
Abstract
Natural polymorphisms of HIV-1, often associated with drug resistance, are widely described in protease and reverse transcriptase regions but data on their presence in the integrase region, especially in non-B subtypes, are still very limited. We aimed to characterize naturally occurring polymorphisms in the integrase region in 104 treatment-naive and 10 treatment-experienced patients infected predominantly with HIV-1 CRF06_cpx and its recombinant with subtype A1 and/or CRF03_AB viruses. No primary drug resistance mutations against integrase inhibitors were found, but resistance-associated polymorphisms such as V72I, L74I, V201I, and T206S were seen in more than 90% of viruses. Substitutions E157Q and E157K, associated with raltegravir resistance, were found in only two CRF06_cpx strains. We conclude that similar to other HIV-1 non-B subtypes, the CRF06_cpx and its recombinants with subtype A1 and CRF03_AB are rich in integrase region natural polymorphisms, which may impact the development of resistance against integrase inhibitors.
T
The Estonian concentrated HIV-1 epidemic begun in August 2000 when the number of infected subjects rose rapidly reaching the highest prevalence (to 1053 per million inhabitants) in the European Union in 2001.
1
Although in recent years the rate of new infections has diminished, there are still about 500 new cases per million reported each year (
The studies conducted thus far have demonstrated the presence of several natural polymorphisms in the integrase region associated with resistance to INIs. 3 –5 Most of these studies, however, have included either subtype B or widely spread subtypes such as A, C, F, and CRF01 and CRF02 viruses. 4 –6 The data on other subtypes and circulating recombinant forms are still very limited.
We aimed to describe the presence of naturally occurring polymorphisms in the integrase region in HIV-1 CRF06_cpx and its recombinants with subtype A and CRF03_AB viruses isolated from antiretroviral (ARV) naive and experienced individuals in Estonia. The samples were collected from 2005 to 2006 from subjects infected during the concentrated HIV epidemic (
Briefly, RT-PR and IN region HIV-1 RNA reverse transcription was carried out using 0.4 μM antisense primer JA272degen (5′-GGATAAATMTGACTTGCCCART-3′) and antisense primer INREV-Idegen (5′-TCTCCTGTATGCAGACCCCAATAT-3′), respectively. Nested polymerase chain reaction (PCR) was carried out using primers JA269degen (5′- AGGAAGGMCACARATGAARGA-3′), JA272degen, JA270 (5′-GCTTCCCTCARATCACTCTT-3′; NT), and JA271 (5′-CCACTAAYTTCTGTATRTCATTGAC-3′) for the RT-PR region and primers INFORIdegen (5′-GGAATYATTCARGCACAACCAGA-3′), INREV-Idegen, HIV +4141degen (5′-TCTAYCTGKCATGGGTACCA-3′), and INREVII (5′-CCTAGTGGGATGTGTACTTCTGA-3′). Sequencing was performed by second round primers and four additional primers in the RT-PR region: JA273 (5′-CCCTCAAATCACTCTTTGGC-3′), JA274 (5′-AAAATCCATACAATACTCCA-3′), JA275 (5′-TTATTGAGTTCTCTGAAATC-3′), and JA276 (5′-TGTATATCATTGACAGTCCA-3′).
TE population RT-PR sequences were submitted to the Stanford HIV Drug Resistance database (
Phylogenetic trees were constructed using IN region sequences and reference seguences from the Los Alamos HIV database (
The amino acid polymorphisms in every IN position were analyzed using the subtype B consensus sequence from the Los Alamos HIV sequence database (
The study included a total of 104 TN and 10 TE subjects; 74 (84%) were male and 58 (66%) were intravenous drug users (IDUs). The median age was 26.8 (IQR = 23.3–30.3) years. Among TN and TE populations the median viral load was 175,200 copies/ml and 63,163 copies/ml and the median CD4 cell count was 414 cells/μl and 174 cells/μl, respectively.
In the phylogenetic analysis the majority of sequences in TN (89/104) as well as in TE (7/10) populations formed a monophyletic branch with the recently sequenced Estonian and Russian HIV-1 CRF06_cpx strains (Fig. 1). There were only two sequences in the TE and one in the TN population that had the closest similarity to the subtype B, CRF02_AG, and subtype A1 reference sequences, respectively. A total of 14 sequences in the TN and one in the TE population were obvious recombinants between different reference strains and thus were excluded from the phylogenetic tree construction. They were analyzed with SimPlot software, which revealed a complex recombinant structure between CRF06_cpx, CRF03_AB, and subtype A1 of these 14 viruses.
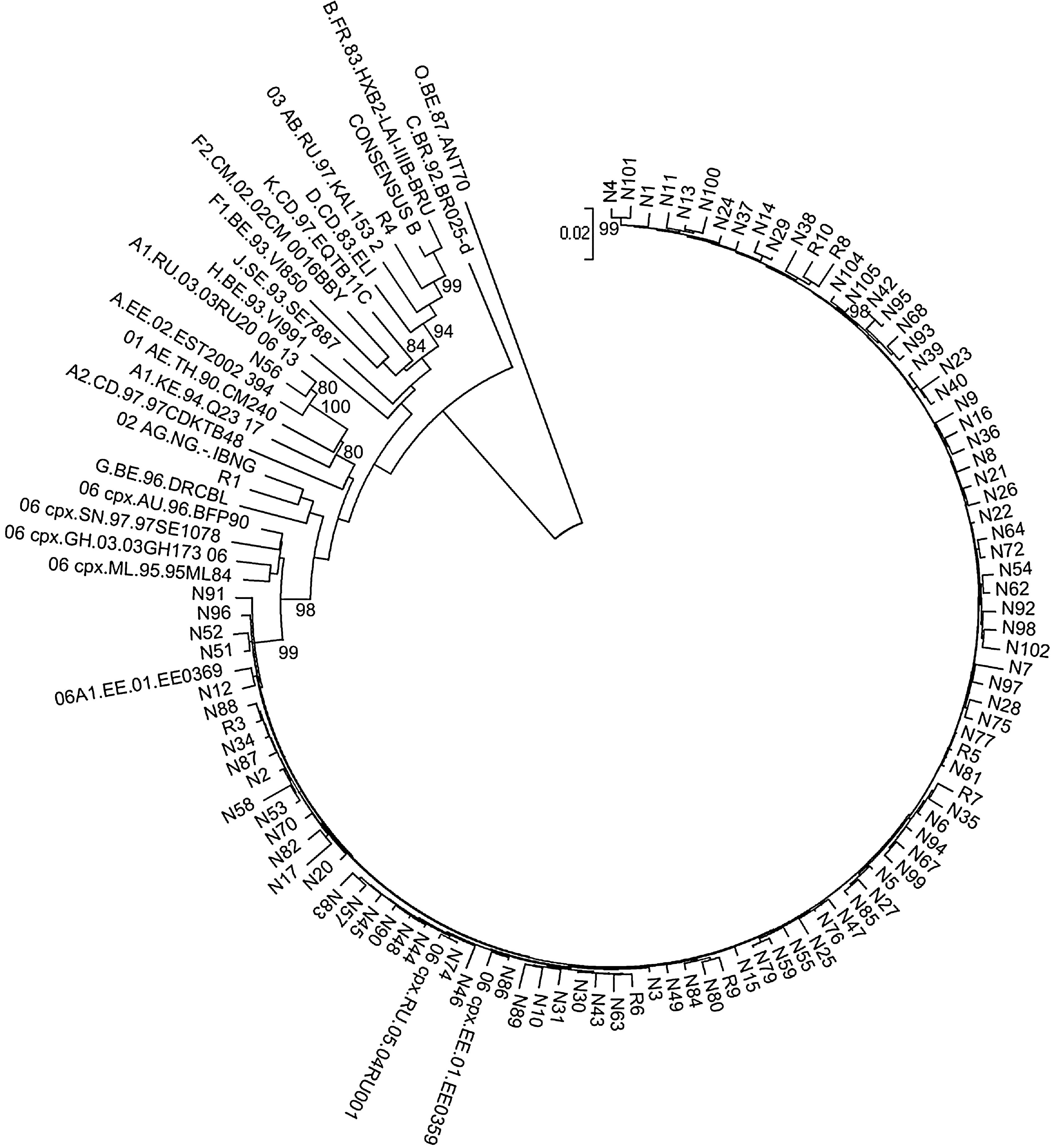
Neighbor-joining (NJ) tree of 104 TN and 10 TE Estonian HIV-1 IN regions. Reference sequences of all subtypes, CRF01_AE, CRF02_AG, CRF06_cpx, and some sequences related to Estonian (designated as EST) or former Soviet Union (designated as FSU) HIV-1 epidemics described before by Adojaan et al. (2005) are added. 15 The tree is rooted by the HIV-1 group O reference sequence. Bootstrap values higher than 70% are shown. A genetic distance scale of 0.02 is indicated. Estonian HIV-1 IN sequences from the TN population are indicated with an “N” and from the TE population with an “R.” Estonian IN sequences form a monophyletic cluster with earlier Estonian and Russian CRF06_cpx sequences. Recombinant sequences in the IN region between CRF06_cpx and subtype A1 and/or CRF03_AB were excluded from the figure. Additionally, one TN population's viral sequence clusters together with FSU subtype A1 sequences and two TE population's viral sequences cluster together with subtype B and CRF02_AG sequences, respectively.
In the TN population of 288 integrase aa 207 (72%) were absolutely conserved; in 55 (19%) positions the predominant aa was spread to more than 95% of sequences and the polymorphic positions (the most predominant aa was spread in fewer than 95% of sequences) accounted for 26 (9%) cases. In the TE patients 250 positions (87%) were absolutely conserved. In both populations functional positions (DDE, HHCC, and extended active site residues) were absolutely conserved except for polymorphisms E92K, I141V, and V151I in the TN population seen in single cases only. In LEGP/p75 binding residues polymorphisms H171L, H171Y, and D167E were detected in one, one, and seven cases, respectively. Mean aa pairwise distances in IN sequences were 0.028 and 0.044 in the TN and TE populations, respectively. Mean aa pairwise distances of CRF06_cpx sequences were 0.025 in the TN and 0.028 in the TE populations. The distance within the cluster of CRF06_cpx recombinant forms with other subtypes was 0.038. Table 1 shows the prevalence of aa polymorphisms in comparison to consensus reference sequences of subtype B.
The superscript indicates the percentage of sequences that possesses the indicated amino acid different from the subtype B consensus sequence. The same amino acids as the subtype B consensus have not been indicated.
We did not find any primary DRMs, but identified several accessory mutations and natural polymorphisms associated with INI drug resistance. The accessory mutations L74I and V72I were common and presented in more than 90% of the entire population and more than 95% in the CRF06_cpx population. The substitution V72I is known as a consensus aa in the subtype B, but has also been outselected in strains in which isoleucine is not a wild-type residue. Other accessory mutations E138K, V151I, E157Q, G163R, and I203M were seen in single cases only. Among polymorphisms so far associated with INI drug resistance in vitro only the V201I and T206S were consensus aa showing prevalence rates of more than 95% in the whole as well as the CRF06_cpx population; polymorphisms V249I and V165I were found in single cases.
In this study mutations V72I, L74I, T206S, and V201I were very common and were seen in more than 90% of viruses. With this CRF06_cpx viruses differ from the subtypes B–D, F, G, CRF01_AE, and CRF02_AG in which the frequency of the L74I polymorphism in less than 20% and the T206S has been found only in subtypes G and CRF02_AG
6,8
(
Some of the subtype-specific polymorphisms (e.g., V72I, L74I, T206S, and V201I) have been selected by earlier ARV compounds, but the significance of these residues under pressure of the current generation INIs is largely unknown. A large in vitro study suggested that the clade-specific polymorphisms in the IN region do not affect the susceptibility to INIs. 10 These finding were further affirmed in the RAL phase III clinical trials, indicating no influence of HIV subtype on the treatment response to INIs. 11
It still remains unknown whether the efficacy of INIs is affected by the selection pressure of previous ARV therapy with RTIs or PIs. The physical interactions between RT and IN may induce aa covariations of these enzymes, especially in the case of the emergence of RT DRMs, and thus induce mutations in the IN region. 12 Similar to previous researchers we were unable to show any associations between the presence of RT DRMs and substitutions in the IN region suggesting the potential use of INIs as salvage therapy in patients failing ARV therapy as demonstrated in recent clinical trials. 13,14 Still, based on these results no definite conclusions can be drawn because of the low number of TE patients and the diverse pattern of PR and RT DRMs.
In conclusion, the phylogenetic analysis of the IN region confirmed results of earlier studies in the gag and env genes indicating that the Estonian epidemic is monophyletic and predominantly caused by CRF06_cpx viruses or by its recombinants with Eastern European subtype A1. 1,7 We did not identify any major DRMs to RAL or ELV in viruses circulating in INI treatment-naive populations in Estonia. However, four polymorphisms (L74I, V72I, V201I, and I206S) potentially associated with the resistance pathways were commonly present and their frequency in CRF06_cpx and its recombinant viruses differed from that in other HIV-1 subtypes. Whether the presence of these mutations would impact the response to INIs and trigger faster than usual resistance development remains to be determined in future clinical trials.
Sequence Data
The nucleotide sequences of IN regions have been submitted to GenBank and the accession numbers are GQ926737–GQ926850.
Footnotes
Acknowledgments
The authors are grateful to Maarit Maimets for critical manuscript review. Grant sponsors: the Center of Excellence of Translational Research of Neuroimmunology, the Basic Financing and the Target Financing of Estonian Ministry of Education and Research, Grant number SF0182726s06, the European Union (European Regional Development Fund), and the Archimedes Foundation.
Author Disclosure Statement
No competing financial interests exist.