
Abstract
A diverse array of non-subtype B HIV-1 viruses circulates in Africa and dominates the global pandemic. It is important to understand how drug resistance mutations in non-B subtypes may develop differently from the patterns described in subtype B. HIV-1 reverse transcriptase and protease sequences from 338 patients with treatment failure to first-line ART regimens were evaluated. Multivariate logistic regression was used to examine the effect of subtype on each mutation controlling for regimen, time on therapy, and total mutations. The distribution of HIV-1 subtypes included CRF02_AG (45.0%), G (37.9%), CRF06_cpx (4.4%), A (3.6%), and other subtypes or recombinant sequences (9.2%). The most common NRTI mutations were M184V (89.1%) and thymidine analog mutations (TAMs). The most common NNRTI mutations were Y181C (49.7%), K103N (36.4%), G190A (26.3%), and A98G (19.5%). Multivariate analysis showed that CRF02_AG was less likely to have the M41L mutation compared to other subtypes [adjusted odds ratio (AOR) = 0.35; p = 0.022]. Subtype A patients showed a 42.5-fold increased risk (AOR = 42.5, p = 0.001) for the L210W mutation. Among NNRTI mutations, subtype G patients had an increased risk for A98G (AOR = 2.40, p = 0.036) and V106I (AOR = 6.15, p = 0.010), whereas subtype CRF02_AG patients had an increased risk for V90I (AOR = 3.16; p = 0.003) and a decreased risk for A98G (AOR = 0.48, p = 0.019). Five RT mutations were found to vary significantly between different non-B West African subtypes. Further study to understand the clinical impact of subtype-specific diversity on drug resistance will be critically important to the continued success of ART scale-up in resource-limited settings.
Introduction
T
Nigeria, like much of West Africa, is known to have multiple HIV-1 subtypes as well as HIV-2 infections. The predominant HIV-1 subtypes include CRF02_AG and G, the former first described in Ibadan, Nigeria in 1994. 4 Sankalé and colleagues have reported on a diverse array of subtypes including CRF02_AG, G, CRF06_cpx, A3, and unique recombinant forms that appear to differ geographically within Nigeria. 5 Similar distributions of HIV-1 subtypes have also been described in other West African countries including Senegal, 3 Cameroon, 6 Ivory Coast, 7 and Gambia. 8
Until recently, antiretroviral drugs were developed and tested for efficacy with subtype B viruses as the reference. The clinical effectiveness of these drugs and their patterns of drug resistance were established in clinical trials conducted for the most part on patients infected with subtype B. Although most drugs would be expected to act on targets that were conserved as a result of their critical function in the viral replication cycle such as reverse transcription, protein processing (protease), integration, and coreceptor binding, it seems probable that genetic differences between subtypes might impact the drug resistance pathways or kinetics of drug resistance development. It has been shown that the mutational pathways to drug resistance to nucleoside reverse transcriptase inhibitor (NRTI) drugs may vary among different HIV-1 subtypes. 9 –14 In addition, non-B subtype HIV genomes carry subtype-specific polymorphisms that act as minor mutations in subtype B, particularly in the protease gene. 15 –17 The impact of these genetic differences on the clinical response to antiretroviral therapy has yet to be fully assessed. 18 –24
Nigeria is the most populous country in sub-Saharan Africa with a recent national census indicating a population exceeding 140 million. As in neighboring West African countries, HIV is thought to have entered the country in the mid-1980s. By 2000, based on National HIV Sentinel Surveillance surveys, cases of infection had been reported in all 36 states of the Federation and the epidemic was considered generalized. In 2007, the Nigerian National Sentinel Surveillance estimated the nationwide HIV prevalence at 4.4%, translating into ∼2.8 million HIV-infected individuals. 25 In 2002, the government of Nigeria began its National ART program with the purchase of generic antiretroviral therapy (ART) drugs for 10,000 adults and 5000 pediatric AIDS cases, with treatment delivery at 25 designated federal ART centers. The ART drug regimen was stavudine (d4T) + lamivudine (3TC) + nevirapine (NVP) and was provided to eligible AIDS patients for the nominal fee of 1000 Naira (∼$7 USD) per month. However, the patients were responsible for the cost of laboratory monitoring.
In 2004, the United States President's Emergency Plan for AIDS Relief (PEPFAR) began in 15 focus countries including Nigeria. 26 The Harvard School of Public Health PEPFAR program initiated ART in six university teaching hospitals or medical research institutions in the first year. All of these clinics were designated federal ART sites and had already initiated some AIDS patients on ART through the government of Nigeria ART program. A broader array of FDA-approved ART drugs was available for first- and second-line treatment and laboratory monitoring was provided free of charge to all patients including those on government-provided drugs. ART treatment and care in Nigeria were further expanded with contributions from other international donor organizations and programs such as the Global Fund for AIDS, Malaria and Tuberculosis, the World Bank, and the Clinton Foundation. 27 By 2009, over 300,000 eligible patients in the country were receiving ART; however, this was still considered less than half of the estimated 800,000 patients in need of ART in the country.
In a 7-year period, Nigeria, like many other sub-Saharan African countries, has initiated ART treatment and care to significant numbers of eligible AIDS patients. The early assessment of ART efficacy in these treated patients has been similar to that described in ART treatment trials in the developed world. 28 –30 However, the durability of these responses has yet to be well studied. Critical to the sustainability of these treatment responses and ultimate success of these programs is the surveillance of drug resistance in both untreated and treated populations. In this study we examined HIV-1 genotype data acquired through surveillance of a large population of adult Nigerian patients failing first-line ART in a population in which multiple non-B HIV-1 subtypes are prevalent. We determined the HIV-1 subtype based on reverse transcriptase (RT) and protease (PR) sequences and mapped these by clinic sites distributed throughout the country. We characterized subtype-specific mutations that develop in response to nucleoside and nonnucleoside reverse transcriptase inhibitor drugs (NRTI and NNRTI, respectively) and also described polymorphisms in the PR gene unique to these HIV-1 subtypes.
Materials and Methods
Setting and patients
Since 2004 the Harvard School of Public Health has participated in the PEPFAR program to scale up ART in Nigeria, designated as the AIDS Prevention Initiative in Nigeria (APIN) Plus. According to Nigerian national guidelines, patients were placed on first-line ART consisting of two NRTIs (most commonly stavudine, zidovudine, or tenofovir, plus lamivudine or emtricitabine) and one NNRTI (nevirapine or efavirenz). Patients in virologic failure were switched to second-line NRTI and PR inhibitor-containing regimens. As part of clinical care, genotype testing was performed on a limited number of patients failing first-line therapy prior to drug regimen change at six federal ART centers in four Nigerian cities: Lagos (Lagos State), Ibadan (Oyo State), Jos (Plateau State), and Maiduguri (Borno State).
Patients were recruited for participation and enrolled in the APIN Plus ART treatment program following written informed consent, which was subject to ethical review by the Institutional Review Boards of the University of Ibadan/University College Hospital; National Institute for Medical Research, Lagos; Jos University Teaching Hospital; University of Maiduguri Teaching Hospital; and the Harvard School of Public Health. Criteria for inclusion in this study were plasma HIV RNA >1000 copies/ml after 6 months or more on first-line therapy and the presence of one or more major drug resistance mutations as defined by the International AIDS Society-USA. 31 If more than one genotype had been performed on the same patient, the first result obtained after 6 months on therapy was analyzed.
HIV-1 genotype
As part of routine clinical care, EDTA-separated blood was collected from patients in virologic failure and cryopreserved plasma was shipped in dry liquid nitrogen containers to the Harvard School of Public Health in Boston, where genotypic testing was performed. The ViroSeq HIV-1 Genotyping System 2.0 Assay (Abbott, Chicago, IL) was used to reverse-transcribe and amplify 297 bases of the PR and 1005 bases of the RT genes. The sequence was edited and compared to an HXB2 subtype B reference with the manufacturer's software to generate lists of mutations and polymorphisms. Sequences were aligned in CLUSTAL W (Belfield, Dublin) along with reference sequences from the Los Alamos repository, 32 and neighbor-joining trees were used to classify them by subtype.
Statistical analyses
Univariate analysis of the association between NRTI and NNRTI drug resistance mutations listed in the International AIDS Society USA guidelines 31 and HIV-1 subtypes was conducted using Pearson's chi-squared or Fisher's exact tests. Drug resistance mutations with univariate p-values less than 0.3 with respect to HIV-1 subtype were selected as candidates for multivariate modeling. The association between each drug resistance mutation and HIV-1 subtype, adjusting for time on ART, total number of drug resistance mutations, and ART regimen, was assessed by fitting a multivariate logistic regression model in which HIV-1 subtype was represented in the form of an indicator variable. A postestimation Wald test was used to evaluate the effect of regimen indicator variables as a set in the model. Additional analyses evaluating the influence of gender and specific clinic sites were explored but did not impact the multivariate model and were not included in the final model. Model building and assessment of fit proceeded along the lines recommended by Hosmer and Lemeshow. 33 p-values less than 0.05 were considered significant. Statistical analyses were performed using Stata software (version 9.2, Stata Corporation, College Station, TX).
Results
Baseline characteristics of the study population
A total of 338 patients were categorized by antiretroviral regimen from entry into the APIN Plus/PEPFAR program to the time of genotyping. At study entry, 189 patients (55.9%) were already receiving Government of Nigeria ART consisting of d4T + 3TC + NVP or drugs from a private source and 149 patients (44.1%) were ARV naive. The median time on ART for drug-experienced patients was 33.2 months. For patients entering the program as drug-naive, the median time on therapy was 13 months. Table 1 presents the distribution of patients by months on ART treatment and by ART experience.
Distribution of patients by time on antiretroviral therapy, stratified by ART experience on entry in the PEPFAR program; 189 patients were ART experienced at entry and 149 were naive.
Table 2 describes the distribution of patients by the NRTI and NNRTI components of their ART regimens. The most common regimen was d4T + 3TC + NVP, followed by zidovudine (AZT)-containing and tenofovir (TDF)-containing regimens. Among NNRTIs, NVP was far more frequently prescribed (91.1%) than efavirenz (EFV), which accounted for only 8.9% of patients.
Categorization of patients by treatment regimen within the PEPFAR program. The same set of patients is stratified by the NRTI backbone of their treatment regimen (whether a single regimen throughout the study period or multiple regimens due to changes) and also by the NNRTI component of their treatment.
The gender distribution profile in the study sample differed from that of the study population. Women made up 40% of the study sample, whereas they account for 64% of the patients on ART in our program. 34 Due to this difference, we investigated whether gender was associated with drug resistance development. Univariate analysis showed that men were more likely than women to have the V75M (p = 0.045) and Y188C mutations (p = 0.002). However, multivariate analysis revealed that gender had no noticeable effect after controlling for time on therapy, total number of mutations, and drug regimen, and was therefore dropped from further analysis.
Subtype by geographic location
HIV-1 subtype was determined based on phylogenetic analysis of pol gene sequences. Of the 338 patients in the study sample, 152 (45.0%) were CRF02_AG, 128 (37.9%) were subtype G, 15 (4.4%) were CRF06_cpx, 12 (3.6%) were subtype A, and the remaining 31 (9.2%) patients had other subtypes or recombinant sequences. A variant of subtype A, subsubtype A3 (originally described in Senegal), has been reported in other West African countries including Nigeria. 35 Subsubtype A3 represented 9 of the 12 subtype sequences evaluated with the remaining sequences classified as A1. Among the 128 subtype G sequences, 94 (73.4%) formed a unique monophyletic subcluster referred to as G′. 35,36 We have previously observed this unique subcluster, which has been shown by full-length sequence to have an average diversity of 7.7% within G′ sequences, while differing by 9.5% from prototypical subtype G sequences. 37
The distribution of the five non-B subtypes was not random and appeared to vary in association with a roughly north–south gradient in the country (Fig. 1). Subtype G was more prevalent in the northernmost site at the University of Maiduguri Teaching Hospital in Borno State with a relatively smaller proportion in Jos, located in the north-central belt region, while the lowest proportions were found in the southwest region, where Lagos and Oyo states are located. Conversely, the proportion of CRF02_AG was highest in the southwest and decreased in sites situated in the middle belt and northern regions of the country. Removing miscellaneous recombinant forms from the analysis, HIV-1 subtype was associated with sites based on a north versus south gradient (Fisher's exact test, p = 0.019).

Subtype distribution in HIV among Nigerian patients selected for resistance testing. Color images available online at
Drug resistance mutations
The most common NRTI mutation was M184V (301, 89.1%) (Table 3). Thymidine analog mutations (TAMS) were prevalent in 8–27% of viruses examined and K65R was seen in 37 viruses (10.9%). The median number of mutations was five and the mode was three. Figure 2 shows the most common NRTI mutations stratified by NRTI backbone. Of note, the T69 deletion, an uncommon mutation that in the context of virus with multidrug resistance has been shown to improve the replication capacity of the resistant virus, 38 –40 was present in only seven patients on d4T-based therapy. In six of those seven, the K65R mutation was also present.
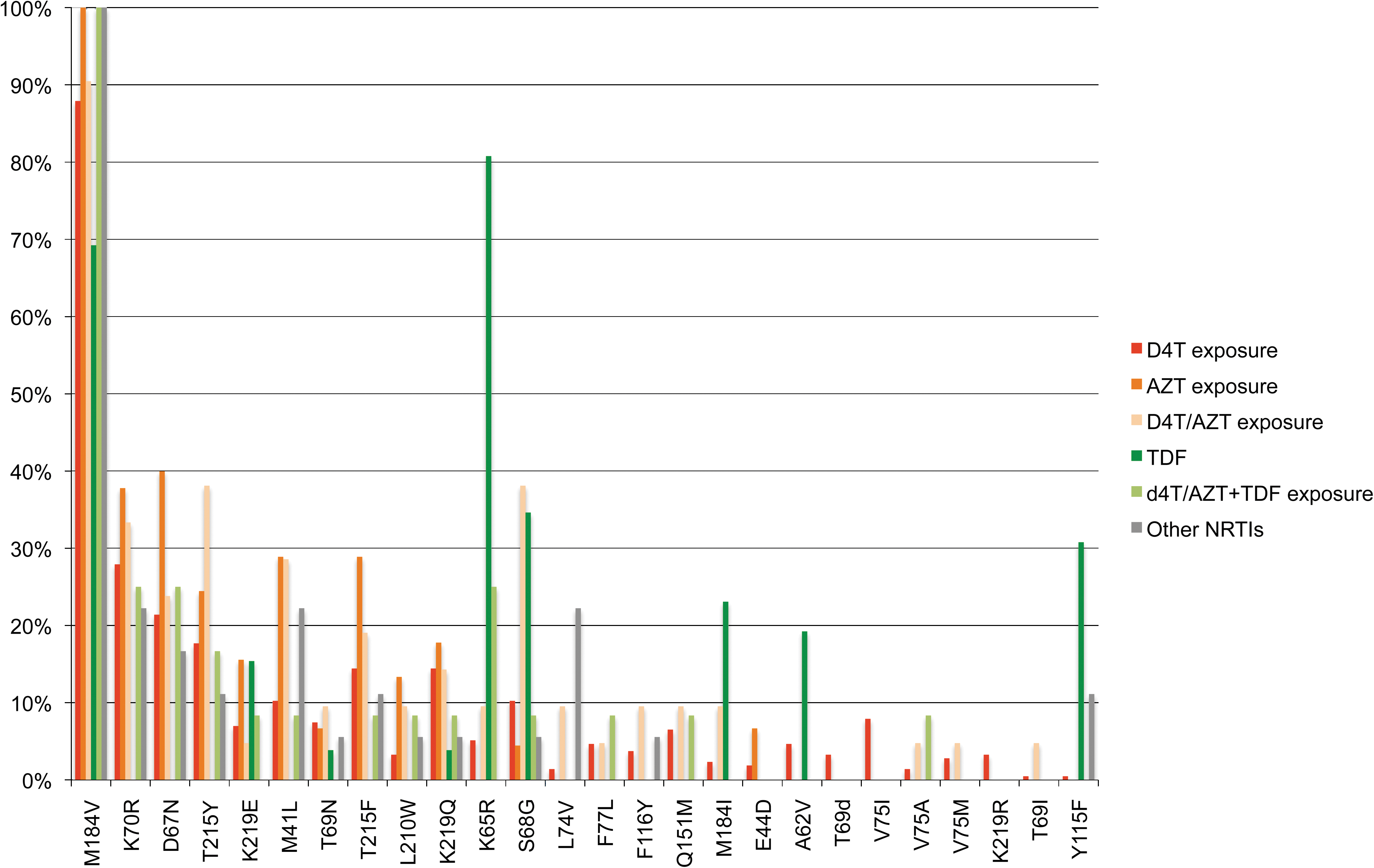
Frequency of NRTI mutations, by NRTI exposure. Color images available online at
Frequency of most common NRTI mutations in relation to exposure to tenofovir or to AZT and/or d4T while on ARV treatment in the PEPFAR program and to most common NNRTI mutations. Frequencies are reported in the total study population of 338 patients, 27 patients who were exposed to tenofovir, and 281 patients who were exposed to stavudine or zidovudine.
Subtype-specific differences in reverse transcriptase
Multivariate analysis revealed a number of statistically significant associations between NRTI mutations and certain subtypes after controlling for time on ARV therapy, total number of drug resistance mutations, and ART regimen (Table 4). CRF02_AG patients were less likely to have the M41L mutation compared to other subtypes [adjusted odds ratio (AOR) = 0.35; p = 0.022]. Patients categorized as subtype G′ were more likely to have the M41L mutation (AOR = 3.08, p = 0.015), and CRF06_cpx patients demonstrated a similar but nonsignificant trend (AOR = 4.37, p = 0.081). Subtype A patients showed a 42.5-fold increased risk (AOR = 42.5, p = 0.001) for the L210W mutation compared to other subtypes, whereas G′ patients showed a nonsignificant trend toward lower risk for this mutation (AOR = 0.22, p = 0.077). Regimens containing zidovudine (ZDV) were associated with both the M41L and L210W mutations, independent of subtype (p < 0.02). In addition to subtype, total number of mutations was significantly associated with M41L and L210W: each additional mutation doubled the odds of the patient having the M41L (AOR = 2.3, p < 0.0001) or L210W mutations (AOR = 2.0, p < 0.0001).
Results of logistic regression analysis controlling for regimen (NRTI backbone for M41L and L210W, NNRTI backbone for V90I, A98G, and V106I), time on therapy, and total number of mutations. Adjusted odds ratios (AOR) and p-values <0.05 are shown; p-values >0.05 were considered not significant (NS). AORs with p-values >0.05 but <0.1 are shown in italics.
Similarly a multivariate analysis for NNRTI mutations showed a difference in V90I, A98G, and V106I by HIV-1 subtype (Fig. 3). Subtype G patients had an increased risk for A98G (AOR = 2.40, p = 0.036) and V106I (AOR = 6.15, p = 0.010), whereas subtype CRF02_AG had an increased risk for V90I (AOR = 3.16; p = 0.003) and a decreased risk for A98G (AOR = 0.48, p = 0.019).
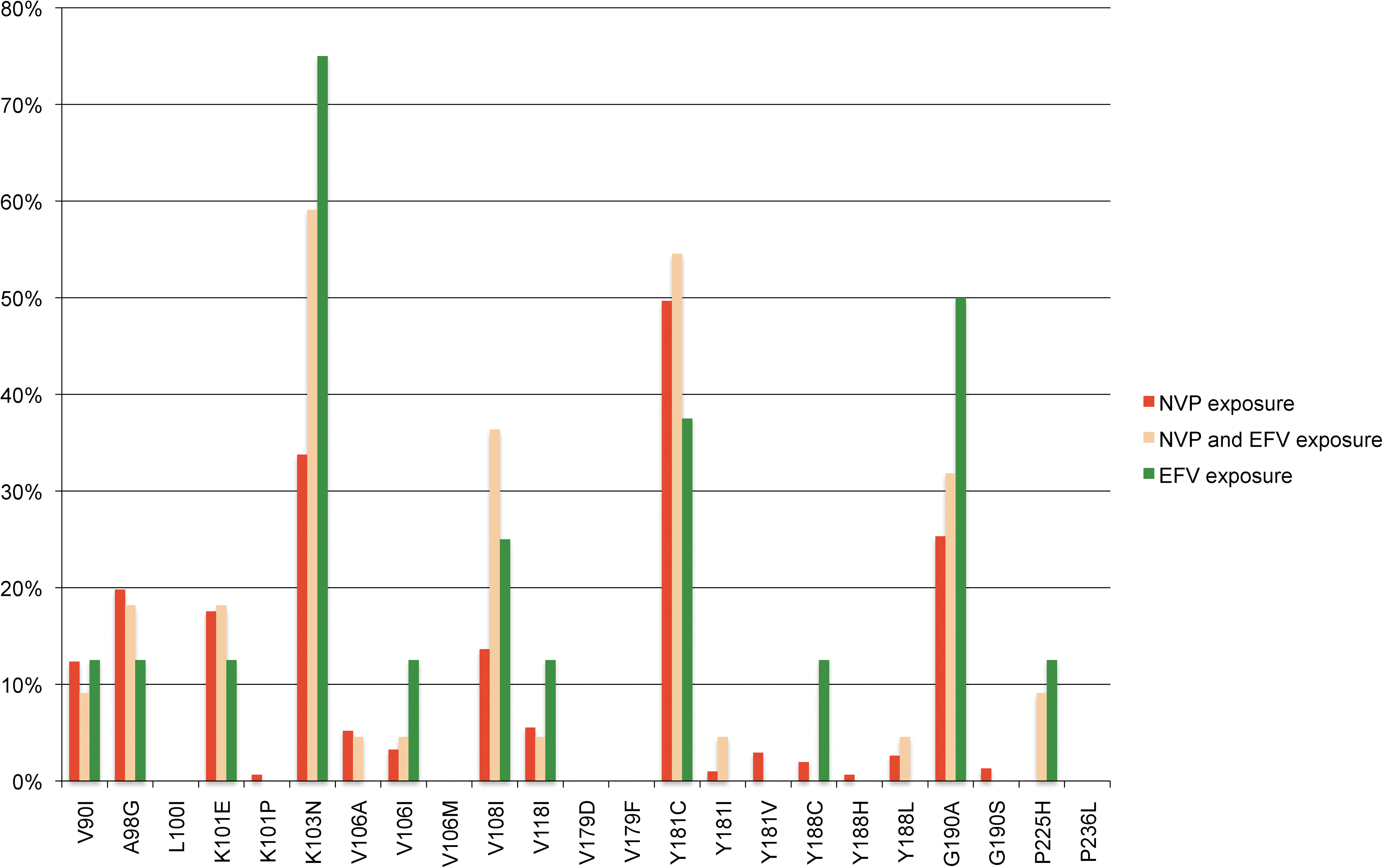
Frequency of NNRTI mutations, by NNRTI exposure. Color images available online at
Subtype-specific differences in protease
Genotypes were examined in patients on first-line failure with no exposure to protease inhibitors (PI). Three mutations in the protease gene were observed in 90–100% of all five non-B subtypes evaluated, in striking contrast to a low frequency or complete absence in subtype B: these included I13V, M36I, and H69K (Table 5). The K20I mutation was seen in 93–100% of subtypes G′, G, CRF02_AG, and CRF06_cpx, yet is completely absent in subtypes A and B. Other mutations included L10I, G16E, K20R, I64M, and V82I with subtype-specific differences.
Number and percentage of protease polymorphisms present in ≥25% of patients in a specified subtype and significantly higher than in subtype B PI-naive patients. Thirty-four patients are classified as subtype G, 94 as G′, 152 as CRF02_AG, 15 as CRF06_cpx, and 12 as A.
Based on the assessment by the Stanford HIV Database, five patients had intermediate resistance to more than one PI, including atazanavir, fosamprenavir, indinavir, nelfinavir, saquinavir, and tipranavir. One of those patients was also highly resistant to nelfinavir, conferred by the presence of L90M. 41
Discussion
The HIV-1 subtypes found in the ART-treated patients in this study were CRF02_AG, G, CRFO6_cpx, and A. Other recombinant viruses that could not be classified or subtypes present in small numbers were observed in 9.2% of all viruses typed. These subtypes and their distribution are similar to what has been described in Nigeria and other West African countries. The most common subtypes in the study population were CRF02_AG and G, with the majority of the subtype G sequences belonging to the subcluster G′. The distribution of these subtypes followed a north–south gradient in the population surveyed, with CRF02_AG constituting more than 50% of the infections observed in Lagos State. Approximately equal proportions with subtype G were in evident in Oyo and Plateau States, and subtype G was more prevalent in the north. CRF06_cpx and A were present at lower and similar proportions in all sites surveyed. The heterogeneous nature of subtypes and their distribution in West Africa have been described 42 and national HIV sentinel surveillance surveys conducted in all 36 states of the Federation have demonstrated higher prevalence rates in the central belt and northern regions of the country. 25 This, coupled with the higher proportion of subtype G in these regions, might suggest that this subtype entered this region of the country earlier than other subtypes, initiating an epidemic that predated the subtype CRF02_AG epidemic. Although these subtypes are genetically closely related, the distinct geographic distributions may indicate differences in epidemiologic origin, impact of migration, and determinants for differential transmission and fitness.
In ART treatment programs in resource-limited settings a significant proportion of the patients are women. In our program in Nigeria we have provided ART to 48,754 patients with 60% being women. The patients evaluated in this study were selected based on virologic failure, and the slightly higher proportion of men suggested potential differences in time to failure based on gender. We have recently analyzed viral suppression at 6 and 12 months of therapy by gender and found that women showed a statistically significant higher rate of viral suppression compared to men. This effect was largely driven by better drug adherence in women in the first 12 months of treatment. 34 Although our univariate analysis indicated certain drug resistance mutations (V75M and Y188C) were more common in men, these associations were not significant in multivariate analysis. It seems likely that gender differences in response to therapy could lead to more rapid drug resistance mutations in men, perhaps in mutations more sensitive to drug adherence, but the addition of gender to our multivariate analysis failed to demonstrate an independent effect of gender on mutation development.
Genotyping for the samples used in this study was performed as part of a clinical care program, and patients were tested at varying lengths of time after virologic failure. Therefore it is likely that time on therapy as noted in this study was an overestimate of the time to drug resistance development. The mean length of time on therapy was 25.8 months. Certain uncommon mutations noted in this data set, such as the T69 deletion, were found in patients on therapy for a median of 27.2 months, slightly longer than the population median of 25.8 months. Therefore, this mutation may occur after prolonged time on therapy and further study with longer follow-up is warranted.
Drug resistance mutations for NRTI drugs were found in the majority of patients (95.9%). In general, the mutations observed were similar to what has been described for subtype B viruses, including M184V/I, K70R, D67N, and T215Y/F as the most common. 31 For patients on tenofovir-containing regimens the most common mutations were similar between non-subtype B patients compared to mutations seen in subtype B. 43 The presence of these major NRTI drug mutations would signify multidrug resistance to most NRTI drugs, compromising the use of this class of drugs in second-line drug regimen choices. We did not find subtype-specific associations with the most common drug resistance mutations observed, such as M184V/I.
L210W was more common in subtype A than in the other subtypes surveyed by an adjusted odds ratio of 42.5 (p = 0.001). One explanation for this may be that the baseline nucleotide sequence at this position in subtypes G and CRF02_AG usually requires two mutations, a transition and transversion, whereas only one transversion is required to achieve this mutation in subtype A; thus the genetic barrier for this mutation is higher in CRF02_AG and G and this is also reported for subtype B. 44 M41L, another TAM, occurred less frequently in CRF02_AG than other subtypes (AOR = 0.35, p = 0.022), and more commonly in G′ compared with other subtypes (AOR = 3.08, p = 0.015); however, this could not be explained by underlying differences in baseline nucleotide sequence.
The TAM mutations in subtype B increase resistance to ZDV and d4T by increasing the proofreading ability of the HIV RT. The development of these mutations follows two pathways; the TAM I pathway, characterized by T215Y, is accompanied by M41L and L210W. The TAM II pathway is characterized by T215F, K70R, and K219QE, 45 and is less frequently observed in subtype B-treated patients. A negative association between the polymorphism L214 and the TAM I mutations M41L, T215Y, and L210W has been previously reported, 46,47 and this same association was observed in the viruses we examined from Nigeria. Although 71% of patients had leucine at position 214 overall, this mutation had a negative correlation with the presence of TAM I mutations: 18% with one TAM I mutation, 10% with two TAM I mutations, and 8% with three TAM I mutations. When subtype was compared with the presence or absence of L214, there were no differences observed in the proportion of L214 in G′, CRF02_AG, CRF06_AG, or A that would explain the differences in M41L or L210W noted by multivariate analysis.
In Botswana, a variation of the TAM pathway has been described, 67N/70R/215Y. 48 This appears to be specific to the d4T/ddI exposure in this country since similar results were not found in other subtype C studies in South Africa, Malawi, and India where other drug regimens were used. 49
A 2005 meta-analysis of 3686 persons with non-B subtypes and 4769 with B subtypes found that 55 known treatment-associated mutations that were observed in subtype B were also found in non-B subtypes, and the converse was true for 61/67 mutations observed in non-B subtypes. 50 In contrast, a study by Palma et al. in 2009 found that genetic background played a role in different treatment-associated mutations that developed in subtypes B and G in Portuguese patients. 51 In a study of patients from Rio Grande do Sul, Brazil, in a population infected by subtypes B and C, a lower rate of accumulation of mutations was found in subtype C than subtype B. 52 However, certain NRTI mutations such as K65R have been shown to develop more quickly in subtype C than in other subtypes. 13
NNRTI-associated mutations were found in 98.5% of patients in virologic failure. The most common NNRTI mutations observed in our patients were Y181C, K103N, G190A, and A98G, similar to what has been described in subtype B infection. Three NNRTI mutations were found to be associated with subtype in the logistic regression model: V90I was more likely to occur in CRF02_AG than other subtypes by adjusted odds ratios of 3.16, and A98G and V106I were more likely to occur in G with adjusted odds ratios of 2.40 and 6.15, respectively. An increased frequency of the V90 after therapy in subtype C-infected patients has been previously observed. All three of these mutations confer resistance to etravirine, a potential second-line NNRTI. 53
Some minor mutations in the PR gene are the consensus in untreated non-B subtypes. In these PI-naive Nigerian patients, I13V, M36I, and H69K were the wild-type consensus sequences for G′, G, CRF02_AG, CRF06_cpx, and A, K20I was the consensus for G′, G, CRF02_AG, and CRF06_cpx, and V82I was the consensus for G′ and G. In addition, the mutations L10I, G16E, and K20R occurred in ≥25% of subtype A patients, at a proportion that is significantly greater than in subtype B, and I64M occurred in ≥25% of CRF06_cpx patients surveyed. Based on codon bias and genetic barrier considerations, CRF02_AG and subtype G viruses are differentially more likely to develop L10V and L10I drug resistance mutations, respectively. 50,54 Some of these non-subtype B-specific protease polymorphisms have been previously noted, but studies of non-subtype B patients on PR inhibitor regimens are uncommon in the literature so that the clinical significance of these baseline minor mutations is still being evaluated. 15,16,18,51 Although none of the subtype-specific polymorphisms in the PR are considered major PI mutations, many are minor mutations to PR inhibitors commonly used in resource-limited settings such as Nigeria, including indinavir/ritonavir and lopinavir/ritonavir.
We performed genotyping on patients on first-line ART with evidence of virologic failure in a resource-limited setting where rapid scale-up of ART is underway. Five non-B HIV-1 subtypes were found in all six clinical centers, although proportions appeared to vary geographically. The distribution and frequency of NRTI and NNRTI mutations were generally similar to what has been described for subtype B. Among the most common drug mutations found, there was no apparent association with HIV-1 subtype. Therefore, in large part, we can anticipate that drug resistance development to the first-line regimens in Nigeria will largely follow what we understand from studies of subtype B. Two NRTI TAM I mutations (M41L and L210W) and three NNRTI mutations (V90I, A98G, L210W) were found to be significantly associated with an array of non-B West African subtypes. Variation in the TAM pathways in non-subtype B viruses is not unexpected given their baseline genetic diversity; however, the impact on the durability of ART efficacy is yet to be appreciated.
Further study is needed to determine the clinical significance of the subtype-specific PR gene polymorphisms on the development of PR inhibitor resistance in non-B West African subtypes. Because PR inhibitors are the predominant class of drugs used for second-line therapy in resource-limited settings, it will be critical to assess the impact of the viral genetic diversity on treatment efficacy. These results have enhanced our understanding of the extent of drug resistance in this population and provided insight into subtype-specific drug resistance that may be useful to inform ART regimen policy.
Sequence Data
Sequences have been deposited in the GenBank Sequence Database under the following accession numbers: FJ931123–FJ931460.
Footnotes
Acknowledgments
We would like to acknowledge and thank all patients and staff in the AIDS Prevention Initiative in Nigeria Plus (APIN Plus) Harvard PEPFAR program. Financial support was provided by the National Institutes for Health, UO1 AI025915, AIDS Prevention Initiative in Nigeria, Bill and Melinda Gates Foundation, and the Health Resources and Services Administration, U51HA02522. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the funding institutions.
Author Disclosure Statement
No competing financial interests exist.