
Abstract
Human T cell lymphotropic virus type 1 and 2 (HTLV-1/2) Western blot indeterminate results are a problem for blood banks in endemic areas. To determine the prevalence of HTLV-1/2 infection among indeterminate donors, we analyzed 130 cases from Mashhad, an HTLV-1/2 endemic area in Northeast Iran. The most frequent Western blot bands were GD21 alone (37.2%) followed by rgp46-2 alone (32.1%). We further tested 40 available DNA samples of these cases by PCR for viral sequences, tax, gag, and pol, and found five cases (12.5%) to be positive for two or three HTLV-1 genes. There were no significant age, sex, and blood group differences between PCR-positive and PCR-negative cases. Among PCR-positive individuals, the most prevalent Western blot bands were variable combinations of rgp46-1, GD21, and gp21. The mean of the optical density (OD) of the enzyme-linked immunosorbent assay (ELISA) test was significantly higher in PCR-positive individuals. The frequency of the rgp46-1 band was also significantly higher in PCR-positive cases compared to PCR-negative ones. In conclusion, the majority of HTLV-indeterminate donors lack the HTLV provirus and therefore are not considered infected. However, in some cases with higher ODs in the ELISA test and seroreactivity to env proteins, rgp46-1 and GD21 in particular may be indicative of infection and need further evaluation by molecular methods.
Introduction
H
HTLV-2 shares a number of biological characteristics with HTLV-1, such as similar routes of transmission, and it has also been shown to be associated with a weaker form of HAM/TSP-like neurological disorder, but its association with any malignancy has not yet been confirmed. 1,3
These viruses have a worldwide distribution. HTLV-1 is endemic in the Caribbean, Melanesia, South Western Japan, Central and Western Africa, and South and Central America. HTLV-2 has a more restricted distribution than HTLV-1, primarily occurring in Amerindians in North, Central, and South America, and in injecting drug users worldwide. 1 –6
Northeast Iran, particularly the city of Mashhad, is an endemic region of HTLV infection and it has been reported that 3% of the general population and 0.77% of the blood donors were infected with HTLV-1. 7,8 However, a more recent study has demonstrated that the prevalence of infection in blood donors has declined to 0.42%. 9
Mandatory screening of blood supplies for HTLV-1/2 was implemented in the mid-1980s in countries such as Japan, Canada, and the United States and is being gradually established in many other countries. 3 –10
In the endemic region of Iran screening of blood donors for HTLV-1/2 has continued to be performed since 1996 in blood transfusion services. The screening process is initiated with an HTLV-1/2 specific enzyme-linked immunosorbent assay (ELISA). Samples that are found to be repeatedly reactive by ELISA are confirmed by Western blot assay. In a significant number of cases, which can be verified throughout the world, HTLV-1/2 ELISA is positive but an incomplete antibody response appears on the Western blot. Individuals providing these samples are categorized as HTLV-1/2 seroindeterminates. All blood banks worldwide report these seroindeterminate blood donors with different prevalence. However, to date the clinical significance of these cases has not been identified. 1,2,5,8
This study was conducted to investigate the overall prevalence rate and demographic characteristics of HTLV seroindeterminate blood donors and to determine their infectious status.
Materials and Methods
Samples
From June 2008 to June 2009, a total number of 79,687 volunteer blood donors (93.8% male and 6.2% female) were recruited. All these donors fulfilled the criteria for blood donation; a clinical examination was performed and an interview was conducted to record the history of previous infectious diseases, surgery, blood transfusion, heart disease, anemia, and information on foreign travel. According to our criteria the age range of donors must be between 17 and 65 years. About one-third of these donors were regular donors and the rest were recruited by donor recruitment programs such as media and religious ceremonies.
HTLV 1/2 serologic assay
Serum samples were tested for HTLV-1/2 antibodies using an ELISA assay (MP HTLV 1/2 ELISA 3.0, MP Diagnostics, Singapore) according to the manufacturer's instructions. Reactive samples were retested in duplicate with the same kit. Repeatedly reactive samples were further evaluated with a confirmatory Western blot assay (MP HTLV 2.4 Western blots, MP Diagnostics, Singapore) following the manufacturer's criteria. Seroreactivity was interpreted according to the stringent criteria indicated by the manufacturer. A Western blot test was scored as HTLV-1 positive only if bands for the gag proteins (p19 with or without p24) and two env proteins (GD21 and rpg46-1) were present; it was scored as HTLV-2 positive if bands for the gag proteins (p19 with or without p24) and two env proteins (GD21 and rpg46-2) were found. The presence of p24, p19, and GD21 was considered as HTLV positive but nontyped. The test was identified as indeterminate if specific bands for HTLV that did not meet the criteria of positivity were present. Those that did not exhibit bands specific for HTLV were considered negative (Fig. 1).
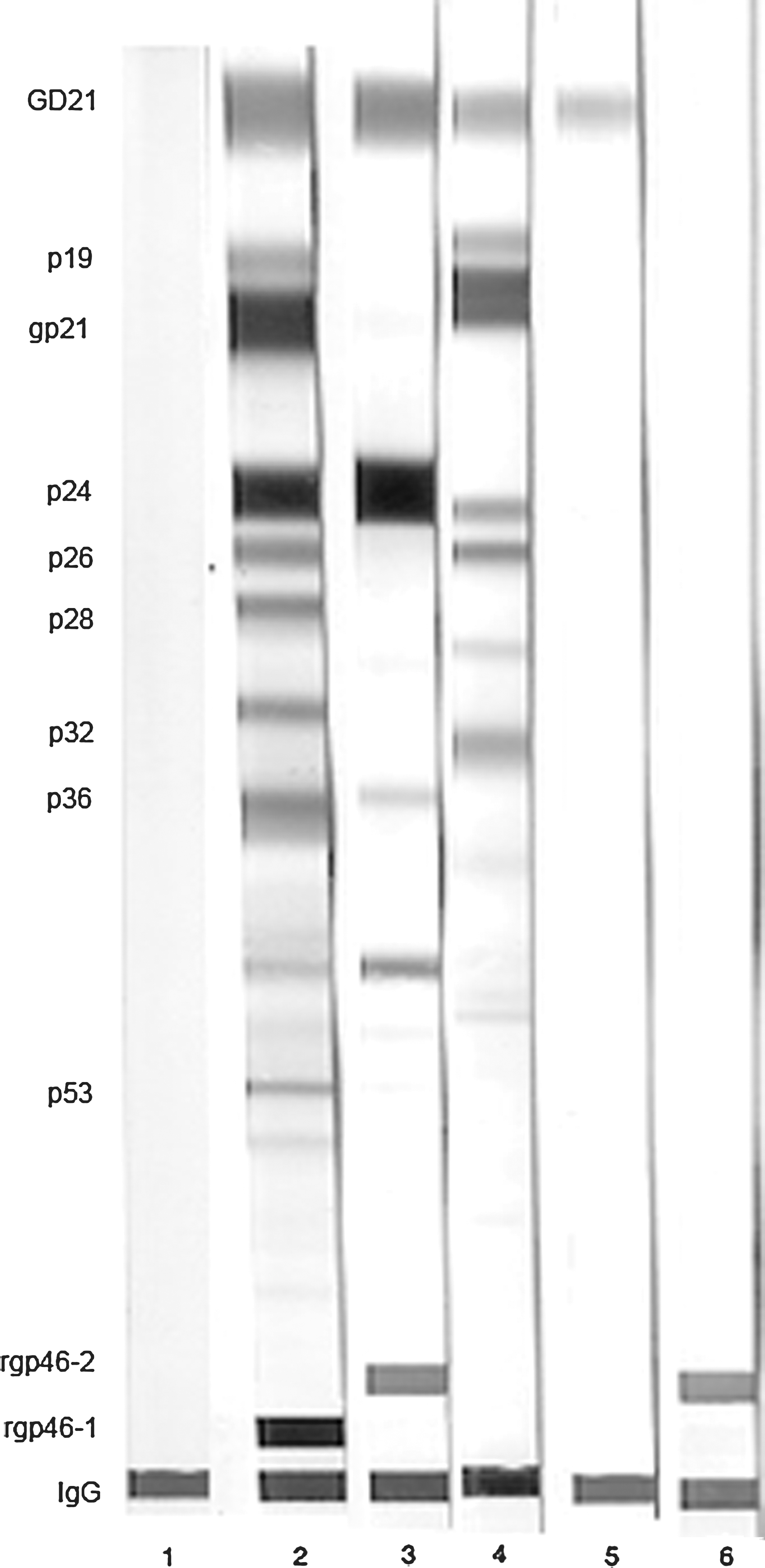
Western blot analysis using MP HTLV 2.4. Lane 1: HTLV-negative control. Lane 2: HTLV-1-positive control. Lane 3: HTLV-2-positive control. Lane 4: HTLV-positive (not typed). Lanes 5 and 6: HTLV indeterminate with isolated GD21 and rgp46-2 bands, respectively.
Molecular analysis
Genomic DNA was extracted from peripheral blood mononuclear cells of Western blot seroindeterminate individuals using a commercial kit (QIAamp DNA blood minikit; Qiagen GmbH, Hilden, Germany) according to the manufacturer's instructions. Primer sequences and polymerase chain reaction (PCR) were previously described. 11 Briefly, each reaction contained 1.5 μg of DNA, 0.2 mM dNTP mix, 2 μl of 10 × reaction buffer, 0.1 mM each oligonucleotide primer, and 1 U of Taq DNA polymerase in a total volume of 20 μl. For the gag region we used a seminested PCR with primers gag949, and gag1244 in the first reaction and gag949 and gag1056 in the second reaction, which generated 332-bp and 127-bp fragments, respectively. We used Pol3-4 and SK111 for the pol region and Rmtax1 and Rmtax2 for the tax region, which produced 450-bp and 250-bp fragments, respectively. Gag and tax primers were specific for HTLV-1 whereas pol primers were common for both types.
The reaction mixture was processed as follows: after denaturating at 94°C for 5 min, the reaction mixtures were cycled 40 times at 94°C for 1 min, 55°C (tax), or 58°C (gag, pol) for 1 min, and 72°C for 2 min followed by a 10-min final extension. For the seminested PCR, the first fragment was amplified and 2 μl of the initial PCR mixture was used for the second run. Amplified DNA was size fractionated on 1.5% agarose gel electrophoresis and visualized by ethidium bromide. The amplifiability of each extracted DNA sample was confirmed with a PCR for the β-globin gene.
Statistical analysis
The prevalence of HTLV was calculated with an estimation of 95% confidence interval (95% CI). The comparison of sex and age was determined using the chi-square test. The Fisher's exact test and Mann–Whitney test were used for comparing the blood groups and ODs in the ELISA assay, respectively. A p-value less than 0.05 was considered significant.
Results
Of 79,687 donors screened for HTLV-1/2, 512 (6.4%) were reported repeatedly reactive by the ELISA assay. Western blot analysis revealed 285 (0.36%) positive for HTLV-1 and 16 (0.02%) positive for HTLV. One hundred and thirty (0.16%) were found to be indeterminate including 114 (87.7%) males and 16 (12.3%) females, with a mean age of 37.6. The Western blot patterns of seroindeterminate subjects are summarized in Table 1. The most common HTLV-indeterminate patterns were GD21 alone (37.2%) followed by rgp46-2 alone (32.1%). No HTLV-1 Gag indeterminate profile (HGIP) was found. Only 40 seroindeterminate donors accepted a second sampling for molecular testing. The interval between the first and second sampling for these donors was variable (mean = 4 months). The second sample was tested with the same ELISA and Western blot and confirmed to be indeterminate. Proviral DNA was found in 5 out of these 40 indeterminate samples (12.5%), of which 4 samples were positive for tax, pol, and gag and the other was positive only for the tax and pol regions.
There were no significant age, sex, and blood group differences between HTLV-negative and HTLV-indeterminate donors except that the percentage of female donors was higher in the indeterminate group in comparison to HTLV-negative donors (Chi-square test, p = 0.003). Also there were no significant age, sex, and blood group differences between PCR positive and PCR negative indeterminate individuals (Chi-square test, p = 0.09 and p = 0.055; Fisher's exact test, p = 0.29, respectively). The mean of the optical density (OD) of the ELISA assay among PCR-positive samples was significantly higher than those with negative PCR results (Mann–Whitney test, p = 0.004).
Among PCR-positive specimens, the most prevalent Western blot bands were variable combinations of the rgp46-1, GD21, and gp21 bands. The frequency of the rgp46-1 band was significantly higher and the frequency of the rgp46-2 band was significantly lower in PCR-positive cases compared to PCR-negative ones (Fisher's exact test, p = 0.007 and 0.0025, respectively).
Discussion
HTLV-1/2 Western blot indeterminate results are a worldwide problem of blood banks, especially in endemic areas, although the clinical and epidemiological importance of these results is still not fully understood. We analyzed 79,687 blood donors with ELISA and Western blot and found the HTLV-1/2-positive and indeterminate prevalence rate to be 0.37% and 0.16%, respectively. To investigate the infectious status of indeterminate donors, we further examined 40 indeterminate subjects by PCR. Five samples (12.5%) were determined to be positive for HTLV-1. This finding is consistent with some previous studies, especially in endemic areas, for HTLV-1/2.
For instance, Costa and Segurado 3 found that 0.98% of donors in Brazil were Western blot indeterminate and 9.2% of these indeterminate cases tested PCR positive. Mangano et al. 1 studied 89 indeterminate samples from Argentinian blood donors and reported an overall indeterminate prevalence rate of 0.10%, of which 13.8% of them were HTLV-1/2 PCR positive. Berini et al. 4 studied 83 HTLV-1/2 indeterminate Western blot cases in Argentina and found 13.2% of them were positive by PCR. Santos et al. 12 tested 41 Western blot seroindeterminate individuals and found 22% of them were positive by PCR. On the other hand, researchers, particularly in nonendemic regions, have revealed different results; for example, Lal et al. 13 studied U.S. blood donors and determined that 0.14% were Western blot indeterminate and all were PCR negative. Similarly, Rouet et al. 2 found 0.4% Western blot indeterminate in Caribbean blood donors who all were PCR negative. These findings highlight the importance of indeterminate results in HTLV endemic regions.
There were no significant differences in age, gender, and blood groups among the seroindeterminate and seronegative cases in our study except for a gender difference between the two groups. These findings are consistent to some extent with other findings. For example, studies by Santos et al. 12 and Jacob et al. 14 showed younger men predominated among seroindeterminate individuals whereas older women predominated between seropositive individuals for HTLV-1/2. The survey by Cesaire et al. 15 did not find any significant gender difference between these groups, but they found the seroindeterminate cases were younger than the seropositive ones. However, the study by Mauclere et al. 16 determined that the prevalence of the indeterminate Western blot profile was similar between males and females and did not correlate with age. It seems that even in endemic areas the demographic characteristics of the HTLV-indeterminate population is not similar.
The most common HTLV-indeterminate pattern by Western blot in our study was GD21 alone followed by rgp46-2 alone, which is similar to the findings of Lu et al. 17 and Mangano et al., 1 but is in contrast to the findings of Rouet et al. 2 in the Caribbean, the study of Costa et al. 3 in Brazil, the survey of Lal et al. 13 in the United States, the study of Cesaire et al. 16 in Martinique, and the findings of Berini et al. 4 in Argentina, which all demonstrated high gag indeterminate as the most prevalent HTLV-indeterminate Western blot profile.
Blood banks, especially in endemic regions, have reported anti-HTLV indeterminate results among blood donors. The significance of indeterminate results and counselling for these cases are a challenge for physicians in HTLV-endemic areas as well as for blood banks throughout the world. Presumptive etiologies of indeterminate profiles are different. Some studies demonstrated that it may be due to cross-reactivity to other agents including antibodies against peptides of Plasmodium falciparum, 11,18 endogenous retroviral sequences, 13 simian T-lymphotropic virus type 1 (STLV-1), 19 and varicella-zoster virus. 20 Others revealed different causes such as seroconversion 16 and infection by variant HTLV strains containing mutations in proviral DNA sequences that encode immunodominant epitopes. 21 –24
In conclusion, in HTLV-endemic regions such as Northeast Iran, molecular evidence of HTLV infection may be revealed in a number of indeterminate blood donors. Therefore, to definitely determine the infectious status of HTLV-1/2 indeterminate donors, molecular analysis associated with follow-up studies, especially in those with a high OD in the ELISA test and/or seroreactivity to env proteins in the Western blot assay, is strongly recommended.
Footnotes
Acknowledgment
We thank the technical staff of Mashhad blood transfusion service for their kind assistance in sample collection and testing.
Author Disclosure Statement
No competing financial interests exist.