
Abstract
We compared the efficacy of combination antiretroviral therapy (cART) of Antillean HIV-1-infected patients treated on the Caribbean island of Curaçao (CUR-AN) with Antillean (NL-AN), Surinam (NL-SUR), and Dutch (NL-NL) patients treated in The Netherlands. In total 2118 therapy-naive patients who started cART between January 2005 and August 2008 were included in the comparison. The CUR-AN patients initiated cART at a median CD4 cell count of 141 cells/mm3 and 63% had counts below 200 cells/mm3. Within 12 months of the start of cART 76% of the CUR-AN patients achieved viral suppression, defined as HIV-1 RNA plasma levels below 80 copies/ml. The percentage achieving viral suppression was higher in patients treated in The Netherlands (NL-AN = 87%, NL-SUR = 93%, and NL-NL = 96%). Lost to follow-up after 30 months of cART was 10% among CUR-AN patients and was higher than observed among patients treated in The Netherlands (NL-AN = 8%, NL-SUR = 3%, and NL-NL = 2%). A similar pattern was found for progression to AIDS and death (10% of CUR-AN vs. 5%, 6%, and 7% of NL-AN, NL-SUR, and NL-NL patients, respectively). Late start of cART and limited viral suppression after the start of cART determine the higher rate of disease progression to AIDS and death among Antillean patients treated in Curaçao. The high percentage of lost to follow-up may result in an underestimation of AIDS and AIDS-related death among HIV-1-infected Antilleans treated in Curaçao.
Introduction
T
Curaçao is a Caribbean island and part of The Netherlands Antilles. It has approximately 140,000 inhabitants and an estimated HIV prevalence of 0.61–1.05%. 11 A relatively large number of Antilleans (135,000) live in The Netherlands. In Curaçao antiretroviral therapy has been available since 1996. Centralized registration and monitoring of HIV-infected individuals treated in Curaçao began in January 2005, in collaboration with the Dutch HIV Monitoring Foundation [Stichting HIV Monitoring (SHM)]. 12
We evaluated the immunological, virological, and clinical responses to cART in HIV-1-infected Antillean patients who started treatment for HIV-1 infection in Curaçao between January 2005 and August 2008 and then compared these responses with those of Antillean, Surinam, and Dutch patients who were treated in The Netherlands.
Materials and Methods
Study settings
Care of HIV-infected patients is provided in Curaçao at the St Elizabeth Hospital in Willemstad. Antiretroviral drugs are distributed by the hospital pharmacy and include the nonnucleoside reverse transcriptase inhibitors (NNRTIs) efavirenz and nevirapine, the nucleot(s)ide reverse transcriptase inhibitors (NRTIs) tenofovir, didanosine, emtricitabine, stavudine, lamivudine, and zidovudine, and the protease inhibitors (PIs) indinavir, ritonavir, nelfinavir, saquinavir, and ritonavir-boosted lopinavir.
In The Netherlands, HIV care and treatment are provided by 8 university and 17 general hospitals throughout the country that are appointed by the Dutch Ministry of Health, Welfare and Sport as HIV treatment centers. 13 The full range of antiretroviral drugs is available for combination treatment.
Study population
The study population consisted of HIV-1-infected patients aged 15 years or older who were previously antiretroviral drug naive and who started cART between 1 January 2005 and 1 August 2008 in Curaçao or The Netherlands. We compared four subgroups: patients originating from The Netherlands Antilles were treated for HIV-1 in (1) Curaçao (CUR-AN) or (2) The Netherlands (NL-AN) and patients originating from (3) Surinam and treated in The Netherlands (NL-SUR) and (4) from The Netherlands and treated in The Netherlands (NL-NL). cART was defined as at least two NRTIs combined with at least one PI, one NNRTI, or both, or at least three NRTIs including abacavir or tenofovir.
Data collection
Demographic, epidemiological, clinical, virological, immunological, and therapy-related data were collected from patients' medical files after each (out-patient) hospital visit and were entered online into the SHM database by trained data collection clerks.
13
We scanned protease and reverse transcriptase (RT) sequences obtained during routine clinical care for major resistance-associated mutations to assess resistance to antiretroviral drugs (
Outcomes and statistical analysis
Clinical response was assessed by the combined endpoint of death or AIDS. Patients who did not attend the clinic and for whom no CD4 cell count and plasma viral load were available for more than 1 year beyond the date of their last visit, last viral load, or last CD4 cell count were classified as being lost to follow-up. A change in the composition of the first-line regimen was chosen as a measure of durability of the first-line therapy.
Time to clinical progression, lost to follow-up, and change in the first-line regimen were analyzed by Kaplan–Meier estimates and unadjusted and adjusted Cox proportional hazard regression models. Patients not known to have died by July 2009 were right censored on the date of their last visit prior to July 2009.
Because HIV-1 RNA concentration in plasma obtained from patients treated in Curaçao was measured by the commercially available NucliSens EasyQ (bioMérieux, Boxtel, The Netherlands) assay, we defined the virological response to cART as a concentration ≤80 copies/ml and calculated the percentage of patients with such a response 6, 12, and 18 months after the start of cART. Furthermore, we analyzed the time from the start of cART to the first of two consecutive viral load measurements ≤80 copies/ml. We observed differences in the frequency of HIV-1 RNA measurement between patients treated in Curaçao and The Netherlands, and because measurement frequency may affect parameter estimates, 14 we used a parametric survival model with a Weibull distribution, taking into account the interval-censored nature of the data.
T-lymphocyte subsets were measured with standard flow cytometry (FACSCalibur, BD Bioscience, The Netherlands). The median CD4 cell counts at the start of cART and at 6, 12, and 18 months were calculated. Differences at these time points among the four groups were assessed with the Mann–Whitney test. Changes in the immunological response up to 18 months after starting cART were analyzed by use of mixed effect models. For each patient a random slope between 0 and 6 months and between 6 and 18 months was assumed. We checked whether the results of the longitudinal mixed effect models were confirmed by the results from a Cox regression analysis of the time between the start of cART to the observation of an increase in CD4 cell count of at least 100 CD4 cells/mm3. Finally, we examined whether differences between groups in the rate of patients lost to follow-up could have affected the results of the CD4 cell count and viral load analysis by censoring at the end of the study period instead of the moment of lost to follow-up.
Adjusted models included the following potential confounders: gender, age at the start of cART, initial cART regimen, transmission risk group, plasma HIV-1 RNA concentration and CD4 cell count at the start, AIDS diagnosis at the start (any AIDS-defining event up to 1 month after starting cART), cART started during a pregnancy, weight at the start, and hepatitis B (HBV) or C (HCV) virus infection. HBV was defined as a positive result on a hepatitis B surface antigen (HBsAg) test. HCV coinfection was defined by a positive result on a qualitative or quantitative RNA test result, or if not available, a positive antibody test. Analyses were performed with SAS version 9.1 (SAS Institute, Cary, NC).
Results
A total of 2118 patients were eligible for analysis, including 123 patients in the CUR-AN group, 83 in NL-AN, 168 in NL-SUR, and 1744 in NL-NL (Table 1). Compared to the CUR-AN, NL-AN, and NL-SUR patients, we observed a lower proportion of women among the NL-NL patients. The median age at the start of cART was 43 years (IQR, 37–50) in the NL-NL and 44 years (IQR, 36–52) in the CUR-AN patients, which was higher compared to the median age in the NL-AN and NL-SUR patients [37 years (IQR, 31–42) and 39 years (IQR, 31–46)]. Of all 894 patients in whom the HIV subtype was determined, 100% of the CUR-AN patients were infected with subtype B, as were 90% of the NL-NL (compared to CUR-AN, p = 0.10), 84% of the NL-AN (p = 0.05), and 97% of the NL-SUR patients (p = 0.99). In Curaçao, HIV-1 diagnosis is often established in settings other than the one in which patients ultimately receive clinical care and CD4 cell counts at the moment of diagnosis are generally not measured. In CUR-AN patients the delay between HIV-1 diagnosis and entry into clinical care (first clinical visit) was a median of 15 weeks and for 25% of CUR-AN patients more than 2 years. Median time between diagnosis and entry in clinical care in patients treated in The Netherlands was 4–5 weeks. The median CD4 cell count at first clinical visit was significantly lower in CUR-AN than in NL-NL patients (p = 0.0004). CD4 cell counts at first clinical visit were not significantly different between the CUR-AN and NL-AN (p = 0.76) patients and NL-SUR (p = 0.82) patients. The viral load at first clinical visit was not significantly different among the four patient groups.
CUR-AN, Antillean HIV-1-infected individuals living in Curaçao; NL-AN, Antillean HIV-1-infected individuals living in The Netherlands; NL-SUR, Surinam HIV-1-infected individuals living in The Netherlands; NL-NL, Dutch HIV-1-infected individuals living in The Netherlands.
MSM, men having sex with men; IVDU, intravenous drug usage; IQR, interquartile range; CDC, Centers for Disease Control and Prevention; PI, protease inhibitor; NFV, nelfinavir; LPV/r, lopinavir/ritonavir; NNRTIs, nonnucleoside reverse transcriptase inhibitors; EFV, efavirenz; NVP, nevirapine.
HBsAg positivity. Reported p-values were obtained using Fisher's exact or Chi-square test for categorical variables and Mann–Whitney test for continuous variables comparing CUR-AN patients with each of the three groups treated in The Netherlands.
The median CD4 cell count at the start of cART was 141 cells/mm3 for CUR-AN patients and was lower when compared to the groups treated in The Netherlands with 180 cells/mm3 (p = 0.44) for NL-AN, 190 (p = 0.060) for NL-SUR, and 215 (p < 0.0001) for NL-NL patients. Of the CUR-AN patients for whom CD4 cell counts were available, 63% started cART with <200 cells/mm3. However, the proportion with an AIDS diagnosis at the start of cART was lower among the CUR-AN patients (15%) compared with the NL-AN (29%), NL-SUR (27%), and NL-NL (22%) patients.
Between 63% and 66% of the patients treated in The Netherlands started with an NNRTI-based cART regimen, whereas in Curaçao most starting regimens were PI based (p < 0.0001). In patients receiving an NNRTI-based first-line regimen, the most frequently prescribed NNRTI was efavirenz in all four groups. In patients receiving a PI-based first-line regimen, lopinavir/ritonavir was most frequently prescribed in all four groups. Zidovudine plus lamivudine (either individually or as combivir) was the most frequently prescribed NRTI combination to CUR-AN patients (90% of all patients), whereas tenofovir and emtricitabine (either individually or combined) was the most frequently prescribed NRTI combination in The Netherlands (56%).
Patient survival, follow-up, and clinical outcomes
The median follow-up time after starting cART for all 2118 patients was 1.61 years (IQR, 0.86–2.60); 93 (4%) had AIDS, 42 (2%) were lost to follow-up, and 92 (4%) died. Of all the deceased patients, 39 (42%) died of AIDS and 44 (48%) died due to a non-AIDS-related cause. For 9 patients (10%), the cause of death was unknown. The probability of patients being lost to follow-up was highest in the first half-year of treatment for all four groups. However, after 30 months of treatment, the CUR-AN and the NL-AN patients showed a higher rate of patients lost to follow-up [10% (95% CI, 5.6–17.7) and 8% (95% CI, 3.3–19.6), respectively] compared with the NL-SUR and NL-NL patients [3% (95% CI, 0.9–6.5) and 2% (95% CI, 1.1–2.6), respectively]. In an adjusted analysis the relative hazard for patients lost to follow-up compared with that among the CUR-AN patients was 0.44 for NL-AN patients (95% CI, 0.16–1.27; p = 0.13), 0.29 for NL-SUR (95% CI, 0.11–0.79; p = 0.01), and 0.14 for NL-NL (95% CI, 0.07–0.28; p < 0.0001) (Fig. 1A).
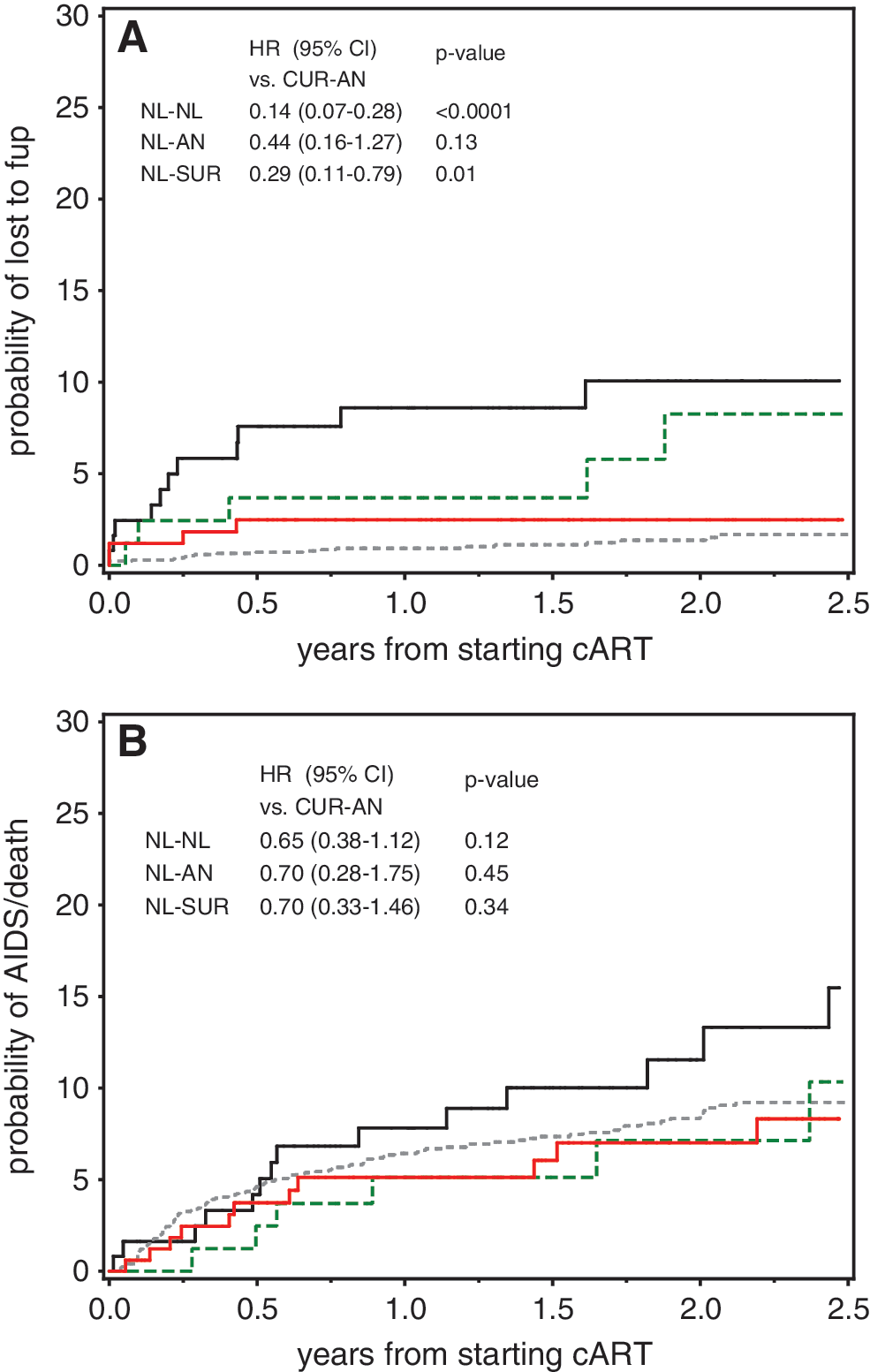
The probability of progression to AIDS or death after 30 months of cART was 10% (95% CI, 5.6–17.4) for the CUR-AN patients compared with 5% (95% CI, 1.9–13.1) for NL-AN, 6% (95% CI, 3.2–11.4) for NL-SUR, and 7% (95% CI, 6.1–8.8) for NL-NL. In adjusted analyses, the relative hazard for disease progression compared to the CUR-AN patients was 0.70 for the NL-AN patients (95% CI, 0.28–1.75; p = 0.45), 0.70 for NL-SUR (95% CI, 0.33–1.46; p = 0.34), and 0.65 for NL-NL (95% CI, 0.38–1.12; p = 0.12) (Fig. 1B). Apart from older age, predictive factors for the combined endpoint of AIDS or death in the CUR-AN group were a previous diagnosis of AIDS (HR, 2.25; 95% CI, 1.62–3.12; p < 0.0001) and a CD4 cell count < 200 cells/mm3 at the start of cART (HR compared to ≥200 cells/mm3 1.68; 95% CI, 1.18–2.40; p = 0.004).
The most frequent AIDS-defining diagnoses among CUR-AN patients were Pneumocystis jiroveci pneumonia (n = 3) and wasting syndrome (n = 2), among the NL-AN patients toxoplasmosis of the brain (n = 2), among the NL-SUR patients esophageal candidiasis (n = 2), and among the NL-NL patients Kaposi's sarcoma (n = 15) and Burkitt's lymphoma (n = 15).
Viral response
Kaplan–Meier estimates for the time after the start of cART to undetectable viral load (HIV-RNA plasma concentrations <80 copies/ml) are presented in Fig. 2 and show that the proportion of patients in the CUR-AN group with virological success was significantly lower compared to the groups treated in The Netherlands. At 12 months from the start of cART, the proportion of patients with virological success in the CUR-AN group was 76%, 87% in the NL-AN group, 93% in the NL-SUR group, and 96% in the NL-NL group.
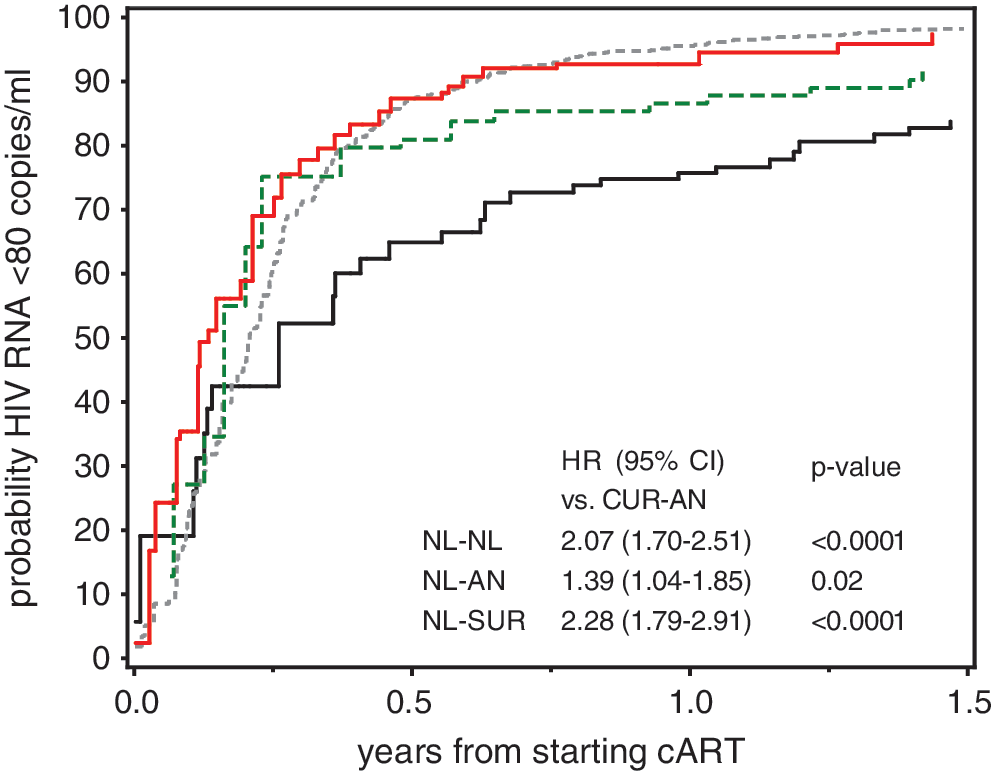
Kaplan–Meier curves of the probability of achieving undetectable viral load (<80 copies/ml) per study group up to 18 months after the start of antiretroviral therapy (cART). Solid black line CUR-AN: Antillean HIV-1-infected individuals living in Curaçao; dashed black line NL-AN: Antillean HIV-1-infected individuals living in The Netherlands; solid gray line NL-SUR: Surinam HIV-1-infected individuals living in The Netherlands; dashed gray line NL-NL: Dutch HIV-1-infected individuals living in The Netherlands; HR: adjusted hazard ratio.
In adjusted analyses, when differences in the frequency of HIV RNA measurement were taken into account, the relative hazard of successful virological response among NL-NL patients compared to CUR-AN patients was 2.07 (95% CI, 1.70–2.51; p < 0.0001), for NL-SUR it was 2.28 (95% CI, 1.79–2.91; p < 0.0001), and for NL-AN it was 1.39 (95% CI, 1.04–1.85; p = 0.02). Furthermore, patients starting cART with a PI-based regimen had a lower relative hazard of success when compared to patients starting with an NNRTI-based regimen (HR, 0.73; 95% CI, 0.66–0.80; p < 0.0001) independent of country of origin. Other variables associated with a shorter time to virological success were older age (HR per 10 year increase in age, 1.06; 95% CI, 1.01–1.10; p = 0.009) and a lower plasma viral load at the start of cART (HR of 4–5 log10 copies/ml vs. ≥ 5 log10 copies/ml 1.41; 95% CI, 1.28–1.56; p < 0.0001). Analysis of the interaction between baseline variables in the four different groups revealed that although there was no significant effect of age on the hazard in the NL-NL and NL-SUR groups (HR, 1.04 per 10-year increase in age; 95% CI, 0.99–1.08; p = 0.11), CUR-AN and NL-AN patients of older age had a significantly higher probability of virological success (HR, 1.18; 95% CI, 1.04–1.34; p = 0.01).
Immunological response
During the first 6 months after the start of cART, CD4 counts increased by 110 cells/mm3 (IQR, 66–173) among the CUR-AN patients (Fig. 3). This increase was significantly less than among patients treated in The Netherlands, which for NL-AN patients was 160 cells/mm3 (IQR, 90–220; p = 0.01, compared to CUR-AN), for NL-SUR 150 (80–230; p = 0.01), and for NL-NL 150 (80–240; p = 0.001). The absolute CD4 cell count 18 months after starting cART remained lowest among CUR-AN patients, 355 cells/mm3 (IQR, 230–505); this is compared with 425 cells/mm3 (IQR, 300–560; p = 0.37) among NL-AN patients, 400 (IQR, 280–485; p = 0.33) among NL-SUR, and 400 (IQR, 275–520; p = 0.006) among NL-NL. The mean overall change in CD4 cell count during the first 1.5 years after starting cART was not significantly different among the four patient groups in unadjusted and adjusted models. In adjusted analyses the difference in mean change in CD4 cell count among the NL-NL, NL-SUR, and NL-AN patients compared to the CUR-AN patients was 36 cells (95% CI, 3–69; p = 0.03), 0 (95% CI, −43–43; p = 0.99), and 47 (95% CI, −9–103); p = 0.11), respectively. Irrespective of origin and being treated in Curaçao or The Netherlands, patients older than 50 years at the start of cART had on average a smaller increase in CD4 cell count, 14 cells/mm3/year (95% CI, 0–29; p = 0.06). Furthermore, patients with an HCV coinfection had a lower increase of 46 CD4 cells/mm3/year (95% CI, 19–74; p = 0.0009) compared to patients without HCV coinfection, and female patients had an increase of 27 CD4 cells/mm3/year (95% CI, 6–47; p = 0.009) higher than male patients. A Cox regression analysis of the time from the start of cART to an increase of ≥100 CD4 cells/mm3 gave largely similar results for each patient group (data not shown).
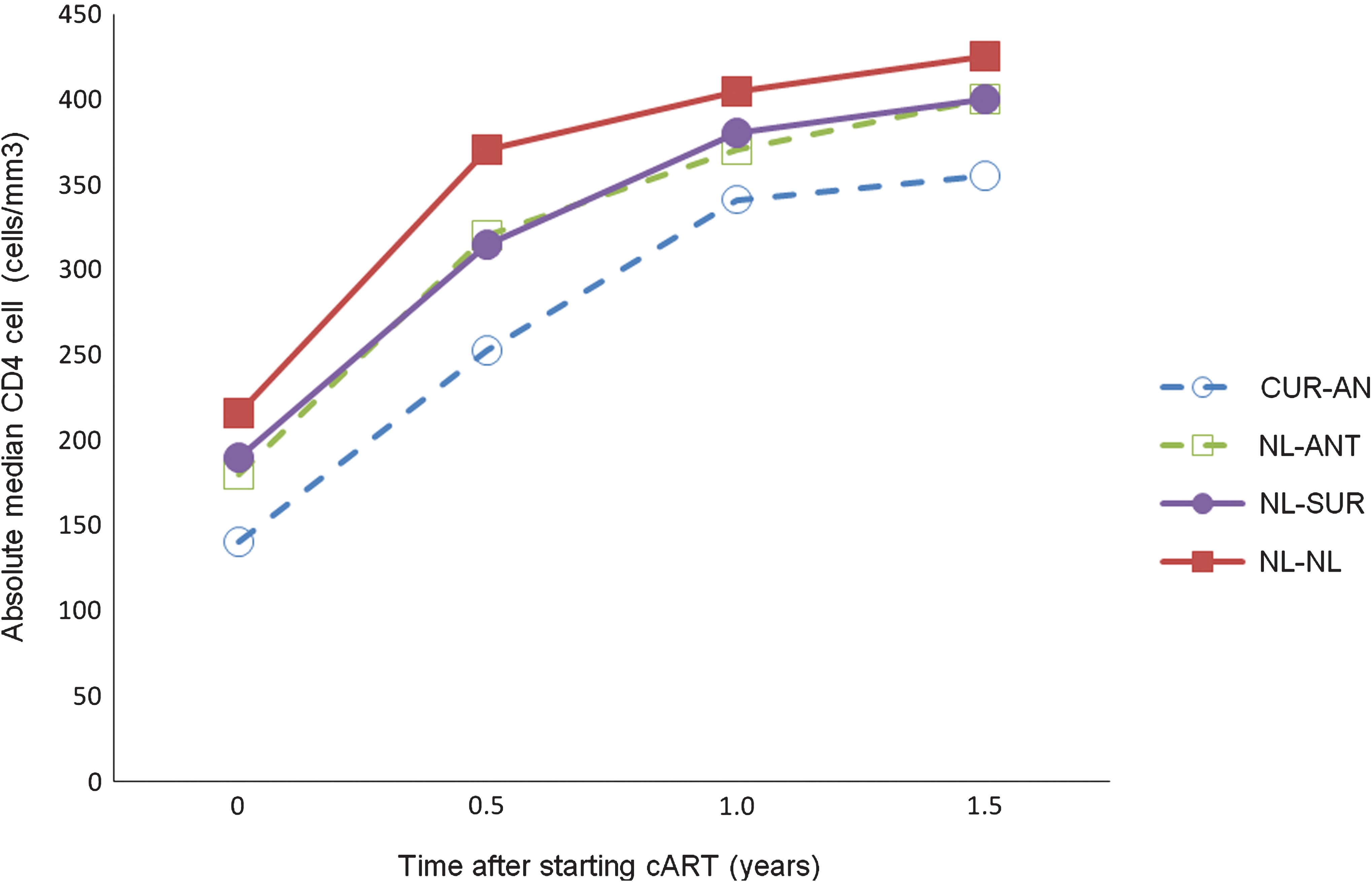
The absolute median CD4 cell count over time per study group up to 18 months after starting antiretroviral therapy (cART). CUR-AN: Antillean HIV-1-infected individuals living in Curaçao; NL-AN: Antillean HIV-1-infected individuals living in The Netherlands; NL-SUR: Surinam HIV-1-infected individuals living in The Netherlands; NL-NL: Dutch HIV-1-infected individuals living in The Netherlands.
First-line cART change
In total, 867 (47%) patients changed their first-line regimen during the first 18 months of follow-up. The Kaplan–Meier estimate of the proportion of patients who switched their first-line regimen to another after 18 months of cART was 34% in the CUR-AN group, 47% in the NL-AN (log-rank test, p = 0.01, compared to CUR-AN), 45% of the NL-SUR (p = 0.04), and 46% of the NL-NL group (p = 0.02). Overall, the most common reason for switching the cART regimen was because of adverse events.
Among CUR-AN patients 78% of all reported side effects were gastrointestinal adverse events vs. 36%, 52%, and 37% in the NL-AN, NL-SUR, and NL-NL patients, respectively. The most common adverse events in the groups treated in The Netherlands were neuropsychiatric side effects (57% of all reported side effects in the NL-NL group, 52% in NL-SUR, and 36% in NL-AN vs. 33% in CUR-AN).
After adjustment for baseline variables, the NL-AN, NL-SUR, and NL-NL patients had a significantly higher relative hazard for switching from the first-line cART regimen compared to the CUR-AN group [HR, 2.21 (95% CI, 1.40–3.48); 1.87 (95% CI, 1.25–2.80); and 2.15 (95% CI, 1.52–3.03), respectively]. A significant interaction was observed between the patient group and initial cART regimen. Whereas NL-NL, NL-SUR, and NL-AN patients starting on a PI-based had a significantly higher probability for a change in the regimen [HR compared to a NNRTI-based regimen, 1.76 (95% CI, 1.51–2.06); p < 0.0001], CUR-AN patients starting on a PI-based regimen had a lower probability for a change compared to patients on an NNRTI-based regimen [HR, 0.48; (95% CI, 0.25–0.93); p = 0.03].
Observed resistance patterns in all four groups were in accordance with the administered first-line regimens. Resistance to PIs was most commonly observed in the CUR-AN group, whereas resistance to NNRTIs was most commonly observed in the groups treated in The Netherlands (data not shown).
Discussion
We studied the CD4 cell and viral load responses to cART in a population of HIV-1-infected inhabitants of the island of Curaçao in the Caribbean and compared them to those found in HIV-infected patients treated in The Netherlands and who originated from The Netherlands Antilles, Surinam, or The Netherlands. The two major findings in the Antillean population treated in Curaçao were the late start of cART and the low virological response rate compared with the Antillean and Surinam patients treated in The Netherlands.
Diagnosis of HIV-1 in a late stage of infection is reported as a common finding in studies among Caribbean populations. 15,16 In the present study we report similar results, but also found late diagnosis of HIV-1 to be frequent among Antillean and Surinam populations living in The Netherlands. This may indicate that Caribbean sociocultural factors are playing a role in the acknowledgment of risk factors for HIV infection. 15
Studies done in both resource-rich 17 –19 and resource-limited settings 20,21 have shown the importance of higher CD4 T cell counts at the start of therapy for patient survival and clinical outcome. Tuboi et al. showed that patients with a lower median CD4 T cell count at the start of cART in seven locations throughout Latin America and the Caribbean tended to have higher mortality rates. 22 In our study more than half of the CUR-AN patients started cART late in the course of their infection.
Of concern is the less effective virological response to cART among CUR-AN patients compared to the Antillean and Surinam as well as the Dutch patients treated in The Netherlands. This lower virological response could be attributed to several factors.
First, a low CD4 cell count at the start of cART correlates with a decreased virological response to cART. 23 However, this only partly explains the low virological response of cART among CUR-AN patients since NL-AN and NL-SUR patients treated in The Netherlands also initiated cART at low CD4 cell counts, but those patients had significantly higher virological response rates than the CUR-AN patients. Studies of cART treatment in HIV-1-infected migrant populations in Europe showed comparable virological response rates over time. 9,24,25
Second, the virological response may be influenced by the use of various drug regimens. Although NNRTI-based regimens have been recommended as first-line cART both in the Caribbean region 26 and in The Netherlands, first-line PI-based regimens were prescribed more frequently for the CUR-AN patients than for the patients treated in The Netherlands. The time needed to achieve virological success appeared to be longer in patients treated with PI-based cART regimens in all four patient groups. Possible explanations could be a higher risk for suboptimal adherence due to the complexity of the regimen, drug–drug interactions, or a lower tolerability of PI-based regimens.
PI-based regimens used in The Netherlands are associated with a higher probability for changing first-line regimens than is NNRTI-based cART. However, the opposite was shown in patients treated in Curaçao. Physicians' personal preference plays an important role in deciding which antiretroviral drug combination therapy should be initiated and deciding when to switch as clinical care in Curaçao is provided by one single physician.
Poor adherence may cause low virological response and viral-load rebound. 27 When lost to follow-up was taken as a marker of adherence, the Antillean patients treated either in Curaçao or The Netherlands showed significantly higher rates of lost to follow-up compared to the Surinam and Dutch patients. Nellen et al. reported that patients from Surinam or Netherlands Antilles treated in The Netherlands are more prone to nonadherence characterized by patient-initiated treatment interruptions of more than 12 weeks. 25 In addition, antiretroviral drug availability may play a role in Curaçao because continuity in stock and logistics on small islands are more complicated than in West European countries such as The Netherlands.
The less effective virological response in the CUR-AN patients may have contributed to the low immunological response to cART. 28 More than half of the patients treated in Curaçao initiated cART with CD4 cell count <200 cells/mm3, leaving less opportunity for full recovery of the immune system over time. 18,29 –31 The NL-AN patients, who initiated cART at the same stage of infection, showed improved viral suppression, indicating that the ongoing viremia in the CUR-AN group indeed contributed to the CD4 cell decline. Furthermore, older age in the CUR-AN group could have contributed to the lower immunological response. 32
Although not significant, clinical outcome was less favorable in the CUR-AN patients compared to the patients treated in The Netherlands. However, owing to the lack of data for causes of death as well as the high lost-to-follow-up rates, the results from this analysis should be interpreted with caution. Because progression to AIDS and death for patients who were lost to follow-up was unknown, disease progression may have been underestimated among the CUR-AN patients. However, the sensitivity analyses of the virological and immunological response to cART suggest that the impact of lost to follow-up on the model estimates is small. Our analysis of virological responses accounted for the interval between the last measurement below and the first above 80 HIV-1 RNA copies/ml. Therefore it is unlikely that the lower virological response found in the CUR-AN patients results from a lower HIV-1 RNA measurement frequency. By checking for significant interaction between patient group and risk factors we aimed to correct for possible bias due to differences in sample sizes.
To our knowledge, our study is among the first to describe the long-term effects of first-line cART in a small Caribbean setting. When comparing the response to cART in an Antillean population treated in Curaçao to that in an Antillean, Surinam, and Dutch population treated in The Netherlands, we have shown that HIV-1-infected patients in Curaçao present late for care and treatment and respond less well to cART, most probably as a result of less adherence to the prescribed drug regimen.
Footnotes
Acknowledgments
This study was supported by a grant from The Netherlands Antillean Foundation for Higher Clinical Education (NASKHO). The authors would like to thank Y.M. Ruys and K. Laurant for data collection and entry and S. Ebeling for English language editing.
The authors acknowledge their gratitude to the members of the clinical and epidemiological working group of the ATHENA cohort study. (A list of the clinical sites participating in the ATHENA cohort study can be found at
Author Disclosure Statement
No competing financial interests exist.