
Abstract
The rate of virological failure was assessed in 819 patients followed up by the private sector of Douala, the economic capital of Cameroon, and treated according to the World Health Organization (WHO) recommendations. In addition, genotypic resistance testing was carried out in the subgroup of 75 selected patients representative of the 254 patients in virological and/or immunological failure receiving a first-line (83%) or second-line (17%) regimen. Overall, 36% of patients treated by antiretroviral drugs (ARV) were in virological failure, as assessed by plasma viral load above 3.7 log10 copies/ml under treatment for more than 6 months. According to the immunological status, 17% of patients showed a CD4 T cell count under 200 cells/mm3 and 37% under 350 cells/mm3, indicating either ongoing immunorestoration or immunological failure under treatment. Twenty percent of patients in virological failure showed wild-type viruses susceptible to all ARV, likely indicating poor adherence. However, 80% of them displayed plasma virus resistant at least to one ARV drug, mostly to the nucleoside reverse transcriptase inhibitors (NRTIs) class (80%), followed by the non-NRTI class (76%) and the protease inhibitor class (19%), thus reflecting the therapeutic usage of ARV drugs in Cameroon as recommended by the WHO. Whereas the second-line regimen proposed by the 2009 WHO recommendations could be effective in more than 75% of patients in virological failure with resistant viruses, the remaining patients showed a resistance genotypic profile highly predictive of resistance to the usual WHO second-line regimen, including in some patients complex genotypic profiles diagnosed only by genotypic resistance tests. In conclusion, our observations highlight the absolute need for improving viral load assessment in resource-limited settings to prevent and/or monitor therapeutic failure.
Introduction
T
The HIV epidemic in Cameroon is basically generalized, with an overall prevalence of 5.6% throughout the country. 5 Whereas the healthcare of Cameroon's patients was principally devoted to the public sector, original important private sector initiatives have carried out prevention and antiretroviral (ARV) treatment activities since the beginning of 2000. The Cameroon Business Coalition against HIV/AIDS, tuberculosis, and malaria, including the so-called GICAM (Groupement Interpatronal du Cameroun) representing the employers' federation, was formally launched in March 2006 to elevate the private sector response from a company-level working group to a national initiative. In Cameroon, 71% of the structures delivering antiretrovirals are public, 11% are private (private hospitals and healthcare services of the large companies), 16% are from the private nonprofit system, and 2% are from the security-associated sector (police, jails, and the armed forces). 6 Whether the private sector allows efficient care and treatment of HIV-infected patients has been poorly documented in sub-Saharan Africa.
The high genetic diversity in HIV-1 subtypes, comprising a high proportion of natural polymorphisms, among which certain positions are associated with resistance, increased the complexity in the management of ARV therapy in sub-Saharan Africa.
7
A high level of HIV
The aim of the present study was to assess the rate of virological failure and the selection of HIV-1 variants resistant to ARV drugs in patients followed up by the private sector of Douala, the economic capital of Cameroon, where the private sector has now assumed a large place in the healthcare services of HIV-infected individuals. The drug resistance study was performed for 75 patients, mostly infected with a CRF02_AG HIV-1 recombinant, and displaying therapeutic failure with uncommon ARV drug resistance profiles.
Materials and Methods
Study patients
HIV-infected patients receiving an ARV-containing regimen followed up in the ARV access program in Douala (DARVIR) for biological analyses in Litto-Labo, one of the main private laboratories for HIV monitoring in Douala, were studied. Indications for ARV treatment were based on the World Health Organization (WHO) 2006 revised criteria for adults and adolescents. 16 Patients receiving an ARV-based regimen for at least 6 months, with one measurement of HIV-1 plasma viral load and two measurements of CD4 T cell counts, were consecutively included from January 2007 to September 2008.
Virological and immunological monitoring
Plasma HIV-1 RNA viral loads were determined by a commercial assay: NucliSens EasyQ (bioMerieux, Boxtel, The Netherlands) at the laboratory Litto-Labo held in Douala, Cameroon. CD4 T cell counts were measured by flow cytometry using the Partec CyFlow Counter (Partec GmbH, Munster, Germany).
Genotypic resistance testing
A genotypic resistance test was carried out between January 2007 and September 2008 for a subgroup of selected (one out of three) HIV-treated patients harboring one or two criteria of virological (e.g., HIV-1 RNA load above 10,000 copies/ml) or immunological failure according to the WHO recommendations.
16
Genotypic analysis of the reverse transcriptase (RT) and protease (PR) HIV genes was performed at the virology laboratory of Georges Pompidou European Hospital, Paris, France, with the commercial assay ViroSeq (Celera Diagnostics, Alameda, CA) used on plasma samples, transported frozen in dry ice. ARV drug resistance mutations were identified and interpreted according to the Agence Nationale de Recherches sur le SIDA et les hépatites virales (ANRS) algorithm, updated July 2009 (
Phenotypic resistance testing
Some of the samples exhibiting mutations conferring resistance to protease inhibitors (PIs) were subjected to a phenotypic resistance test. Phenotypic resistance tests were performed using the vircoTYPE assay (version 4.1). Results of the assay are expressed as the fold change (FC) of inhibitory concentration 50% (IC50) values between the tested virus and a wild-type reference virus. All available PI, nucleoside reverse transcriptase inhibitors (NRTIs), and nonnucleoside reverse transcriptase inhibitors (NNRTIs) were tested.
Results
HIV-1 RNA viral load and CD4 T cell count in the study population
During the 21-month study, 819 HIV-infected patients (401 males and 418 females) received their HIV monitoring in Litto-Labo, including HIV-1 RNA viral load and CD4 T cell count. The median duration of ARV treatment in study patients was 4.3 years (ranges, 1–6 years). Most patients (91%) were receiving their first-line ARV drug regimen, whereas a minority of them received second-line (7%) or third-line (2%) ARV therapy. The ARV regimen consisted of 2006 WHO recommended ARV treatment, mainly including zidovudine (AZT), lamivudine (3TC), and NNRTIs in the first-line regimen, and a PI-containing regimen, mainly with indinavir (IDV), and, when available, lopinavir (LPV) boosted with ritonavir in a second-line regimen.
The distribution of plasma viral load levels in the study patients is depicted in Fig. 1A. Forty-nine percent of patients showed undetectable HIV-1 RNA viral load (<1.7 log10 copies/ml), exhibiting virological success. Seven percent of patients showed low-level viremia, below log10 3.0 copies/ml, likely due to possible transient viral blips. Thirteen percent of patients displayed moderately elevated HIV-1 RNA viral load, between log10 3.0 and 4.0 copies/ml. Unfortunately, a second determination of HIV-1 viral load was generally not carried out in these latter patients; but their medical care, mainly focusing on a better observance of the same ARV regimen, was reinforced to prevent therapeutic failure. Finally, 31% of patients had a plasma HIV-1 RNA viral load above log10 4.0 copies/ml, exhibiting virological failure. If the value of log10 3.7 copies/ml (5000 copies/ml) is taken as the threshold of virological failure, as recently recommended by the 2009 revised WHO criteria, 18 the percentage of patients in virological failure would increase to 36% (n = 295), including 239 (81%) patients on a first-line regimen and 50 (19%) patients on a second-line or later line regimen. Therefore, the rates of virological failure were 32% (239/745) in patients on a first-line regimen and 68% (50/74) in patients on a second-line or later line regimen.
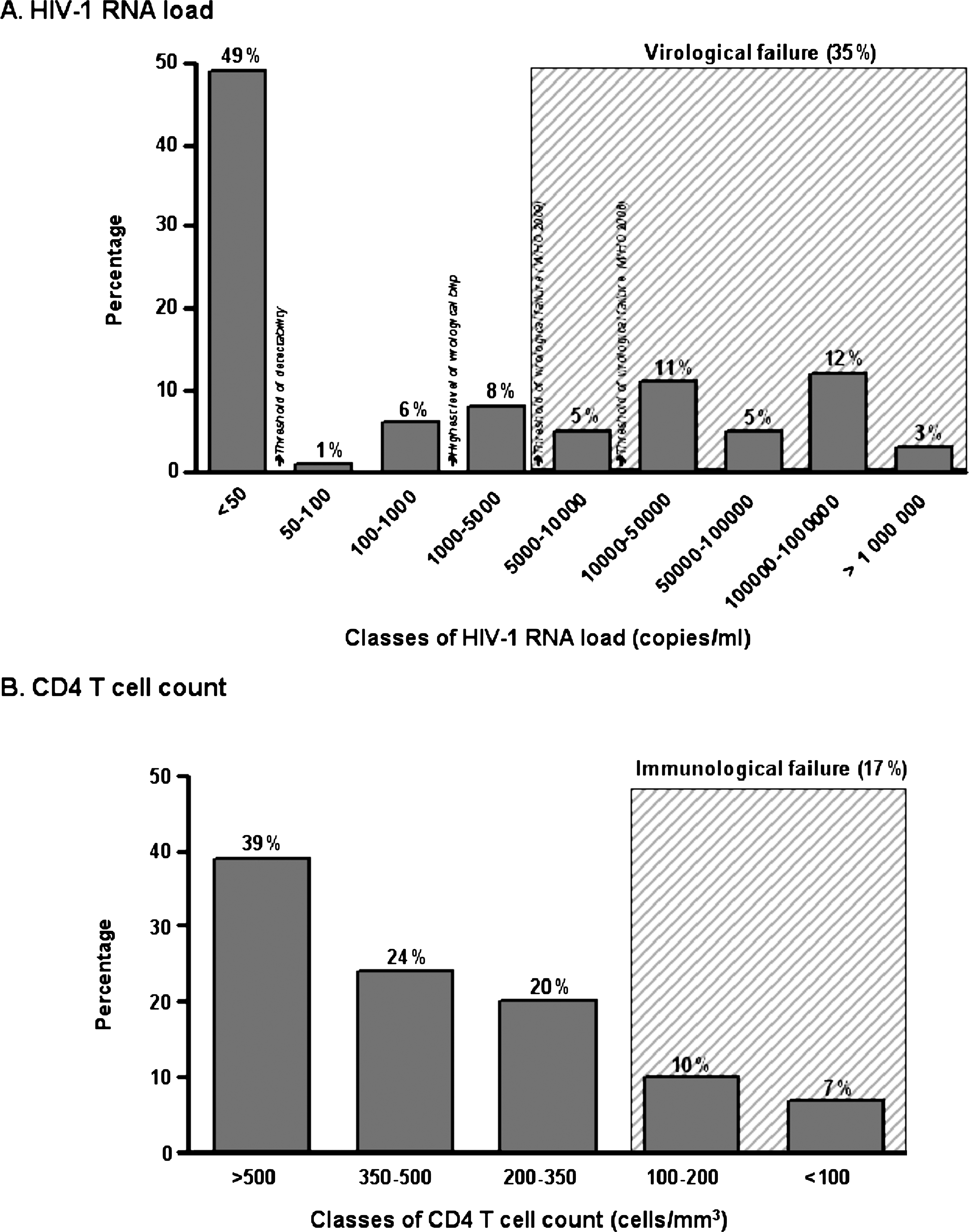
Distribution of HIV-1 RNA viral load
The distribution of CD4 T cell counts is depicted in Fig. 1B. Thirty-nine percent of patients displayed a CD4 T cell count above 500 cells/mm3, 24% of patients displayed a CD4 T cell count between 350 and 500 cells/mm3, 20% of patients displayed a CD4 T cell count between 200 and 350 cells/mm3, 10% of patients displayed a CD4 T cell count between 100 and 200 cells/mm3, and 7% of ARV-treated patients displayed severe immunodeficiency with a CD4 T cell count below 100 cells/mm3. Thus, 17% of patients had a CD4 T cell count below the threshold of ARV treatment initiation according to the 2006 WHO revised criteria for adults and adolescents (200 cells/mm3). 16 The number of treated patients with a CD4 T cell count under 350 cells/mm3, the new CD4 T cell threshold for treatment initiation, 18 reached 37%.
Antiretroviral drug resistance study: patients characteristics
A genotypic resistance test was carried out in 75 of 254 (30%) patients with virological and/or immunological failure. The period between the initiation of ARV-based therapy and the time of the genotypic resistance test was highly variable, ranging from 6 months to 5 years (median 3.1 years). The median age of the patients was 37 years. Thirty-five patients (47%) were female. At the time of genotypic resistance testing, the median HIV-1 RNA viral load and the median CD4 T cell count were log10 4.6 copies/ml (range 1.7–6.4) and 147 cells/mm3 (range 2–1146), respectively. We checked that the subgroup of patients taking advantage of genotype analysis showed median HIV-1 RNA viral load, CD4 T cell count, and treatment duration similar to the remaining 179 patients in virological and/or immunological failure not taking advantage of genotype analysis (data not shown).
The more frequently prescribed ARV regimen was the association of AZT, 3TC, and efavirenz (EFV) received by 32% of the patients (n = 24). The generic combination of stavudine (d4T)/lamivudine/nevirapine (NVP) was received by 19% (n = 14) of the patients. The combinations of d4T/3TC/EFV and AZT/3TC/NVP were received by nine and eight patients, respectively. Twenty patients (27%) received a PI-containing regimen, mainly with IDV (n = 14), but with LPV in six cases. Finally, 62 (83%) of the 75 selected patients for genotyping analysis were on first-line therapy, whereas the 13 remaining ones were on a second-line regimen.
The predominant subtype was CRF02_AG, detected in 31 patients (52%). A large variety of subtypes was observed: subtype A1 (n = 6; 10%), CRF11_cpx (n = 5, 8%), subtype F2 (n = 4, 7%), subtype D (n = 2, 3%), CRF01_AE (n = 1, 2%), CRF14_BG (n = 1, 2%), and F2/CRF02_AG recombinant form (n = 1, 2%) (Fig. 2). Finally, eight samples (14%) were unclassified HIV-1 subtypes.
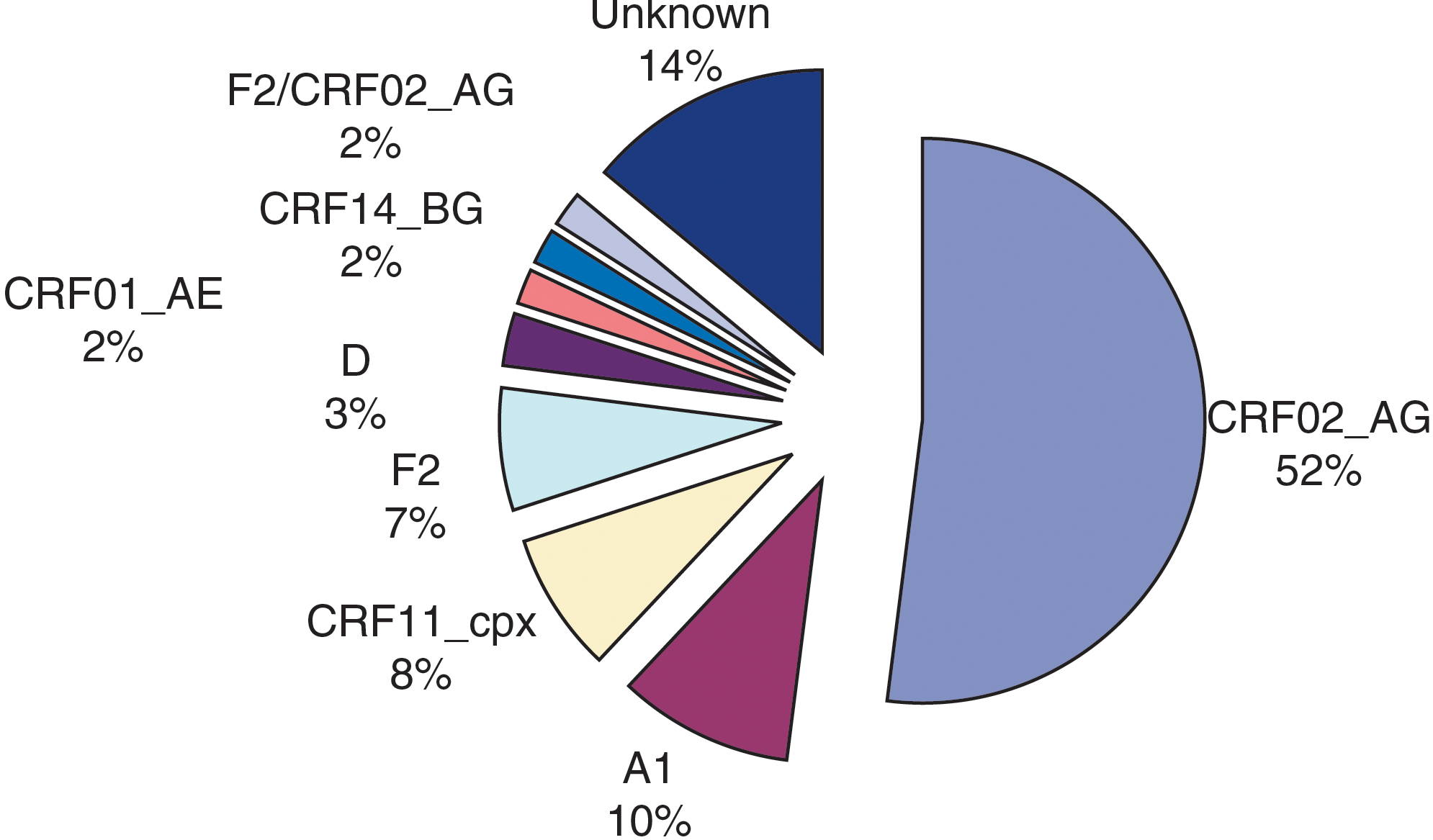
Distribution of HIV-1 subtypes among 75 HIV-infected patients followed up in Douala, Cameroon in virological and/or immunological failure and selected for genotype analysis. Color images available online at
Genotypic resistance testing data
Sequence results were successfully obtained in 59 samples (79%) for the RT gene and in 57 (76%) for the PR gene. Thirteen of 16 samples with negative amplification were from patients with an HIV-1 RNA viral load at a low level (between log10 2 copies/ml and log10 3 copies/ml).
Eighty percent (n = 47) of 59 patients whose genotypic analysis was successful displayed resistant virus to at least one ARV drug. In more than half of the patients harboring wild-type virus, ARV drug discontinuation for more than 1 month or poor adherence to ARV-based therapy was well documented. The adherence was assessed by a self-reporting questionnaire on ARV drugs intake, as previously described. 19
Resistance to at least one molecule of the NRTI drug class was found in virus from 80% of patients (n = 47). The most common resistance mutation was the M184V mutation harbored by 71% of the virus (42/59) (Fig. 3A). The thymidine analog mutations (TAMs) were observed at a high proportion, found in virus from 63% of patients. In most of cases, the observed TAMs were indicative of the TAM1 pathway (49%), associated with the T215Y mutation. 20 Noteworthy, multidrug-resistant (MDR) viruses were frequently detected: six samples with the Q151M mutation (10%) and two samples with an insertion at codon 69 of the RT gene (3%). The mutation L74I/V was detected in virus from 8% of patients. Only one patient displayed plasma virus harboring the K65R mutation.
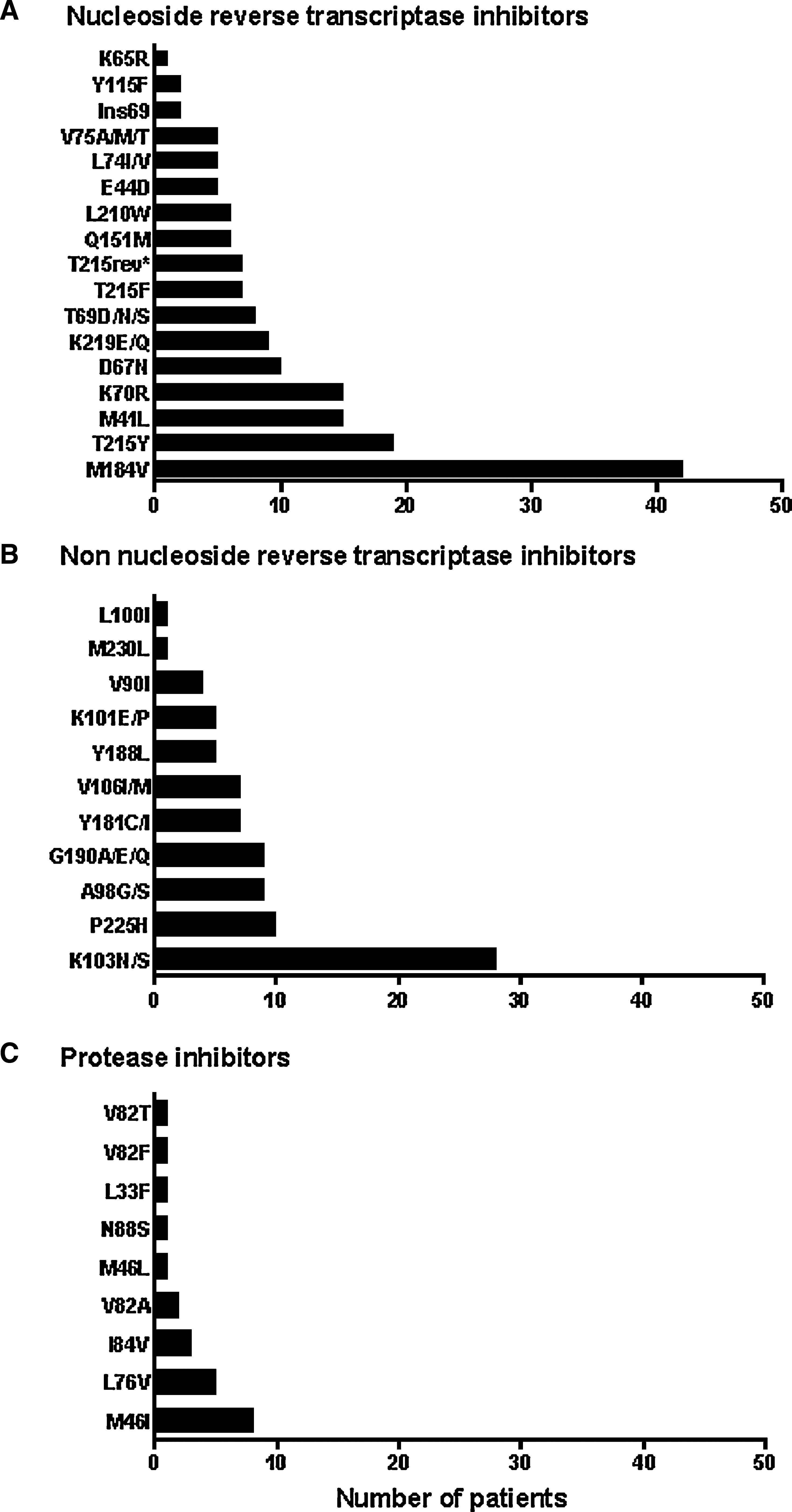
Number of patients whose viruses showed resistance-associated mutations to nucleoside reverse transcriptase inhibitors (NRTIs)
Resistance to the NNRTI drug class was found in viruses from 76% of patients (n = 45), with a median of two NNRTI resistance mutations per sample (range 0–4). The most prevalent NNRTI resistance mutation was the K103N/S mutation displayed by 46% of the virus (Fig. 3B). Of note, the mutation P225H was detected in virus from 17% of patients. The mutations V106I/M and Y181I/C were detected in seven cases (12%).
As expected with HIV-1 non-B subtypes protease sequences, a high frequency of natural polymorphisms was observed (median five, range three to seven). Resistance to at least one molecule of the PI drug class was found in virus from 19% of patients. The predominant major PI resistance mutation was the M46I/L mutation found in all PI-resistant viruses, since IDV was routinely used as the PI in the African context (Fig. 3C). Interestingly, the mutation L76V was found in nearly half (5/11, 45%) of PI-resistant virus, always associated with the M46I mutation, and represented the second most prevalent major PI resistance mutation with a high prevalence of 8.8% (Table 1). Only one patient whose virus harbored the L76V mutation had taken LPV for a period of 2 years; the four remaining patients had never received any LPV-containing regimen, only IDV-containing regimens.
Therapeutic history, current antiretroviral treatment, HIV-1 subtype, profiles of resistance-associated mutations to nucleoside reverse transcriptase inhibitors (NRTIs), nonnucleoside reverse transcriptase inhibitors (NNRTIs), or protease inhibitors (PIs), interpretation of genotypic resistance profiles according to the 2009 ANRS algorithm, and in vitro phenotype resistance are given.
Phenotyping of virus from patient #D5 was unsuccessful.
na, not applicable; nd, not determined; WT, wild-type; yr, year. 3TC, lamivudine; ABC, abacavir; APV, amprenavir; ATZ, atazanavir; AZT, zidovudine; d4T, stavudine; ddI, didanosine; DRV, darunavir; EFV, efavirenz; ETV, etravirine; IDV, indinavir, LPV, lopinavir; NFV, nelfinavir; NVP, nevirapine; SQV, saquinavir; TDF, tenofovir; TPV, tipranavir.
Resistance mutations are identified according to the Agence Nationale de Recherches sur le SIDA et les hépatites virales (ANRS) algorithm, version 18, July 2009. Major resistance mutations to protease inhibitors according to the IAS-USA list are indicated in bold.
Genotypic susceptibility interpreted using the ANRS algorithm: RP, possible resistance; S, susceptible; R, resistant.
Phenotypic susceptibility expressed as the fold change (FC) of inhibitory concentration 50% (IC50) values. FC values interpreted as resistant are indicated in bold; FC values interpreted as an intermediate level of resistance are indicated in italics.
Overall, 4 (7%) of 47 patients in therapeutic failure with successful genotypic data harbored resistant virus to one drug of their ongoing ARV-based therapy, 17 (29%) exhibited resistant virus to two drugs of their current therapy, and 24 (40%) harbored plasma virus resistant to all three drugs of their ARV-based therapy.
Phenotypic analysis of HIV-1 variants harboring the L76V mutation
The unexpected high prevalence of the L76V mutation found in virus showing PI resistance mutations (45%) prompted us to evaluate their phenotypic resistance profiles to ARV drugs, as given in Table 1, in four patients whose virus phenotype assay was successful. The four tested viruses displayed a high level of resistance to IDV with an FC ranging from 7.8 to 33.3. Two of the viruses showed a high level of resistance (FC > 18) to LPV and the two remaining viruses displayed an intermediate level of LPV resistance (FC = 8). Three viruses were susceptible to darunavir and one exhibited an intermediate level of resistance to this drug. Regarding susceptibility to atazanavir, two viruses were found resistant and two others were susceptible. Of note, in vitro hypersusceptibility to tipranavir was observed in three out of four viruses.
Viral susceptibility to future therapeutic options
We further estimated the possible ARV therapeutic options remaining in patients under virological failure, according to their resistance genotypes. Genotypic resistance tests in the 59 patients of the study showed that they harbored plasma virus remaining susceptible to a median of three molecules of the NRTI drug class, of one molecule of the NNRTI drug class (which was exclusively etravirine), and to all of the PI class.
Five patients (8%) displayed multiresistant viruses to all of the six current NRTIs. In nine patients, plasma viruses were found to be susceptible to only one NRTI drug: didanosine (ddI) or tenofovir (TDF). Among the NRTI-resistant viruses, 76% remained susceptible to ddI and 74% to TDF, the two main ARV drugs included in the second-line regimen in Africa.
The majority of patients displayed viruses remaining susceptible to the second NNRTI generation etravirine, since only one (1.7%) harbored virus with a predicted resistance to this drug.
Only 4 of the 11 PI-resistant viruses (36%) showed a remaining susceptibility to LPV, which constitutes the major PI of the second-line regimen in Africa. In addition, we assessed the molecules remaining susceptible in the case of the L76V-mutated virus by combining genotypic and phenotypic results. Among the four available samples, the following ARV drugs, TDF, etravirine, and darunavir, remained susceptible in three, four, and four patients, respectively; ddI and amprenavir remained susceptible in two patients and atazanavir in one patient.
Among the 46 patients on a first-line regimen with available genotypic resistance data, 34 (74%), 37 (80%), 44(96%), and 45 (98%) exhibited viruses susceptible to abacavir, tenofovir, atazanavir, and lopinavir, respectively, and at least 37 (80%) could receive a second-line regimen with at least two active ARV drugs according to the 2009 revised WHO recommendations. Among the 13 patients on a second-line regimen with available genotypic resistance data, 10 (77%), 9 (69%), 9 (69%), and 8 (61%) exhibited virus susceptible to abacavir, tenofovir, atazanavir, and lopinavir, respectively.
Virus polymorphisms and genotypic resistance mutations
Resistance mutations evidenced in the present series were not associated with specific HIV-1 subtypes, despite high genetic diversity. Thus, seven protease sequences (12%) issued from PI-naive patients infected by CRF02_AG, F2, D, and CRF11_cpx subtypes displayed possible or full resistance to saquinavir (SQV), related to the presence of natural polymorphisms at codons 10, 15, 20, and 62 of the PR gene according to the ANRS algorithm. No significant differences in the frequency of drug resistance mutations between the CRF02_AG subtype and the others HIV-1 subtypes of the study viruses could be observed (data not shown). Of note, the NNRTI resistance mutation P225H was found in eight patients with the CRF02_AG subtype and in two with other HIV-1 subtypes. The major PI resistance L76V mutation was found in both CRF02_AG and in other HIV-1 subtypes.
Discussion
In the present study, the efficiency of ARV treatment, mostly as a first-line regimen prescribed according to WHO guidelines, was evaluated in 819 HIV-infected patients followed up in healthcare centers of the private sector in Douala, the economic capital of Cameroon. Overall, 36% of ARV-treated patients were in virological failure, as assessed by a plasma viral load above log10 3.7 copies/ml under treatment for more than 6 months. According to immunological status, 17% of patients showed a CD4 T cell count under 200 cells/mm3 and 37% showed a count under 350 cells/mm3, indicating either ongoing immunorestoration or immunological failure under treatment.
Genotypic resistance tests, carried out in the subgroup of 75 selected patients representative of the 254 patients in virological and/or immunological failure, showed that 80% of patients displayed virus resistant to at least to one ARV drug, most frequently of the NRTI class (80%), followed by the NNRTI class (76%) and the PI class (19%), thus reflecting the therapeutic use of ARV drugs in Cameroon as recommended by the WHO. The pattern of genotypic resistance mutations was not associated with viral diversity. Further therapeutic options in patients in therapeutic failure with resistant viruses included a median of three molecules of the NRTI drug class, one molecule of the NNRTI drug class (which was exclusively etravirine), and all of the PI class.
Although in the majority of the patients, the second-line regimen proposed by the 2009 revised WHO recommendations could be effective, a minority showed a complex resistance genotypic profile highly predictive of resistance to the usual WHO second-line regimen. Thus, the analysis of genotypic resistance mutations appeared markedly relevant, even necessary, in some patients in virological failure. However, the therapeutic options resulting from the determination of resistance mutations frequently included ARV drugs not frequently available in Cameroon. Taken together, these observations indicate that virological failure may be frequently encountered in patients cared for in the private sector of Douala, emphasizing the importance of performing regular plasma viral load measurements and the need for genotypic analysis of ARV resistance in a minority of patients in therapeutic failure not responding to a second-line ARV regimen as proposed by the WHO guidelines.
Overall, 36% of ARV-treated patients under treatment for more than 6 months displayed virological failure, as assessed by a plasma viral load above log10 3.7 copies/ml. Notably, the rate of virological failure was 2-fold higher in patients on a first-line regimen than in patients on a second-line or later line regimen, strongly arguing for the urgent need for better second-line therapeutic strategies. Based on immunological status, 17% of patients showed a CD4 T cell count under 200 cells/mm3 and 37% showed a CD4 T cell count under 350 cells/mm3, indicating either ongoing immunorestoration or immunological failure under treatment. Virological failure associated with ARV drug resistance has been frequently observed in treated patients in Cameroon, at variable rates according to duration of treatment, healthcare services, and urban or remote areas. 3,9,11,21
Our observations showed seemingly high rates of both virological failure (36%) and resistant viruses (around 80%) in cases of detectable viral load under treatment. These features contrast with the relatively low prevalence of resistant viruses under ARV treatment, previously reported by Kouanfack and colleagues in the Central Hospital of Yaoundé. 11 The differences between the rates of virological failure and resistant viruses observed in patients followed in Yaoundé and those in Douala may be due in part to the high level of healthcare services offered in the so-called “hôpital de jour” of the Central Hospital of Yaoundé, which is basically a university and research center for HIV-infected patients. Interestingly, 20% of Douala patients in virological failure showed sensitive viruses, suggesting a problem with adherence that must be corrected. Numerous socioeconomical factors, including the heterogeneity of healthcare services in the private sector, which includes medical services of very different levels, and the occasional difficulties with the distribution of ARV drugs and with payment for routine biological tests for treatment monitoring, may partly explain the relative high prevalence of virological failure observed in the study patients. Taken together, these findings strongly emphasize the need to reinforce the healthcare of patients treated in the private sector of Douala to achieve the level of university healthcare structures.
Eighty percent of patients in virological failure displayed plasma virus resistant to at least one ARV drug. Such a high prevalence was not surprising, since ARV drugs with a low genetic barrier to resistance were widely used, such as lamivudine or NNRTIs, which was found to be similar to previously reported data in HIV-treated patients with virological failure. 12,14 As expected, the prevalence of drug resistance was correlated with the differential use of ARV drug classes: 80% NRTIs, 76% NNRTIs, and 19% PIs, thus reflecting the therapeutic use of ARV drugs in Cameroon as recommended by the WHO.
Forty percent of patients exhibited plasma virus resistant to all three drugs of their ongoing ARV-based therapy, a high proportion compared to previous data reporting less than 10% of triple-drug-resistant virus in ARV-treated patients displaying virological failure. 12,13 This outcome is likely to be related to a long period of detectable HIV-1 viral load under ARV-based therapy, 22 which commonly occurred in Africa. This was due to a lack of viral load control, which led to a delayed diagnosis of virological failure, with a risk for an accumulation of drug resistance mutations and reduced future therapeutic options. 23
Another finding we observed in our study is an unexpected high prevalence (8.8%) of the major PI resistance mutation, L76V; in comparison, previous studies reported a proportion of 1.1% in the Stanford HIV Drug Resistance database 24 and of 2.7% in a set of subtype B virus. 25 In the latter, 70% of patients exhibiting L76V-resistant variants were receiving LPV. Others also described this mutation, but in the specific context of therapeutic failure under LPV monotherapy in ARV-naive patients. 26,27 In the study by Delaugerre et al., the L76V mutation was found at a frequency of 3.6% (3/83 patients); interestingly, all three patients were infected with the CRF02_AG subtype. 24 In our study, the selection of the L76V mutation was not found to be associated with a specific HIV-1 subtype. Among the five patients harboring L76V-resistant variants in our study, four were receiving IDV and one LPV; in all cases a high level of viral replication under drug pressure was observed for a long time, more than 2 years, with poor adherence. Similar to the previous findings, 23 –25 we observed in all cases that the L76V mutation was accompanied by the M46I mutation. Noteworthy, the L76V mutation is involved not only in LPV resistance, but likely also in resistance pathways for fosamprenavir and darunavir, 26,27 dramatically reducing future therapeutic options in the PI drug class, especially in Africa.
A majority of patients (52%) in the present study were infected with a CRF02_AG subtype. No significant differences in the frequency of ARV drug resistance mutations between the CRF02_AG subtype and others subtypes were observed, such as recently described between the CRF02_AG and CRF06_cpx subtypes. 13 However, we discovered that the presence of HIV-1 non-B subtype polymorphisms had an impact on genotypic resistance test interpretation, since 12% of protease sequences from PI-naive patients were believed to have a full or intermediate level of resistance to SQV, as we previously described with the CRF12_BG subtype in HIV-infected adults 12 and the CRF11_cpx subtype in HIV-infected children. 28
The second-line regimens proposed by the 2009 revised WHO recommendations could be effective in the majority of patients in virological failure with resistant viruses. However, when looking at the remaining therapeutic options in our study for the NRTI drug class, we observed that TDF was still active in 74% of cases, despite a highly proportion of TAMs (63%), and ddI was still active in 76% of cases. For the NNRTI drug class, the only active drug was the second-generation NNRTI molecule etravirine, which is not yet available in Cameroon. The majority of viruses displayed sensitivity to all molecules of the PI drug class, since it was the lass less used. However, PI genotypic resistance profiles detected in the present study with five patients harboring virus with the L76V mutation, an LPV resistance-associated mutation, 26 strongly impaired future therapeutic options. Thus, LPV, the main PI present in the second-line regimen, remained active in only 36% of the described PI-resistant virus. Overall, future therapeutic options appeared limited in less than 25% of patients of our series, taking into account the fact that recent ARV drugs such as etravirine or darunavir are not yet commonly available. A recent study assessing options for a second-line ARV regimen following an initial regimen of a fixed dose combination of stavudine/lamivudine/nevirapine reported limited therapeutic options in 48% of patients. 29 Interestingly, a minority of ARV-experienced patients showed complex resistance genotypic profiles, largely predictive of resistance to the usual WHO second-line regimens, which may be resolved only with genotypic resistance tests. 30,31
In conclusion, these data confirmed and emphasized the need for (1) improving biological monitoring to diagnose virological failure early with the aim of preserving future therapeutic options and (2) increasing data from HIV-1 non-B subtypes to achieve a better understanding of resistance profiles. To our knowledge, such a prevalence of the L76V mutation was not previously reported in non-B subtypes. Finally, further investigations are needed to obtain more reliable algorithm interpretations for genotypic resistance tests adapted to non-B HIV-1 subtypes.
Footnotes
Acknowledgments
We are very grateful to André Capt and Dr. Lee Bacheler (Virco BVBA, Mechelen, Belgium) for their assistance in performing the phenotypic assays.
Author Disclosure Statement
No competing financial interests exist.