
Abstract
HIV subtype-specific data on mutation type, rate, and accumulation following HAART treatment failure are limited. We studied patterns and accrual of drug resistance mutations in a Cambodian CRF01_AE-infected cohort continuing a virologically failing first-line, nonnucleoside reverse transcriptase inhibitor- (NNRTI-) based, HAART. Between 2005 and 2007, 837 adult HIV-infected patients had regular plasma HIV-1 RNA viral load measurements at Sihanouk Hospital Centre of Hope (SHCH), Cambodia. Drug resistance testing was performed in all patients with HIV-1 RNA >1000 copies/ml after at least 6 months of HAART. Seventy-one patients with a mean age of 34 years, of whom 68% were male, were retrospectively assessed at virological failure. The median duration of antiretroviral therapy was 12.3 (IQR 7.1-18.23) months, the median CD4 cell count was 173 (IQR 118–256) cells/mm3, and the mean plasma HIV-1 RNA viral load was 3.9 log (SD 0.72) at failure. NNRTI mutations, M184I/V mutation, thymidine analogue mutations, and K65R were observed in 78.9%, 69%, 20%, and 12.7% of patients, respectively. For 33 patients, genotypic testing was carried out on at least two occasions before the switch to second-line HAART after a median duration of 5.8 (IQR 4.3–6.1) months of virological failure: 54.5% of patients accumulated new mutations with a rate of 1.6 mutations per person-year. Accumulation was seen both for nucleoside and nonnucleoside reverse transcriptase inhibitors, and also in patients with low-level viremia. Subtype-specific data on mutation type, rate, and accumulation after HAART failure are urgently needed to optimize treatment strategies in resource-limited settings.
Introduction
T
As in other low-income countries (LINC) plasma HIV-1 RNA viral load measurements are not routinely performed in Cambodia and the monitoring of patients' response to HAART generally relies on immunological and clinical criteria. In the absence of virological monitoring, treatment failure is often detected late and the delay in switching HIV therapy puts patients at risk of clinical deterioration and accumulating drug resistance, which might jeopardize future treatment options due to cross-resistance to drugs of the same class.
Data on resistance patterns have largely been generated from studies and reports involving patients infected by the HIV-1 subtype B virus, while the prevalence and pathway of resistance mutations in non-B subtypes are poorly studied in most LINC due to a lack of laboratory facilities, as well as the high cost and complexity of research techniques.
Data on mutation type, rate, and accumulation following treatment failure are urgently needed to optimize treatment strategies in LINC. Mutations induced by nucleoside reverse transcriptase inhibitors (NRTIs) and nonnucleoside reverse transcriptase inhibitors (NNRTIs) seem to differ between subtypes. 3 –8 Therefore, information concerning resistance patterns during treatment failure in regions in which certain subtypes predominate could influence the choice of second-line regimens and shed light on the need for regionally adapted strategies.
Although recent studies have begun to address these needs for patients infected with subtype C, data on other common subtypes, such as CRF01_AE, are very limited. 9 –12
The present study aims to describe the pattern of resistance mutations seen during HAART failure in a Cambodian CRF01_AE-infected cohort and to assess the accrual of mutations while patients continued to receive virologically failing first-line NNRTI-based regimen.
Materials and Methods
Between 2005 and 2007, 837 adult HIV-infected patients at Sihanouk Hospital Centre of Hope (SHCH), Phnom Penh, Cambodia, had regular plasma HIV-1 RNA viral load measurements. These were performed as part of a prospective study developing an algorithm to identify patients failing first-line HAART, “An algorithm to optimize viral load testing in HIV-positive patients with suspected first-line antiretroviral therapy failure in Cambodia.” 13
We conducted a retrospective cohort analysis using these plasma HIV-1 RNA viral load data and performed drug resistance testing on the stored samples of patients identified with treatment failure. Only during the above mentioned period, while the “algorithm study” took place, viral load samples were systematically collected in SHCH and available furthermore for retrospective genotypic testing.
Laboratory tests
Genotypic antiretroviral resistance testing was conducted on viral isolates from patients with a plasma HIV-1 RNA viral load above 1000 copies/ml after at least 6 months of antiretroviral therapy and before switching to second-line treatment.
HIV-1 RNA levels were measured using standard quantitative reverse transcriptase polymerase chain reaction (quantification limit 50 HIV-1 RNA copies/ml; Roche, Cobas AmpliPrep Amplicor HIV-1 viral load test). For viral loads above 1000 copies/ml HIV-1 reverse transcriptase, genotyping was performed using Trugene HIV-1 genotyping (Trugene, Siemens and IDNS, Smartgene). The resistance profile to antiretroviral drugs was interpreted according to the latest Stanford guidelines for HIV genotyping testing (
Mutations
Resistance mutations were classified according to International AIDS Society (IAS)–USA guidelines. 14 As major NRTI mutations, we considered M41L, D67N, K70R, M184V, L210W, T215Y/F, and K219E/Q. Other important NRTI mutations considered were K65R, L74V, Q151M Complex, and 69 Insertion Complex. Major NNRTI mutations included amino acid substitutions in the reverse transcriptase gene positions: 100, 103, 106, 108, 181, 188, 190, 225, 230, and 236. Mutations conferring reduced susceptibility to the different antiretrovirals (ARVs) were described at virological failure and at follow-up.
Procedures
Between 2005 and 2007, samples for HIV-1 RNA viral load testing were prospectively collected every 6 months from all patients included in the study “An algorithm to optimize viral load testing in HIV-positive patients with suspected first-line antiretroviral therapy failure in Cambodia.” 13 Samples were shipped to the Institute of Tropical Medicine (ITM) in Antwerp and were stored at −80°C after viral load testing.
Single samples at failure were available for the majority of patients. We selected all samples with an HIV-1 RNA viral load >1000 copies/ml for resistance testing.
For 33 patients, two samples were available before subsequent second-line therapy was started, due to delays between sampling, shipping, testing, communicating the viral load results, and the decision taken by the local physicians before to switch. Among these patients, the paired samples with HIV-1 RNA viral load >1000 copies/ml were included in both the “prevalence group” and the “accumulation group.” A single postfailure sample was available for the remainder of patients; these patients were included only in the “prevalence group.”
Statistical analyses
Means (±SD), medians, interquartile range (IQR), and frequencies were used to describe patients' characteristics. Study patients were categorized into two groups based on available genotypic tests: a “prevalence group,” in which genotyping was done on patients who had an HIV-1 RNA viral load of >1000 copies/ml after at least 6 months of HIV treatment before switching to second-line, and an “accumulation group,” in which patients had two genotypic resistance tests to assess the accrual of mutations, while they were on a failing first-line NNRTI-based treatment for a short time (approximately 6 months).
Fisher's exact test was used to examine the association between regimen used and mutation selection. p values <0.05 were considered statistically significant. All statistical analyses were performed using Stata software, version 10.1 (Stata Corporation, College Station, TX).
Ethical considerations
The study protocol was approved by the Institutional Review Board of the Institute of Tropical Medicine in Antwerp and the National Ethics Committee in Cambodia. All HIV patients gave written informed consent and benefitted from the findings through the interpretation of resistance tests, with targeted switching to second-line HAART when needed.
GenBank submission
HIV sequences obtained in this study were submitted to GenBank, with accession numbers HM565489–HM565738.
Results
Seventy-one (8%) of the 837 patients had at least one sample with an HIV-1 RNA viral load level above 1000 copies/ml (“prevalence group”), including 33 patients (46% of 71) with two consecutive levels above 1000 copies/ml (“accumulation group”). The overall response to HAART of the SHCH HIV-infected cohort has been described elsewhere. 15
Prevalence group
Two-thirds of the 71 study participants were men. They began treatment with a median CD4 count of 34 cells/mm3 (IQR 8–137) at a mean age of 34 years (IQR 30–38). Of the 71 patients, 68 (96%) were infected with HIV-1 subtype CRF01_AE and all received two NRTI + NNRTI combination therapy, most commonly stavudine (d4T) plus lamivudine (3TC) plus nevirapine (NVP) (n = 56, 79%) (Table 1). At HAART initiation, 10 patients reported previous antiretroviral treatment exposure for a median of 20 weeks (IQR 4–28); four had received dual NRTI therapy and six had taken d4T/3TC/NVP.
Four patients with dual NRTI therapy and six with d4T/3TC/NVP.
The median duration of therapy at failure was 12.3 (IQR 7.1–18.2) months, the median CD4 count was 173 (IQR 118–256) cells/mm3, and the mean plasma HIV-1 RNA was 3.9 log (SD 0.7). The majority of patients (69%) failed with M184I/V plus any of the nonnucleoside-induced mutations, which were detected in 78.9% of the patients at the following frequencies: 181C/I: 50.7%; K103N: 22.5%; G190A: 16.9%; V108I: 15.5%; and Y188L: 5.6%.
Two or more nonnucleoside mutations could be detected in 46.5% of patients: commonly Y181C plus V108I (in 10% of 71) or Y181C plus K103N (in 8% of 71 patients). The use of d4T/NVP was associated with Y181C mutation selection (p = 0.037) whereas the use of AZT/EFV was associated with the selection of K103N (p = 0.072).
Thymidine analogue mutations (TAMs) were detected in 20% (n = 14) of patients: the TAM2 pathway (D67N, K70R, T215F, and K219Q/E) was present in 9/14 (64.2%) patients, the TAM1 (M41L, L210W, and T215Y) was present in 3/14 (21.4%), two patients harbored an M41L plus another TAM2 mutation, and T215F was more frequent than T215Y (7.0 versus 2.8%).
Of interest, V75T/M and T69D/N (associated with decreased susceptibility to d4T and ddI) were not uncommon, each being detected in 9.9% of patients. The Q151M multidrug resistance mutation was observed in 4.2% (n = 3) (Fig. 1).
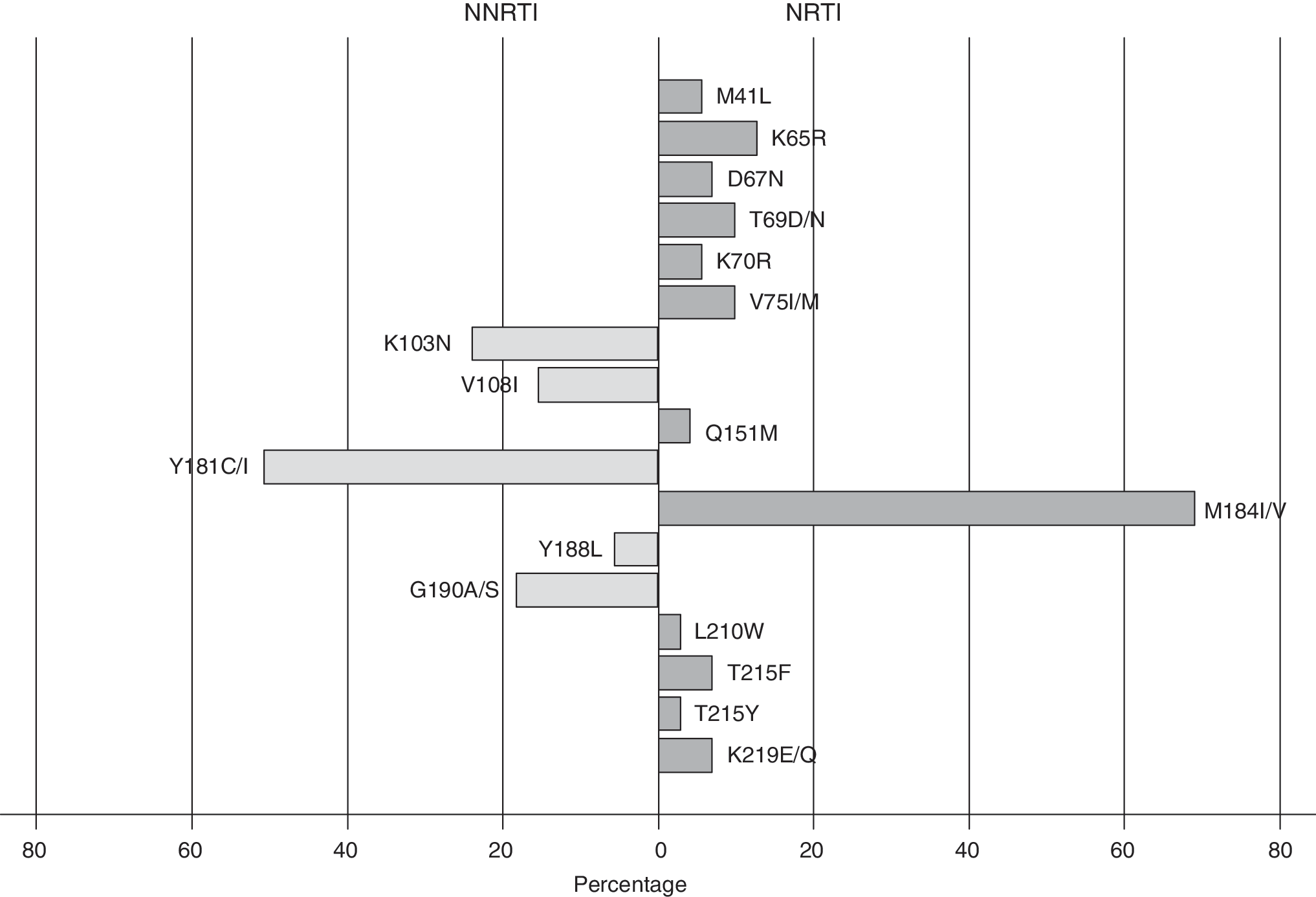
Prevalence of mutations at virological failure in 71 patients.
The K65R mutation appeared in isolates from nine patients (12.7%), of whom only two were taking tenofovir, while the other seven were on treatment with d4T/3TC/NVP and did not report any previous use of antiretrovirals. At the time of K65R detection, the median duration of ART was 12.2 months (IQR 8.6–12.4) and the median plasma viral load 3.6 log HIV RNA copies/ml (range: 3.03–5.17). Of the patients harboring a K65R mutation 77% had a viral load of <4 log copies/ml at failure. The K65R mutation was rarely detected with TAMs: one patient presented with an M41L mutation and another patient, previously treated with dual NRTI therapy, presented with a combination of K70R and K219E mutations together with a Q151M multidrug resistance complex.
Mutations contributing to resistance to the recently FDA-approved NNRTI etravirine (ETR) emerged in 43 patients (60.5%). Eleven patients had two or more ETR resistance-associated mutations, with the most prevalent combination being Y181C + G190A (7/11).
No mutations could be detected in 20% (n = 14) of these 71 patients and one sample failed to amplify. Out of 14 patients who lacked genotypic mutations despite detectable HIV RNA viral load, six patients showed undetectable HIV RNA viral load at the following controls, two were lost to follow up, four were immediately switched to second-line therapy, and the last two did not have any other HIV RNA viral load measurement.
Accumulation group
Data on the potential accumulation of mutations after virological failure could be analyzed for 33 patients for whom plasma samples with HIV RNA viral load >1000 copies/ml were available on at least two occasions before switching to second-line therapy. The median time interval between the two tests was 5.8 months.
Resistance mutations continued to accumulate in 18 patients (54.5%). Additional mutations accumulated for both NRTI and NNRTI: 12 TAMs, five other NRTI mutations (A62V, V75M, F77L, and M184V twice), and nine NNRTI-related mutations were accrued respectively in nine, four, and seven patients (Table 2).
d4T, stavudine; 3TC, lamivudine; NVP, nevirapine; EFV, efavirenz.
Addition mutations in the second sample are in bold.
Previous HAART exposure: dAZT/3TC for 7 months; ed4T/3TC/NVP for 5 months; fddl monotherapy for 3 months followed by d4T/3TC/NVP for an additional 3 months.
In an attempt to quantify the incidence of new resistance-associated mutations, we calculated the number of new mutations divided by person-time at risk. This resulted in a rate of new resistance-associated mutations of 1.6 per person-year. The number of NNRTI mutations increased from 34 to 43, the number of TAMs increased from 6 to 18, and the number of other nucleoside mutations increased from 24 to 29 (Fig. 2). Accumulation of resistance mutations was also observed in patients with persistent HIV-1 RNA levels <5000 copies/ml.
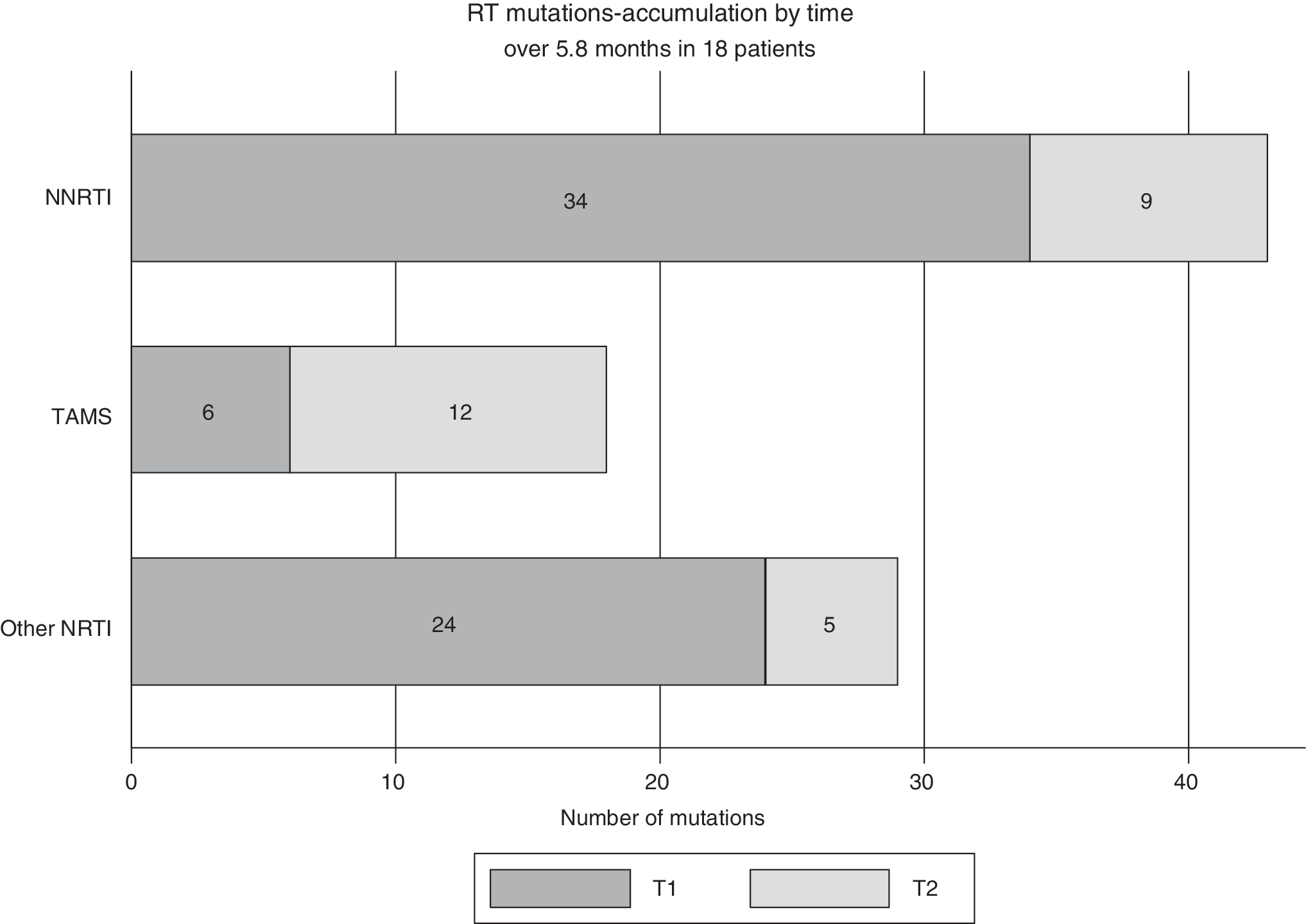
Accumulation of HIV drug resistance mutations.
Discussion
We conducted a retrospective cohort analysis of subtype CRF01_AE-infected patients to determine drug resistance patterns at virological failure and accumulation of mutations while continuing for a short period a failing first-line HAART. Although mutations were similar to those seen in subtype-B-infected patients, the rates and frequencies differed and accumulations of both NRTI and NNRTI mutations were observed even at relatively low HIV-1 RNA viral load.
Most countries with limited resources have adopted the so-called “public health approach” of the World Health Organization (WHO) to deliver comprehensive HIV/AIDS care. In this approach, HIV treatment options are simplified and standardized, and consist of a first-line regimen with an NNRTI plus two NRTIs—generally 3TC and one thymidine analogue such as zidovudine (AZT) or d4T—while the second-line regimen ideally includes a boosted protease inhibitor (PI). 16
Although the WHO clearly states the importance for developing countries to start moving away from d4T-containing regimens given the toxicities associated with this drug, the combination of d4T/3TC/NVP is one of the most common first-line therapies used in LINC, due to its availability as a generic fixed-dose combination with low pill burden and low cost. 17 Failure of the most common first-line HAART regimens used in developing countries (such as d4T/AZT + 3TC + NNRTI) is associated primarily with NNRTI mutations, the 3TC-induced M184V mutation, and, at lower frequency and after longer duration of treatment failure, with TAMs. 18 –26 Moreover, the multidrug resistance reverse transcriptase mutation K65R, generally linked to tenofovir-containing failing regimens, has increasingly been reported in non-B subtype- infected patients failing d4T- or ddI-based regimens. 27 –29 The likely accumulation of TAMs, the K65R selection, or the emergence of the Q151M complex after treatment failure may have an impact on the efficacy of all other available NRTIs, which are generally used together with a boosted PI in the second-line regimen, due to extensive NRTIs cross-resistance.
In our CRF01_AE subtype-infected cohort almost half of the patients (46.5%) harbored two or more NNRTI mutations at failure, with Y181C as the most commonly detected NNRTI mutation after d4T/NVP use (p = 0.037). The most prevalent NRTI-associated mutation was M184I/V, conferring resistance to lamivudine and emtricitabine (FTC), while the prospective nature of the initial cohort allowing early detection of virological failure may explain the low frequency of TAMs, which are expected to emerge when virological replication is ongoing for a longer period.
The K65R mutation, preferentially selected after failing d4T-containing first-line therapy in subtype C patients, was not that rare among our failing patients. This has been reported by others, and has great relevance to the choice of backbones for the second-line treatment options. 30,31 All samples harboring a K65R presented with an Y181C. In one patient those were the only two mutations detected at failure at month 12 of treatment, possibly due to the strong interactions between Y181C and some NRTI mutations such as K65R 32 ; out of nine, only five samples presenting the K65R harbored the 3TC-related mutation M184V. The K65R was associated in only one patient with a Q151M complex. Other pan-nucleoside resistance mutations, such as the 69-insertion or K70E (latest associated with TDF resistance), were not detected in our population.
Looking at the “accumulation group,” the low but detectable RNA level gave an indication of ongoing selective drug pressure and low-level viremia did not preclude accrual of mutations (Table 2). Other cohort studies observing patients kept under failing HAART regimens, mostly unboosted PI-based, have largely shown that the rate of accumulation of drug resistance mutations is independent of HIV viral load and that resistance mutations accumulate even at low concentrations of plasma HIV RNA viral load, with an incidence of new resistance-associated mutations varying from 0.93 to 1.96 over 6 months and 1.61 mutations per year. 33 –36
There is limited agreement on the HIV-1 RNA viral load threshold at which we should switch patients to second-line therapy in LINC. The most recent WHO guidelines recommend that a persistent viral load above 5000 copies/ml (in a patient on a regimen for more than 6 months, and in whom drug adherence is determined to be sufficient) should be used as a therapeutic switching threshold. 16 Although we know that the continuing use of a failing HAART regimen will lead to additional mutations, there are no outcome data from LINC that highlight the impact of the late switch to second-line, taking into account that only limited therapeutic options are available. 37,38 In our accumulation group the resistance mutations continued to accrue at a rate of 1.6 mutations per person-year. Interestingly, the patients with TAM1 accrual were those exposed to AZT, had a longer duration of HAART (>18 months), and had an HIV RNA load of >4 log copies/ml at failure.
Looking at phenotypic susceptibility data in those accumulating resistance mutations (Fig. 3), the second sequence showed a decreased susceptibility to the most common backbones used in second-line therapy in LINC. The fact that TDF seemed to retain reasonable antiretroviral activity after failure supports the more recent WHO recommendations on simplification of the second-line NRTI options, which suggest the use of TDF + 3TC or FTC for patients failing first-line AZT- or d4T-containing treatment. However, 15.5% of our patients harboring by genotype pan-nucleoside resistance mutations (Q151M complex, K65R) needed a stronger NRTI backbone combination, such as AZT/3TC/TDF together with one of the preferred boosted PIs for second-line HAART. Of note, the use of new generation NNRTIs, such as etravirine, would have been compromised in our population and in general it would not be so promising in LINC, where routine HIV RNA viral load monitoring is not feasible and multiple NNRTI mutations would be expected in the scenario of late switch. 39,40

Evolution of NRTI resistance interpretation in 33 patients (accumulation group).
There are a number of important limitations to our study. Retrospective analysis of a prospective cohort was performed to maximize the utility of the collected data. We believe this was appropriate in this setting, although we would have preferred a nationwide sample. The limited numbers of patients, particularly in the accumulation group, certainly warrant confirmation in larger populations.
More sensitive resistance assays may be able to detect mutations with potential clinical relevance, even if they are present in small minority populations.
Another key limitation of this study is that blood samples prior to HAART initiation were unavailable, and therefore possible baseline-resistance mutations could not be detected. However, the low prevalence of HIV-1 drug resistance transmitted virus in Cambodia makes transmitted primary resistance a rare event among our HIV treatment-naive patients. 41
This study utilized an unusual opportunity to evaluate the rate of emergence of genotypic resistance to the common first-line HAART used in Cambodia in patients maintained for a short period on the same treatment after the onset of virological failure.
The appearance of mutations in response to NRTIs and NNRTIs seems to differ between subtypes CRF01_AE and B. Accumulation of mutations may occur relatively quickly and at a low HIV RNA level. These accumulations have relevance not only to the choice of first- and second-line treatment regimens, but also to the type and frequency of patient monitoring employed during therapy. Determination of subtype-specific resistance characteristics should inform HIV treatment policy.
Footnotes
Acknowledgments
This research was funded by the European Commission project Europe AID, CONTRACT SANTE/2002/045-809: Clinical research/activity II B 5, and by the Belgian DGDC (Directory General of Development Cooperation) through a framework agreement with ITM (Institutional Strengthening project HOPE Cambodia 95900 and 95901). We would like to thank the patients and the doctors of the Sihanouk Hospital Center of HOPE who participated in the study and Sok Sopheak for designing the database. We thank Sergio Garcia and Leo Heyndrickx for the excellent work done on managing and genotyping the samples.
Author Disclosure Statement
No competing financial interests exist.