
Abstract
The emergence and spread of transmitted drug resistance (TDR) poses a major threat to the success of the rapidly expanding antiretroviral treatment (ART) programs in resource-limited countries. The World Health Organization recommends the use of the HIV Drug Resistance Threshold Survey (HIVDR-TS) as an affordable means to monitor the presence of TDR in these settings. We report our experiences and results of the 2007 HIVDR-TS in Botswana, a country with one of the longest-existing national public ART programs in Africa. The HIVDR-TS and HIV-1 incidence testing were performed in the two largest national sites as part of the 2007 antenatal Botswana Sentinel Survey. The HIVDR-TS showed no significant drug resistance mutations (TDR less than 5%) in one site. TDR prevalence, however, could not be ascertained at the second site due to low sample size. The agreement between HIVDR-TS eligibility criteria and laboratory-based methodologies (i.e., BED-CEIA and LS-EIA) in identifying recently HIV-1 infected adults was poor. Five years following the establishment of Botswana's public ART program, the prevalence of TDR remains low. The HIVDR-TS methodology has limitations for low-density populations as in Botswana, where the majority of antenatal sites are too small to recruit sufficient numbers of patients. In addition, the eligibility criteria (age <25 years and parity (first pregnancy)) of the HIVDR-TS performed poorly in identifying recent HIV-1 infections in Botswana. An alternative sampling strategy should be considered for the surveillance of HIVDR in Botswana and similar geographic settings.
Introduction
A
In order to monitor the emergence of transmitted drug resistance (TDR) in resource-limited countries, the WHO has proposed the HIV drug resistance threshold survey (HIVDR-TS), which categorizes transmitted drug resistance as low (less than 5%), medium (5–15%), or high (greater than 15%). 7,8 The HIVDR-TS has been recommended for use in small geographic areas where at least 20% of combination ART (cART)-eligible HIV-infected adults have been receiving cART for more than 3 years. The methodology is based on binomial sequential sampling of up to 47 eligible samples. It is recommended that the HIVDR-TS be incorporated in well-established HIV antenatal sentinel surveillance activities, using the following three mandatory eligibility criteria: HIV seropositive status, age (<25 years), and parity (no prior pregnancy). As long-term HIV infection or previous ARV drug exposure might confound or mask the diagnosis of transmitted drug resistance, additional criteria, when routinely available, are also recommended, such as documented laboratory evidence of seroconversion or recent infection, a CD4+ cell count greater than 500 cells/mm, 3 no evidence of WHO clinical stage 3 or 4 events, and/or no known prior exposure to ARV medications. Several countries have conducted HIVDR-TS surveys within existing HIV-1 antenatal sentinel surveillance monitoring using mandatory eligibility criteria. 9 –15 The use of laboratory-based evidence of recent infection as eligibility criteria has not been reported in antenatal sentinel surveillance.
Botswana, a sparsely populated country (1.7 million inhabitants) and a high HIV-1 prevalence rate (17.1% among the general population based on the 2004 Botswana AIDS Impact Survey 16 ) began offering public ART to qualifying citizens in January 2002. As of mid-2007, 92,000 of approximately 110,000 patients ever registered in the national ARV treatment program were actively receiving ART. The vast majority of cART-treated adults were receiving the following first-line ART regimens as recommended by existing national guidelines: zidovudine (ZDV), lamuvidine (3TC) plus efavirenz (EFV) for men and all women not having reproductive potential, and zidovudine (ZDV), lamuvidine (3TC) plus nevirapine (NVP) for women with childbearing capacity. In 2007, Botswana included in its national HIV-1 antenatal sentinel survey both the HIVDR-TS and HIV-1 incidence estimation using HIV-1 BED Incidence EIA® (BED-CEIA) and Vironostika® Less Sensitive (LS-EIA) HIV EIA methodology. We herein report our experiences and results from the use of the HIVDR-TS as well as laboratory-based HIV-1 incidence estimations in Botswana in 2007.
Methods
Study population
In Botswana, national HIV-1 antenatal sentinel surveillance has been performed annually through 2007. According to the national protocol, 17 during a period of 12 weeks, all pregnant women were eligible who registered for routine antenatal care at pre-specified clinics. These clinics were selected based on the number of patients presenting for care (clinic volume). Sociodemographic data were collected and residual blood samples from routine antenatal clinic (ANC) syphilis testing were utilized as per established unlinked, anonymous testing policy.
In 2007, routine sentinel surveillance was supplemented by two additional surveys, namely the HIVDR-TS and HIV-1 incidence testing. In short, all sentinel surveillance samples were tested for HIV-1 using the parallel ELISA strategy (Murex® and Vironostika®) as recommended by the Botswana Ministry of Health HIV testing guidelines. Incidence testing using the BED-CEIA and LS-EIA was performed on all HIV-1 positive samples. Prevalence of transmitted drug resistance (TDR) was estimated in two sites, namely Francistown and Gaborone, as these sites are Botswana's two largest cities, serving close to 400,000 persons or approximately 25% of the country's population. In addition, these sites were established in 2002, and as of early 2007, at least 80% of cART-eligible HIV-1 infected persons were receiving cART at these sites. Approximately 22,000 total patients had been receiving cART for a minimum of 2 years at these two large urban sites.
Study procedures
An aliquot of plasma from anonymized sentinel surveillance participants at the two sites was sent within 24 hours of sampling to the national Botswana–Harvard HIV Reference Laboratory (BHHRL) in Gaborone where it was stored at −70°C. The HIVDR-TS protocol as recommended by the WHO 18 was followed to estimate TDR prevalence. In summary, women were included if they fulfilled the three mandatory criteria: (1) HIV-1 EIA positive, (2) less than 25 years of age, and (3) pregnant for the first time, and in addition were ARV-naïve as self-reported in the sentinel surveillance questionnaire.
Laboratory methods
HIV-1 genotypic drug resistance testing and analyses
Eligible samples were listed consecutively. HIV-1 genotypic drug resistance testing was performed using a broadly sensitive in-house genotyping protocol at the International Laboratory Branch, Division of Global AIDS, National Center for HIV/AIDS, Hepatitis, STD, and TB Prevention (NCHHSTP), Centers for Disease Control and Prevention (CDC), Atlanta, GA, USA. 19 Transmitted HIV-1 drug resistance mutations were determined by Calibrated Population Resistance (CPR) version 4.1 beta using the Stanford HIV Drug Resistance Database. 20 The binomial sequential sampling and classification table was used to categorize the prevalence of HIV-1 drug resistance as specified in the protocol.
Phylogenetic analysis
Generated pol nucleotide sequences were aligned using Muscle 21 with HIV-1 subtypes references from the Los Alamos HIV Sequence Database, 22 followed by a BioEdit 23 manual adjustment. The evolutionary model was selected by using the Akaike information criterion in jModeltest 0.1.1. 24 The parameters of the model (GTR+ v + Γ) were as follows: nucleotide frequencies fA = 0.4225, fC =0.1645, fG = 0.1838, and fT = 0.2291; estimated value of shape parameter α of the Γ distribution = 0.7590; estimated value of proportion of invariable sites = 0.3720; and R matrix values RA↔C = 1.9835, RA↔G = 8.2960, RA↔T = 0.8602, RC↔G =0.8400, RC↔T = 11.2101, and RG↔T = 1.0. The identified substitution model was used in PhyML 25 to reconstruct the genealogy of analyzed pol sequences. The maximum likelihood tree was visualized in MEGA v4. 26 The approximate Likelihood-Ratio Test (aLRT) was used as a statistical test to compute branch supports. The aLRT branch support was significant when it was larger than 0.90. The evolutionary history was also inferred by the Neighbor-Joining method 27 using the Kimura 2-parameter method 28 in MEGA4. 26 The bootstrap test (100 replicates) was used to support branching topology. 29 The bootstrap values of 80 and higher were considered significant. A total of 39 HIV-1 subtype references from Los-Alamos HIV Sequence Database were represented by four A1 sequences, two A2's, five B's, four C's, four D's, four F1's, four F2's, four G's, three H's, three J's, and two K's. Three CPZ sequences were used as an outgroup. The recombination analysis was performed by SimPlot. 30
Determination of “recent” HIV-1 infections
All samples that tested HIV-1 positive in the sentinel survey were additionally tested for recent HIV-1 seroconversion using (1) BED-CEIA (HIV-1 BED Incidence EIA®, Calypte Biomedical Corporation, Portland, OR) 31 and (2) LS-EIA (Vironostika Microelisa System®, bioMérieux, Durham, NC). 32 Patients were considered recently infected if, using the BED-CEIA technique, the normalized optical density (ODn) was less than 0.8, or if, using the LS-EIA technique, the standardized optical density (SOD) was less than 1.0.
Definitions
For the purpose of this study, a participant was defined as recently HIV infected when (1) the HIV-1 EIA test was positive, (2) the BED-CEIA or LS-EIA indicated recent infection as defined above, and (3) the participant reported that he/she was not taking antiretroviral therapy in the sentinel survey questionnaire.
Statistical methods
Agreement between HIVDR-TS eligibility criteria and BED-CEIA or LS-EIA test results were measured using concordance (percent agreement) (i.e,, the proportion of all participants with concordant results), and κ-statistic (i.e., an index comparing the observed agreement versus what might be expected by chance).
Ethical approvals
The study was approved by the Human Research and Development Committee of the Ministry of Health, Botswana. The Human Subjects Committee of the Harvard School of Public Health determined that the study qualified for “exemption” status based on fulfilling the definitions of such research as set forth in the United States code of federal regulations, Section 45 CFR 46.101(b). 4
Results
Between July 9th and September 28th, 2007 (12 weeks), 264 health facilities (28 hospitals and 236 clinics) from all 24 Botswana health districts took part in the national HIV-1 sentinel surveillance. Out of a total of 7814 collected samples, 7726 samples (98.9%) were evaluable for analysis (Fig. 1). Overall, 2705 (35.0%) of 7726 samples tested HIV-1 positive. The HIV-1 prevalence rate was 19.9% (537 of 2705) among women experiencing their first pregnancy and 32.9% (891 of 2705) among women less than 25 years of age. Both criteria were met by 14.2 % (385 of 2705) women. 492 (18.2%) of 2705 patients testing HIV-1 EIA positive reported they were taking ART and were thus excluded from the formal analysis.

Botswana 2007 sentinel surveillance samples and associated HIV status and age/parity characteristics.
HIV-1 subtyping
To determine HIV-1 subtype, newly generated pol sequences were genotyped. The maximum likelihood tree is presented in Fig. 2. A total of 71 out of 72 sequences clustered with HIV-1 subtype C references providing evidence that 98.6% of analyzed pol sequences belong to HIV-1 subtype C. Viral sequence from one participant, B0604, clustered with HIV-1 subtype J reference sequences, but branching topology did not support pure subtype J. The follow-up analysis by SimPlot 30 provided evidence that this pol sequence represents a complex recombinant between HIV-1 subtype J and K. Analysis by the Neighbor-Joining method produced similar results (data not shown).
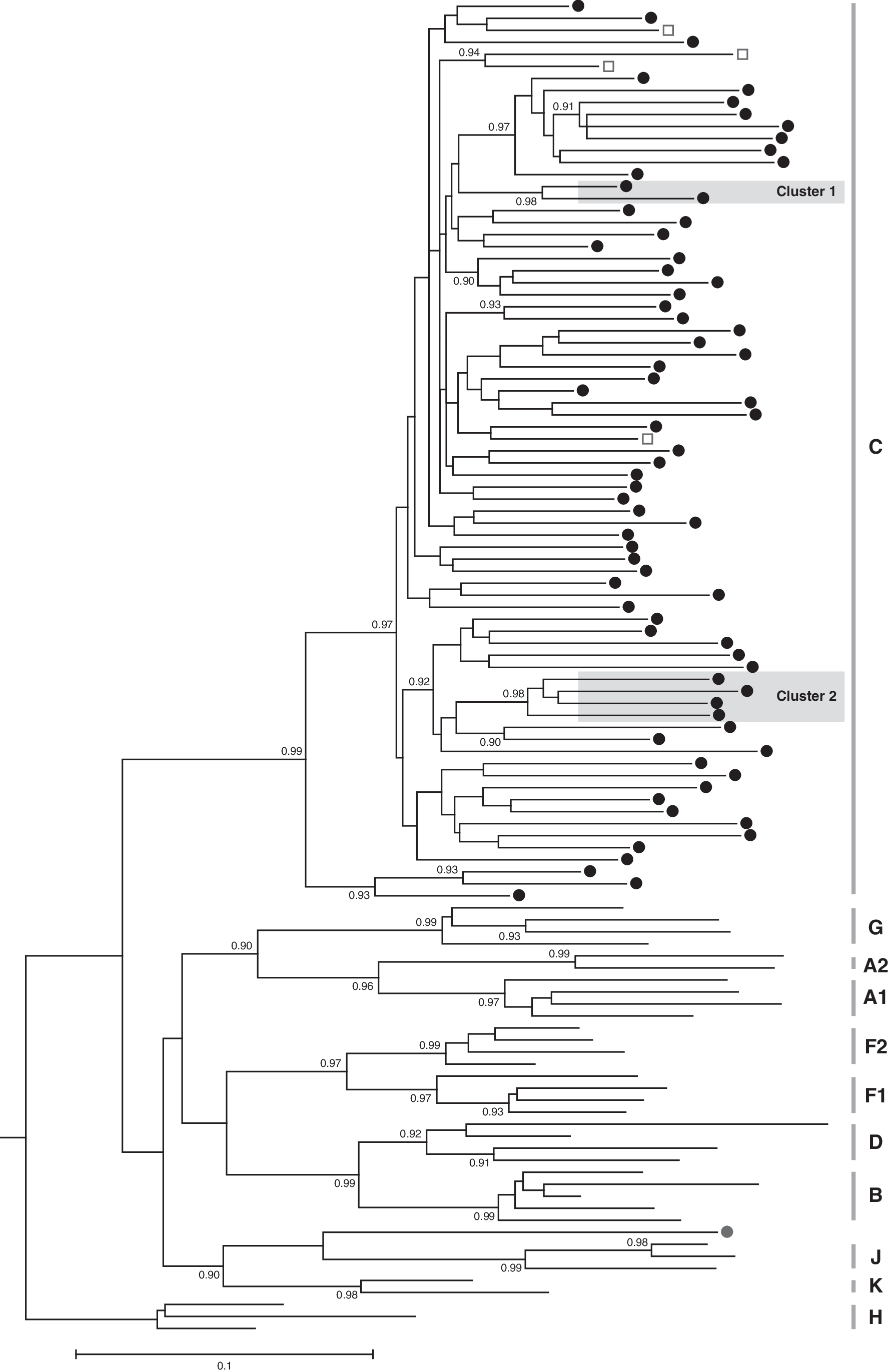
Phylogenetic relationships of 72 pol sequences generated in the study. Maximum likelihood tree is shown with branching support of aLRT (only values over 0.90 are shown). A total of 71 newly generated sequences that cluster with HIV-1 subtype C references are shown by dark circles. HIV-1 subtype C references are indicated by open blue squares. A complex recombinant virus between HIV-1 subtypes J and K is shown by red circle at the bottom of the tree. Two clusters of new pol sequences with aLRT support of 0.98 are highlighted by gray rectangles.
Cluster analysis
Phylogenetic analysis of newly generated pol sequences revealed clusters supported by high aLRT values. As shown in Fig. 2, two clusters within HIV-1 subtype C are supported by aLRT values of 0.98 and higher: one cluster includes two sequences each, while cluster 2 includes four sequences. The same four sequences clustered in the tree inferred by the Neighbor-Joining tree with bootstrap support of 90 (data not shown). It is likely that high aLRT and bootstrap support of branching topology indicates HIV-1 transmission cluster in the local epidemic in Botswana.
2007 HIVDR-TS
The two largest sentinel surveillance sites, Gaborone and Francistown, identified 264 and 225 HIV-1 positive specimens, respectively (Table 1).Of these, 44 (16.7%) and 42 (18.7%) patients, respectively, met the eligibility criteria for HIVDR-TS testing as specified by the WHO.
One sample contained multiple NRTI and NNRTI drug resistance mutations.
39 (88.6%) of the 44 samples from Francistown and 33 (78.6%) of the 42 samples from Gaborone could be genotyped. One sample showed multiple NRTI and NNRTI drug resistance mutations and after case review was classified as acquired drug resistance. No significant drug resistance mutations were identified from the other 71 evaluable subjects. Amino acid substitutions which were deemed to be clinically insignificant were found within the reverse transcriptase gene at position 179 (V179I 1 ) and within the protease gene at positions 23 and 82 (V82I 2 , L23F 1 ).
According to HIVDR-TS protocol, the prevalence of TDR was less than 5% in Francistown; the prevalence in Gaborone could not be determined as the required minimum of 34 samples for genotypic analysis was not attained.
Determination of recent infections using BED-CEIA and LS-EIA
All HIV-1 positive sentinel surveillance samples were tested using the BED-CEIA and LS-EIA methodologies. From a total of 467 patients satisfying BED-CEIA criteria for recent infection, 37 were from Gaborone and 40 from Francistown. Of a total of 265 samples meeting V-LS criteria for recent infection, 24 came from Gaborone and 24 from Francistown.
Association between HIVDR-TS criteria compared to BED-CEIA and LS-EIA
The agreement between the HIVDR-TS criteria (less than 25 years of age and first pregnancy) and BED-CEIA and between HIVDR-TS criteria and LS-EIA was marginal, namely (K = 0.16, 95% CI = 0.11–0.2; concordance = 77.0%) and (K = 0.14, 95% CI = 0.09–0.19; concordance = 81.7%), respectively (Table 2).
Number of samples with available information on both lab-based incidence results and HIVDR-TS eligibility criteria.
Kappa statistic (κ) and concordance (c): measures of agreement between HIVDR-TS and laboratory-based criteria.
Discussion
Botswana has one of the longest-established public national ART programs in sub-Saharan Africa and the development and propagation of transmitted drug resistance is considered to be the major threat to the success of this ambitious initiative. The 2007 Botswana HIVDR-TS survey completed in one of the largest urban national sites indicated that 5 years following the rapid, countrywide ART rollout, TDR was still very low, that is, less than 5% according to the HIVDR-TS protocol. 33 No major drug resistance mutations as defined by the consensus list of surveillance drug resistance mutations compiled by an expert panel from the WHO were detected. 34,35 While these data from one single health district should not be extrapolated to the entire country, they are consistent with projections made by Vardavas and Blower, 36 who had modeled the evolution of TDR in Botswana and predicted that TDR was unlikely to exceed the WHO threshold by 2009, even while assuming (1) a relatively high rate of acquired drug resistance of 20% per year, and (2) a 50% reduced fitness of the transmitted virus. Botswana-specific data concerning these two key determinants of TDR are scarce. Program data on the level of acquired drug resistance are also not available, as genotypic resistance testing is not routinely performed at the time of first-line regimen failure.
Phylogenetic analysis in this study confirmed previous reports that a vast majority of HIV-1 infections in Botswana are caused by HIV-1 subtype C. Of 72 genotyped individuals, 71 (98.6%) were infected with HIV-1 subtype C, while one participant was infected with a complex HIV-1 J/K recombinant.
Excellent 5-year virologic outcomes have been reported from the largest ART site in Botswana. 3 Little is known about the fitness of drug-resistant strains for HIV-1C. A recent report 37 on increased fitness of viruses with specific thymidine analogue mutations (TAMs) among subtype C ART-treated adults, however, is of concern. To improve the understanding of the dynamics of TDR in Botswana, consistent longitudinal monitoring of actual prevalence of TDR and acquired drug resistance rates is needed. In addition, transmitted viral strains need to be characterized in regard to replicative capacity and the presence of minor variants.
In contrast to acquired drug resistance, transmitted drug resistance needs to be analyzed as close to the transmission time as possible as the drug-resistant virus can gradually be replaced by drug-sensitive wild-type virus until ultimately drug-resistant variants will not be detected by conventional population sequencing while persisting as archived virus. 38,39 It is, however, a significant challenge, especially in resource-limited settings, to identify individuals routinely with acute/recent HIV-1 infections. The mandatory HIVDR-TS eligibility criteria recommend the inclusion of young women (less than 25 years of age) in their first pregnancy based on the assumption that these women will be early in the course of their HIV-1 infection. The WHO protocol, however, also recommends that additional criteria can be used to avoid inclusion of persons with acquired drug resistance and/or with long-established HIV infection. Such additional criteria, where routinely available, include history of ARV medication exposure and criteria that assist in estimating the duration of HIV infection (e.g., laboratory, immunological and/or clinical data).
As the 2007 Botswana antenatal sentinel survey had incorporated the HIVDR-TS while collecting additional information on ARV medication exposure and HIV-1 incidence, we wanted to explore the effect of these additional measures on the number of eligible women and determine the degree of agreement between these methods. The relatively poor concordance of the “mandatory” age/parity criteria with either of the two laboratory-based methods, namely BED-CEIA and LS-EIA, was partly explained by the intrinsic difference in case definition and in population size between these criteria. The case definition for laboratory-based criteria is determined by the relatively narrow time interval inherent in the assay methodology (window period), while the case definition for demographic criteria extends to all young (less than age 25) HIV-1-infected women experiencing their first pregnancy irrespective of the duration of infection. The population size which is screened by these criteria also differs (e.g., laboratory-based screen all HIV-positive cases while demographic restrict eligible cases to a subpopulation defined by age and parity). Our results show that the number of eligible samples did not significantly change when persons were enrolled based on laboratory criteria compared to the mandatory WHO criteria. This could be expected as a recent infection by laboratory standard refers to a relatively smaller time interval (i.e., largely the window period of the assay), compared to a potentially “much less recent” (established) infection that is identified by sociodemographic definition (i.e., age less than 25 years and first pregnancy). Of note, the laboratory-based methods detected a substantial number of recent infections that were not identified using mandatory criteria only. Interestingly, an acute HIV-1 infection study done in Botswana in 200719 found that women seroconverted at a median age of 26.0 years, which suggests that focusing on women less than 25 years of age in our setting may preclude the proper identification of a significant number of recently infected females. Overall, laboratory-based criteria did not alter the number of eligible samples for the HIVDR-TS, but these samples were probably more informative for the estimation of transmitted drug resistance as they were derived from a population of recent infections.
The accuracy of the laboratory-based methods used in this study, namely BED-CEIA and LS-EIA, is affected by a number of factors, including the individual variation in the immune response, the impact of late disease and antiretroviral therapy on anti-HIV antibody concentrations 40 –43 and the effect of the HIV subtype on the antibody response. 44,45 For the identification of individuals with recent infections no single currently available test is sufficient and additional information excluding a long-standing infection is necessary. 46,47 For HIV incidence estimation at population level the application of correction factors 48 –50 have been proposed to adjust for the small proportion of infections in the population that are misclassified as ‘recent’ by the BED-CEIA. Latest advances in the field suggest and support the use of algorithms based on multiple methods and/or including confirmatory steps for refining a screening result. 45,51 –53
One of the main advantages of the HIVDR-TS is the relatively small number of eligible participants (34–47 successfully genotyped samples) who, according to protocol, should be recruited from a small, circumscribed geographical area. 1 Botswana and possibly other countries in the region that are actively scaling up public ART programs, yet have small, highly mobile and geographically dispersed populations, face significant limitations and may find it difficult to identify sufficient numbers of cases. According to the Botswana 2007 sentinel survey, only one sentinel survey site could enroll a sufficient number of eligible women for the HIVDR-TS protocol. Similar observations were made during the Botswana 2005 sentinel survey, despite the fact that young ages were oversampled (i.e., enrollment of 15- to 24-year-olds continued during the surveillance period even after reaching the expected sampling size). 15,54 This sample size problem will be even further aggravated in the future as successful regional national ART programs decrease overall HIV-1 transmission rates at the population level and thereby lead to even greater reductions in the numbers of acutely/recently infected individuals. 55,56
Our experiences with TDR surveillance among a low-density population with high mobility such as Botswana suggest that an alternative drug resistance surveillance approach be considered which (1) uses available and accepted lab-based methodology/algorithm for the identification of recent HIV-1 infections and (2) considers all nationally identified recent infection samples as a basis to calculate the overall prevalence of transmitted drug resistance. Alternative algorithms including confirmatory tests and laboratory analysis for widely used ARVs might be necessary for reliable monitoring of HIV-1 TDR. Adopting such an approach may be more costly due to the higher number of genotypic resistance tests that need to be performed, but this can be justified given that it will generate important information on the evolution of TDR in the country.
Footnotes
Acknowledgments
The authors acknowledge the Botswana Ministry of Health, the Botswana–USA Collaboration, the Botswana–Harvard AIDS Institute, and the World Health Organization, Botswana, for their support and advice in conducting the sentinel surveillance activities. We also thank all staff members in the participating antenatal clinics and laboratories.
Author Disclosure Statement
No competing financial interests exist.