
Abstract
The determination of the prevalence of primary resistance to antiretroviral therapy in different places of the world is of extreme importance in molecular epidemiology monitoring, and it can guide the initial patient therapy in a given geographical area. The frequency of drug resistance mutations (DRM) and the genetic variability of HIV-1 isolates from newly diagnosed HIV-infected pregnant women attending the antenatal clinics of the Lucrecia Paim and Augusto N'Gangula maternities, Luanda-Angola, were determined. Thirty five out of 57 samples (61.4%) were sequenced and one mutation associated with resistance to nucleoside reverse transcriptase inhibitors was detected. Additionally, two mutations associated with resistance to non-nucleoside reverse transcriptase inhibitors were also detected. No primary mutations associated with protease inhibitors (PI) were found. Subtypes A1, C, D, F1, G, H, CRF 13, CRF 37, and other mosaics were detected.
S
By the end of 2007, Sub-Saharan Africa (SSA) was the most affected region of the world by HIV-1, the virus that causes the Acquired Immunodeficiency Syndrome (AIDS), with a total of approximately 22.5 million people infected and more than three-quarters of the world deaths associated with AIDS. 2
In 1985, the first case of AIDS was diagnosed in Angola, a country located in SSA and with 17 million inhabitants. Up to December 2007, approximately 190,000 Angolans were infected by HIV, representing a total prevalence of 2.1%, based on antenatal HIV surveillance studies performed in the country, from the total 110.000 were women and 17.000 were children under 15 years. 1 –3
Access to antiretroviral therapy (ART) has increased dramatically in limited resource settings countries, where the majority of people infected with HIV and necessitating treatment resides. 1 In Angola, universal access to antiretroviral therapy started in 2004 and approximately 11,240 infected people had access to treatment until 2009. 4 Gaining access to antiretroviral drugs had a substantial impact in the HIV–AIDS epidemic in the country, in addition to improving the quality of life for people living with HIV/AIDS. Nevertheless secondary resistance has emerged in patients failing ARV therapy in Luanda. 5
Treatment in Angola includes a combination of two nucleoside reverse transcriptase inhibitors (NRTI), zidovudine (AZT) and lamivudine (3TC), and a non-nucleoside reverse transcriptase inhibitor (NNRTI) efavirenz (EFV) or nevirapine (NVP) 3,4
The Mother to Child Transmission (MTCT) is the most important source of HIV infection in children under 15 years. This affects approximately 500,000 children per year worldwide and is responsible for 1800 new infections in children daily, in most developing countries. The rate of vertical transmission in treatment naïve women are 15–25% in developed countries and 25–45% in developing countries. 6 The program for the prevention of vertical transmission (PTV) in Angola started in 2004, aiming to provide integral support to all HIV positive pregnant women as well as to the new born. 7 Under this program, the introduction of the short course ARV therapy has caused the transmission rate to drop to 2% level. 6
The increasing prevalence of resistance to antiretroviral drugs among patients infected with HIV-1 has been associated with increased transmission of resistant virus to newly infected individuals. Therefore, the effectiveness of the antiretroviral may be limited by transmission of resistant virus strains. 8 The rate by which the transmitted mutation associated with resistance reverts to the wild-type has not been fully outlined. However, mutations present at the time of transmission of HIV are more stable than those selected under pressure from antiretroviral drugs. 9 Until now, studies on HIV mutations associated with ARV resistance in pregnant women in Africa are limited and currently unknown in Angola. Due to its public health relevance, we have embarked on the investigation of mutations associated with antiretroviral drugs in the PR and RT genes of HIV-1 in treatment-naïve pregnant women.
A total of 57 treatment-naïve pregnant women on prenatal consultation were diagnosed with HIV-1 infection from November 2008 to January 2009, in two reference maternities Lucrécia Paim and Augusto N'Gangula, located in Luanda, capital of Angola. All pregnant women underwent pre- and post-test counseling and provided written consent prior to participating in the study. The inclusion criteria were: (a) women recently diagnosed with HIV-1, (b) were enrolled at the PTV antenatal clinic, (c) had not taken antiretroviral drugs previously, and (d) were more than 18 years old at the time of the study.
Blood samples, demographic, clinical, and epidemiological information were assessed during the period of the collection. Plasma was aliquot and stored at −80°C immediately after separation.
HIV-1 diagnosis was performed based on the Angolan National Algorithm using two rapid tests for detection of antibodies against HIV-1/2. HIV antibodies tests were performed in the maternities using the following rapid tests: Determine® (Abbott Laboratories, Abbott Park, IL) and Unigold® (Trinity Biotech, Bray, Ireland). Discordant results were further tested by an ELISA assay (Vironostika HIV Uni-form II Ag/Ab ELISA test; bioMérieux, France).
CD4+ lymphocyte count was carried out on the Becton Dickinson (Franklin Lakes, NJ) FACS Count and viral load determined by using 1ml of plasma, on the NucliSens HIV QT platform.
HIV-positive samples were sent to the Central Public Health Laboratory of the State of Pernambuco, Brazil for sequence of PR and RT genes. RNA extraction was performed using QIAamp viral nucleic acid extraction kit under conditions recommended by the manufacturer (Qiagen, Valencia, CA). The RT-PCR and PCR reactions were performed using a one step RT-PCR TruGene kit (Siemens Diagnostics, New York City, NY) to obtain an amplified product from HIV-1 pol gene. Nucleotides: 10 to 297 of protease and 112 to 741 of reverse transcriptase were analyzed.
The presence of drug-resistant mutations was analyzed according to the Calibrated Population Resistance Tool (CPR) Version 4.1 beta that uses the Surveillance Drug Resistance Mutation panel 2009.
10
The genetic subtype was determined by phylogenetic analysis in MEGA v.3.1 software and with REGA HIV-1 Automated Subtyping Tool
11,12
(
This study was approved by the Ethics Committee of Angola, Ethics Committee of Human Research of the Institute of Integrated Medicine Prof. Fernando Figueira and by the National Commission on Ethics in Research of the Brazilian Ministry of Health (CONEP 519/2009).
A total of 57 samples were collected and 35 (61.4%) were successfully sequenced for the HIV-1 pol gene sequences generated. We failed to amplify the remaining 22 samples, due to low viral load (<1000 copies/ml). Table 1 summarizes demographic and epidemiological characteristics of the 57 individuals studied. The median age was 28 years (range 18–39 years), CD4+ lymphocytes count had a median of 285 cells/mm3 (range 31–1269 cells/mm3), suggesting that the majority of the individuals studied were at the late stage of disease.
The subjects were included in a study for the prevalence of primary and secondary mutations associated with antiretroviral drug resistance conducted from November 2008 to January 2009 in Luanda-Angola.
HIV-1 pol sequences (n = 35) were analyzed and we found 31 specimens showing homogeneous subtype for both PR and RT regions. Subtype F1 was the most prevalent accounting for 22.8% of all sequences, followed by subtypes C (17.1%), A1 (14.2%), D (8.5%), AG (8.5%), G (8.5%), H (5.7%), and BD (2.8%). More complex profiles were found in four samples: 1 CRF 13_cpx, 1 CRF 37_cpx, 1 Unclassified/H and 1 Unclassified. Distribution of HIV-1 subtypes in the two regions of 34 specimens is depicted in the phylogenetic tree shown in Figure 1. GenBank accession numbers from 35 sequences are HM357723 to HM357757. None of the known primary mutations associated with PI resistance was detected among PR sequences. However, secondary mutations, not related to drug resistance, were found at positions T74S (2.8%), L10V (25.7%), and L10I (14.2%). Overall we found two isolates carrying primary mutation in RT sequence (5.7%). Sample#11 showed DRM to NRTI and NNRTI (M184V and G190A), and sample # 37 solely shown DRM related to NNRTI (G190A).
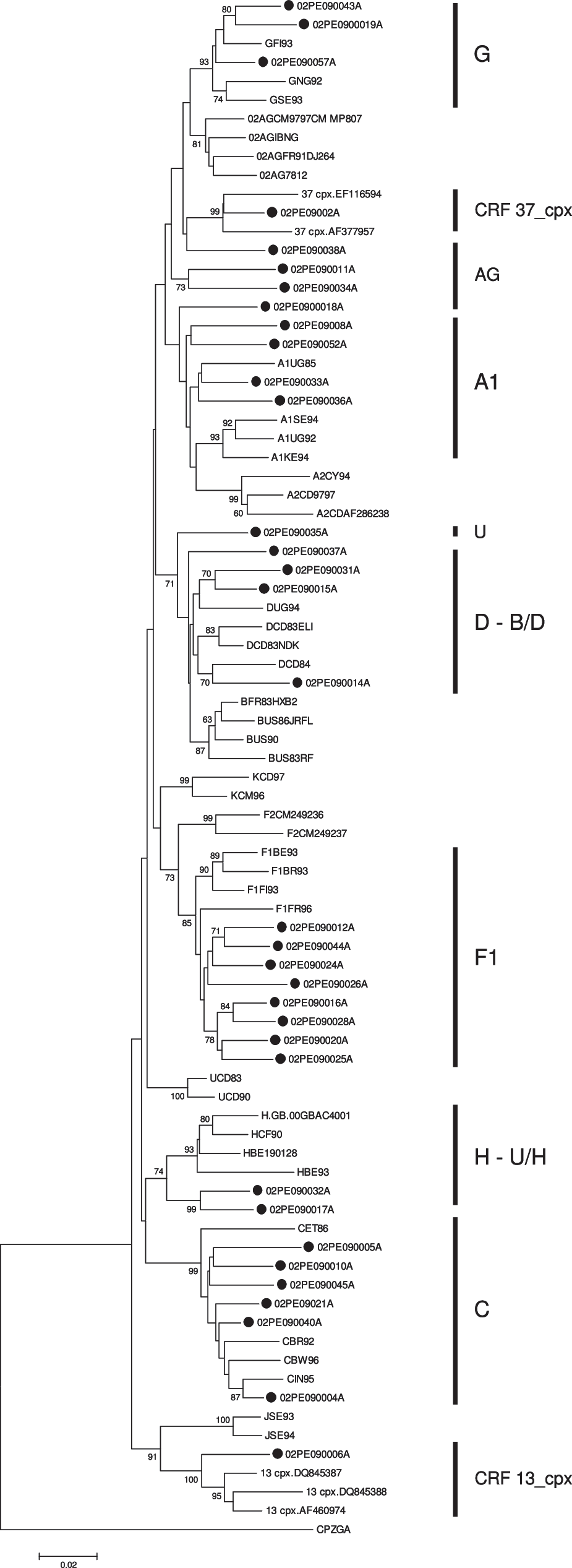
Phylogenetic analysis of HIV pol sequences (Protease 10–297 and RT 112–741 nucleotides) from HIV-1 infected pregnant women in Luanda-Angola. Sequences were aligned in BioEdit software and tree constructed by Neighbor-Joining method using Kimura's 2-parameter in MEGA v.3.1.
The median age of the pregnant women was 28 years and the median of the gestational age were 20 weeks in the occasion of HIV test. Data addressing the prevalence of primary mutations associated with antiretroviral resistance treatment-naïve individuals infected with HIV-1 in Sub-Saharan Africa (SSA) are limited. This study provides the first report of primary mutations associated with antiretroviral resistance among antiretroviral treatment-naïve pregnant women in Angola. In accordance with other reports from SSA, a low prevalence of primary mutations associated with antiretroviral resistance was found among treatment-naïve pregnant women in Luanda. In our study, we identified two samples carrying DRM. Sample#11 carries mutation to two drug classes (NRTI and NNRTI) and sample #37 showed only mutations to NNRTI (Table 2).
PR-Protease, RT-Reverse Transcriptase, U-Unclassified.
Nucleotides: Protease (10–297), Reverse Transcriptase (112–741).
The study was in accordance with Stanford University HIV-1 Drug Resistance Database.
Mutation M184V causes high-level in vitro resistance to lamivudina (3TC) and emtricitabine (FTC) and low level in vitro resistance to didanosine (DDI) and abacavir (ABC). However, it increases susceptibility to zidovudine (AZT), tenofovir (TDF), and stavudine (D4T). Two secondary mutations (T69S and V118I) associated with NRTI resistance have been also found. The T69S which affect NRTI susceptibility is not well studied and V118I occurs in ∼2% of untreated persons, and in higher frequency in persons receiving multiple NRTIs. V118I causes low-level resistance to 3TC and to other NRTIs when associated with E44A/D and/or one or more thymidine analog-associated mutations (TAMs). One primary mutation associated with NNRTI resistance (G190A) was detected. This substitution causes high-level resistance to NVP, intermediate resistance to EFV, and increased DLV susceptibility. Only one secondary mutation associated with NNRTI resistance was found, the amino acid substitution K238T, which is usually selected in combination with K103N causes high-level resistance to NVP, EFV, and DLV.
No primary mutations associated with PI resistance were detected in this study, and three secondary mutations associated with PI resistance were present in 14 specimens. They were probably polymorphisms associated with non-B subtypes circulating in Angola. Indeed, T74S which is associated with reduced NFV susceptibility, occurs in untreated persons with subtype C viruses, and L10I/V is associated with resistance to most PIs when presented with other mutations. This polymorphism occurs in 5–10% of untreated persons as reported in this study. In fact, the overall low prevalence of primary mutations associated with antiretroviral resistance in Luanda reflects the limited use of antiretroviral drugs in this region to date.
The subtype profile of HIV-1 isolates in Angola is very heterogeneous and eight different subtypes have been reported circulating in Luanda. 6,13 –16 Our data confirm and extend these findings as we have additionally detected the rare H and CRFs 13–37 complex profiles in some samples. Some strains from Angola have little organized substructure and form weaker clusters within the phylogenetic tree, not allowing a clear clustering of some sequences, as well as the subtype assessment. The majority of strains analyzed clustered with prototypic subtype F1. Of note, this variant is the major pure non-B or is part of the CRFs/mosaic sequences variants circulating in Brazil and Latin America. It was recently reported that subtype F1 in Angola seems to be the result of a single founder event. Subtype F1 sequences from Angola are closely related to those described in Romania, and distantly related to the subtype F1 lineage circulating in South America. The original diversification of subtype F probably occurred within the Democratic Republic of the Congo (DRC) in the late 1950s. 12 The high genetic diversity of HIV-1 found in Angola suggests that HIV-1 has been circulating in Angola for a long time, and suggests also that there is intense population mobility between Angola and DRC.
Footnotes
Acknowledgments
We thank Dr. Orlando Costa Ferreira Jr. for kindly revising this manuscript.
Author Disclosure Statement
No competing financial interests exist.