
Abstract
Parathyroid hormone (PTH) elevations are associated with reduced bone mineral density and adverse health outcomes and have been reported in patients with HIV infection. We aimed to examine the impact of vitamin D status and tenofovir (TDF) use on PTH levels among HIV-infected patients receiving combination antiretroviral therapy (cART). Demographics, medication and supplement use, and clinical data, including 25-hydroxyvitamin D [25(OH)D] and PTH, were collected on 45 HIV-infected men on ART. Suboptimal vitamin D status was defined as 25(OH)D < 30 ng/ml. The relationship between antiretroviral agents, suboptimal 25(OH)D, and PTH levels was examined. Among subjects with suboptimal vitamin D status, PTH values greater than or equal to the ULN (87 pg/ml) were more common among TDF users than nonusers: 41% versus 0% (p = 0.018); and median PTH was higher in TDF users: 80 pg/ml versus 55 pg/ml (p = 0.02). Among TDF users, PTH was higher in the group with suboptimal 25(OH)D (p = 0.045). Multivariable linear regression showed that PTH was independently and directly related to TDF use (p = 0.017) and inversely related to 25(OH)D (p = 0.017). PTH was not related to the estimated glomerular filtration rate (p = 0.9). In this cross-sectional study of HIV-infected men on ART, the use of TDF and the level of 25(OH)D were independently associated with PTH levels. Because TDF is a potent and widely used antiretroviral drug, information about cofactors that may exacerbate its side effects is of significant clinical value.
Introduction
HIV-
The etiology of bone disease among HIV-infected patients is unclear, but two recent studies indicate that PTH elevations play a direct role. PTH acts on bone to release calcium. Persistent PTH elevations are associated with bone loss across a range of clinical conditions. 6 It is thus striking that between 16.8% 7 and 40% 8 of HIV patients on antiretroviral medications have PTH levels above the upper limit of normal (ULN)—the level strongly associated with bone loss. In these studies, PTH elevations were observed in patients taking both nonnucleoside reverse transcriptase inhibitors (NNRTIs) and protease inhibitors (PIs). 7 Associations with TDF were not investigated.
Knowledge of the side effects caused by antiseizure medications (phenytoin) may provide insights into ART-mediated PTH elevations and bone loss. Bone loss in patients taking antiseizure medications is secondary to reduced absorption of dietary calcium. It is exacerbated by low vitamin D status, and can be mitigated by administering supplemental vitamin D and calcium. We hypothesized that absorption of dietary calcium is reduced in patients with low vitamin D status who are exposed to TDF and other cART agents that cause PTH elevations, bone loss, and increased bone remodeling. 3,5
Materials and Methods
This is a cross-sectional observational study using a convenience sample of 45 men receiving care from a single provider. Anthropometric measurements and blood pressure were determined. The medical record was reviewed. Subjects participated in a telephone interview and provided information on demographics, medical history, prescription medications, and over-the-counter medications and supplements. The study was approved by the Mount Sinai School of Medicine Institutional Review Board. Subjects provided written informed consent.
Biochemical testing for 25-hydroxyvitamin D [25(OH)D], PTH, and 1,25-dihydroxyvitamin D [1,25(OH)2D], and routine biochemical tests were performed. The Diasorin Liaison VD25 assay was used for 25(OH)D, the Diasorin Radioimmunoassay was used for 1,25(OH)2D, and the Siemens Centaur assay was used for HIV viral load testing (lower limit of detection of <50 copies/ml). Standard laboratory assays were used for routine biochemical tests. Corrected serum calcium was calculated by [0.8 × (normal albumin − patient's albumin)] + serum calcium; glomerular filtration rate (GFR) was estimated by the 4-variable Modification of Diet in Renal Disease equation. PTH was measured using the Siemens Immulite 1000 Intact Parathyroid Hormone assay. The ULN of this assay is 87 pg/ml. A recent investigation found that the Siemens Immulite Intact PTH assay is accurate. 9 Ninety-one percent of subjects had 25(OH)D and PTH measured on the same day; in 9% of cases there was a median separation of 10 days. Suboptimal vitamin D status was defined as 25(OH)D < 30 ng/ml, which is consistent with expert opinion. 6
The Mann–Whitney U test was used to analyze continuous variables and the χ2 test or Fisher's exact, used as appropriate, for dichotomous variables. Values of 25(OH)D below the lower limit of the assay, 7 ng/ml, were considered to be 3.5 ng/ml in calculations. The values of 25(OH)D and PTH from the most closely matched dates available were included in the analysis. Univariate linear regression was used to identify factors associated with PTH. The variables examined were age, race/ethnicity where “light-skinned” included subjects who self-identified as whites or white hispanic, 25(OH)D, 1,25(OH)2D, month and season of measurement, each individual highly active antiretroviral therapy (HAART) medication currently taken by any subject, use of vitamin D supplements, each class of HAART medication, diagnosis of hypertension, which was determined through medical record review, GFR, corrected calcium, systolic blood pressure, diastolic blood pressure, BMI, smoking status, and HIV disease status (time since HIV diagnosis, CD4+ T cells ≥350 cells/μl, CD4+ T cells >200 cells/μl). Multivariable linear regression was used to test all the variables that had a p ≤ 0.10 in the univariate analysis for their independent effect on PTH level. We also controlled for estimated GFR as this could be a confounder in the relationship between TDF use and the PTH level. The final model included GFR and variables that remained significantly associated with PTH. SPSS Version 16.0 was used. A p value ≤0.05 was considered significant.
Results
The median age was 49 years (IQR = 43, 55). Eighty percent were white. HIV infection was well controlled in most: 70% had ≥350 CD4+ T cells/μl and 77% had an undetectable HIV viral load. All were receiving cART, and 73% were taking tenofovir, all but one in combination with emtricitabine (FTC) (Table 1). Estimated GFR was above 60 ml/min/1.73 m2 in 91% of subjects. No subject had a GFR of <30 ml/min/1.73 m2, the cutoff below which impaired renal function is known to impact calcium/phosphorus handling. 10
Median (interquartile range).
Normal range.
N = 44.
Corrected calcium = [0.8 × (normal − patient's albumin)] + patient's calcium.
Among the 45 subjects, 37 (82%) had suboptimal vitamin D status. Low vitamin D status was more common among men who did not use vitamin D supplements daily (96% vs. 68% of those on supplements p = 0.02), but was not more common among TDF users than among subjects who did not use TDF (82% vs. 83% p = 1), indicating that vitamin D status was influenced by supplement use, but not by TDF use. In contrast to vitamin D status, PTH was strongly influenced by TDF use: PTH ≥ the ULN occurred in 11 of 33 (33%) TDF users and 0 of 12 non-TDF users (p = 0.023). Among TDF users, PTH was significantly higher in the 27 subjects with suboptimal 25(OH)D than in the six with optimal 25(OH)D (p = 0.045), emphasizing that both TDF use and vitamin D status influenced PTH values (Table 2).
Multivariate analysis included all variables with p ≤ 0.1 in univariate analysis and also controlled for GFR.
As determined by medical record review.
Bold indicates factors with p ≤ 0.05.
Among the 37 subjects with suboptimal vitamin D status, PTH levels were greater than or equal to the ULN in 11 of 27 (41%) TDF users, but in 0 of 10 non-TDF users (p = 0.018); PTH was 80 pg/ml in TDF users and 55 pg/ml in non-TDF users (p = 0.02). Despite the difference in PTH levels, neither 25(OH)D nor 1,25(OH)2D differed significantly between TDF users and non-TDF users (Fig. 1).
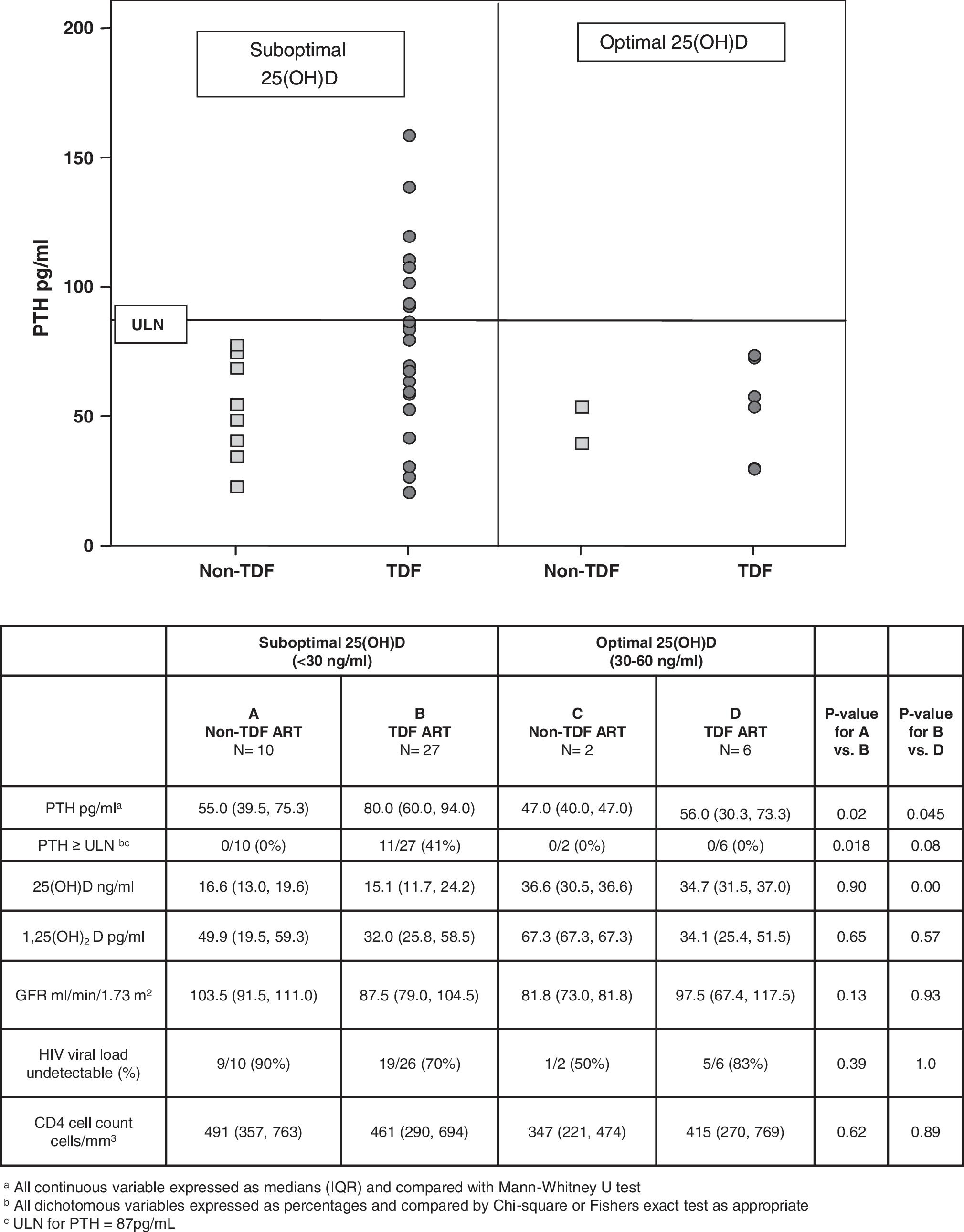
Vitamin D status and PTH in a group of HIV-infected men. Among 45 subjects on ART, PTH levels of subjects with suboptimal 25(OH)D levels were significantly higher in TDF users than in TDF nonusers (left). PTH levels of TDF users were significantly higher in subjects with suboptimal 25(OH)D levels than in subjects with optimal levels (right).
Linear regression was performed to identify factors independently associated with PTH values. Univariate analysis identified only one factor, use of TDF, which was directly related to the level of PTH (p ≤ 0.05). Levels of 25(OH)D, use of darunavir, and use of etravirine were inversely related to the PTH (p ≤ 0.05). These four variables were included in multivariable analysis and only TDF and 25(OH)D level were significant in the final analysis, which showed that PTH was directly related to TDF use [p = 0.017, beta = 22.3, 95% CI (4.6, 39.9)] and that it was inversely related to 25(OH)D levels [p = 0.017, beta = −1.0, 95% CI (−1.9, −0.2)]; however, PTH was not significantly associated with GFR (p = 0.9).
Discussion
In this population of ART-treated men, two variables were independently associated with the PTH value: use of TDF and the level of 25(OH)D. As in our study, TDF has been previously associated with abnormalities of bone and calcium metabolism. 3,11 Thirty-two of the 33 subjects on TDF were also receiving FTC. The effect of TDF in the absence of FTC may differ from what we observed; however, the only patient taking TDF without FTC had a PTH value of 120 pg/ml and satisfied the criteria for a clinical diagnosis of secondary hyperparathyroidism. Because low vitamin D status was associated with lack of vitamin D supplement use, our results suggest that vitamin D supplements may reduce the risk of PTH abnormalities in patients on ART. Reducing PTH elevations may confer a range of clinical benefits, as a number of adverse health outcomes are associated with relative elevations of PTH even within the normal range. 12,13
The mechanism underlying the association between TDF use and PTH elevation was not investigated in our study, nor has it been determined by others. We hypothesize that the mechanism may be similar to the one responsible for PTH elevations in patients taking other medications that affect bone density. Impaired calcium absorption appears to be the main pathway leading to PTH elevations in patients taking antiseizure medications, 14 and has been implicated in the osteoporosis/osteopenia observed in patients taking ribavirin. 15 Phenytoin increases 1,25(OH)2D degradation in the intestine 16 and may impair calcium absorption by creating a local 1,25(OH)2D deficit. A similar process could be taking place in our patients. Although PTH levels were not related to circulating 1,25(OH)2D levels, it is possible that they were related to levels of 1,25(OH)2D in the intestine, which were not measured.
The limitations of our study include the lack of longitudinal data, the lack of more extensive data about electrolytes and calcium intake, the fact that PTH levels were not measured after an overnight fast, and the relatively small number of non-TDF users, which limited our ability to identify other cART agents that may impact PTH. We studied a population of largely white men living at moderately high latitude; our results may not apply to other groups.
This study shows that TDF use is associated with PTH greater than or equal to the ULN. Our data strongly suggest that vitamin D status modulates the severity of this association. Future prospective studies should investigate whether vitamin D and calcium supplements may benefit patients with chronic viral infections and PTH elevations.
Footnotes
Acknowledgments
The investigators thank the subjects for participating and Drs. R. Tamler and T. Davies (MSSM) for advice. This study was supported in part by NIH Grants DA016156 and DK066939. Portions of this work were presented in October 2008 at the ISDA meeting in Washington DC.
Author Disclosure Statement
No competing financial interests exist.