from the DUET studies, ETR appears to be equally effective in suppressing viral replication in patients infected with HIV-1 subtype B or various HIV-1 non-B subtypes with the caveat that the number of patients infected with subtype non-B was small. Additionally, many of the non-B isolates were subtype BF and could be similar to subtype B in the RT region of the pol gene.
Furthermore, the virological response rates were highest among ETR-treated patients (both HIV-1 subtype B and non-B strains) with a baseline weighted genotypic score of <4. Except for a higher number of sensitive ARVs used in those with HIV-1 subtype non-B in both treatment arms, baseline disease characteristics were similar between patients infected with the different HIV-1 subtypes. A higher number of sensitive ARVs could in part explain the numerically higher response rates observed in patients with HIV-1 non-B infection in the ETR + BR arm.
When combining the in vitro susceptibility data and the DUET efficacy data these findings confirm that ETR is active against both HIV-1 subtype B and the tested non-B isolates.
Footnotes
Acknowledgments
DUET-1 and DUET-2 are registered with
Author Disclosure Statement
The author received medical writing support from Gardiner-Caldwell Communications (GCC) Ltd, Macclesfield, UK, which was funded by Tibotec Pharmaceuticals Ltd. All authors are employees of Tibotec Pharmaceuticals Ltd.