
Abstract
Recent studies suggest that natural killer T (NKT) cells play a role in early antiviral pathogenesis and are rapidly depleted in chronic human immunodeficiency virus type 1 (HIV-1) clade B infection. We aimed to characterize the phenotypic and functional characteristics of NKT cells in HIV-1 clade C-infected Africans at different stages of HIV-1 disease. NKT cell frequencies, subsets, and ex vivo effector functions were assessed using multiparametric flow cytometry in a cross-sectional analysis of cryopreserved peripheral blood mononuclear cells from a cohort of 53 HIV-1 clade C chronically infected South African adults with CD4 T cell counts ranging from 94 to 839 cells/μl. We observed a significant decline of NKT cell numbers in advanced HIV-1 disease as well as activation and functional impairment of NKT cells in individuals with low CD4 T cell counts. The loss of NKT cells was largely driven by a reduction in the CD4+ and CD4–CD8– NKT cell subsets in advanced disease. These findings demonstrate significant impairment of the NKT cell compartment in progressive HIV-1 clade C disease that might play an important role in the modulation of immune function in HIV-1 infection.
Introduction
N
Several viruses such as herpes simplex and influenza viruses have developed immune-invasion strategies that impair CD1d-mediated antigen presentation 8,9 suggesting that NKT cells may play a key role in antiviral immunity. The precise role of NKT cells in HIV-1/SIV infection is not well understood, however, several studies have shown a reduced frequency of circulating NKT cells in chronic infection. 10 –12 Furthermore, it has been reported that initiation of highly active antiretroviral therapy (HAART) in conjunction with IL-2 treatment can result in rapid recovery of circulating subsets of NKT cells. 13,14 Interestingly, HIV-1 Nef can mediate down-regulation of CD1d expression by increasing CD1 internalization. 15,16 In addition, HIV-1 Vpu promotes evasion from CD1d-restricted immunity by inhibiting cell surface expression of CD1d and consequently the activation of NKT cells 17 suggesting that HIV-1 might have developed strategies to evade NKT-mediated immunity. These NKT cell studies have been largely performed in HIV-1 clade B-infected white populations, and very little is known about the impact of HIV-1 infection on overall NKT cell frequencies and function in sub-Saharan Africa where HIV-1 clade C is the most predominant subtype 18 and where genetic factors and comorbidities influencing antiviral immunity may differ from white populations.
In the current study, undertaken in a chronically HIV-1 clade C-infected adult cohort from KwaZulu-Natal, South Africa, we characterized the phenotypic and functional characteristics of NKT cells at different stages of HIV-1 disease in treatment-naive and HAART-treated HIV-1-infected subjects as well as uninfected controls. All experiments were performed using cryopreserved cells. We observed a significant decline in NKT cell numbers in advanced HIV-1 disease, strong activation of NKT cells in individuals with low CD4 T cell counts, and a reduced ability of NKT cells to produce cytokines following stimulation. These findings demonstrate significant impairment of the NKT cell compartment in progressive HIV-1 clade C disease.
Materials and Methods
Patients and samples
Plasma and peripheral blood mononuclear cell (PBMCs) samples were obtained from 53 chronically HIV-1-infected patients attending the Sinikithemba clinic at McCord Hospital and 10 HIV-1-negative subjects in Durban, South Africa. All patients had a serologic diagnosis of HIV-1 infection established prior to inclusion in the study. CD4+ T cell counts were quantified by flow cytometry (Becton-Dickinson, CA). Viral load (RNA copies/ml plasma) was measured by the Amplicor HIV-1 Monitor test version 1.5 (Hoffmann-La Roche). The study was approved by the University of KwaZulu-Natal Biomedical Research Ethics Committee and the Massachusetts General Hospital Institutional Review Board, and each subject gave written informed consent for participation.
Isolation of PBMCs
Cryopreserved PBMCs were thawed and then rested overnight in complete medium RPMI (Mediatech Inc., Manassas, VA) with 10% fetal bovine serum (FBS), 1%
In vitro stimulation
PBMCs were stimulated with or without phorbyl-12 myristate-13-acetate (PMA) and ionomycin, Golgi stop (BD Biosciences; San Jose, CA), 5 μg Brefeldin A (Sigma), and incubated for 6 h at 37°C in a humidified chamber with 5% CO2. The cells were washed with PBS supplemented with 2% FBS and resuspended in 200 μl of a 1:2000 dilution of αGalCer loaded CD1d tetramer. After 15 min at 37°C, the cells were washed and stained in the dark with violet amine-reactive viability dye for 15 min at room temperature. The cells were washed again and incubated with a cocktail of surface staining antibodies for 15 min in the dark at room temperature. After washing, the cells were fixed and permeabilized with Fix/Perm A & B (BD Biosciences, San Jose, CA) according to the manufacturer's instructions, and a mix of intracellular antibodies was added. Following a 20-min incubation at room temperature in the dark, the cells were washed a final time and stored at 4°C in the dark until acquisition.
Antibodies
Antibodies for surface staining included anti-CD57 FITC, anti-HLA-DR APC-Cy7, anti-CD38 PE, anti-CD57, anti-CD69 PE-Cy5, anti-CD8 Alexa 700, anti-CD19 V450 (BD Biosciences, San Jose, CA), anti-CD3 Cascade Yellow (Dako, Glostrop, Denmark), anti-CD4 Qdot 605 (Invitrogen, Carlsbad, CA), and α-galactosylceramide (αGalCer) or unloaded CD1d tetramer APC (NIH Tetramer Core Facility, Atlanta, GA). Additional antibodies for intracellular staining included anti-tumor necrosis factor (TNF)-α Alexa 488, anti-IFN-γ (BD Biosciences, San Jose, CA), and anti-IL-4 Pe-Cy7 (Ebioscience, San Diego, CA).
Flow cytometric analysis
Between 500,000 and 1,000,000 total events were acquired on an LSRII flow cytometer (BD Immunocytometry Systems, San Jose, CA) for each patient specimen. Mouse antibody capture beads (BD Biosciences, San Jose, CA) were used to prepare individual compensation tubes for each antibody used in the experiment. Data analysis was performed using FlowJo version 9.0.1 (TreeStar, Ashland, OR). The NKT cells frequency was expressed as a percentage of CD1d tetramer-positive cells per total live lymphocytes. The different CD4+, CD8+, CD4+CD8+, and CD4–CD8– NKT cell subset frequencies were expressed as a percentage of lymphocytes, using the initial lymphocyte gate. Reported data have been corrected for background staining.
Statistical analysis
Statistical analyses and graphic presentation were performed using Graph Pad Prism 5 (Graph Pad Software, San Diego, CA) and Microsoft excel. Results are given as means with standard deviations or medians with ranges. Paired two-tailed Student's t tests were used to test statistical significance between two study groups. One-way ANOVA analyses was used to compare multiple study groups. Differences after comparisons were considered statistically significant if p < 0.05.
Results
Characteristics of the study subjects
A total of 63 black South African participants from KwaZulu-Natal were enrolled into this study, 10 of whom were HIV-1 uninfected. Of the 53 HIV-1 clade C-infected subjects, all were in the chronic phase of disease. Eleven subjects had been treated with HAART for an average of 6 months (range 1–24 months), and had mean viral loads of 7310 copies per milliliter (range 50–26,410) and mean CD4 T cells counts of 373 per microliter of blood (range 94–839) at the time of sampling. Forty-two subjects were untreated and had mean viral loads of 124,623 (range 61,086–237,916) copies per milliliter and mean CD4+ T cell counts of 373 (range 86–948) per microliter of blood (Table 1). Individuals with CD4+ T cell counts below 200 cells per microliter were initiated on HAART according to the South African national treatment guidelines. HIV-1 viral loads and CD4+ T cell counts were inversely correlated in this cohort of 53 HIV-1-infected individuals (R = –0.4, p = 0.01).
CD4+ T cells per microliter of blood.
Viral load: copies of HIV-1 RNA per milliliter of blood.
n/a, not applicable.
Significant reduction in the percentage of NKT cells in progressive HIV-1 infection
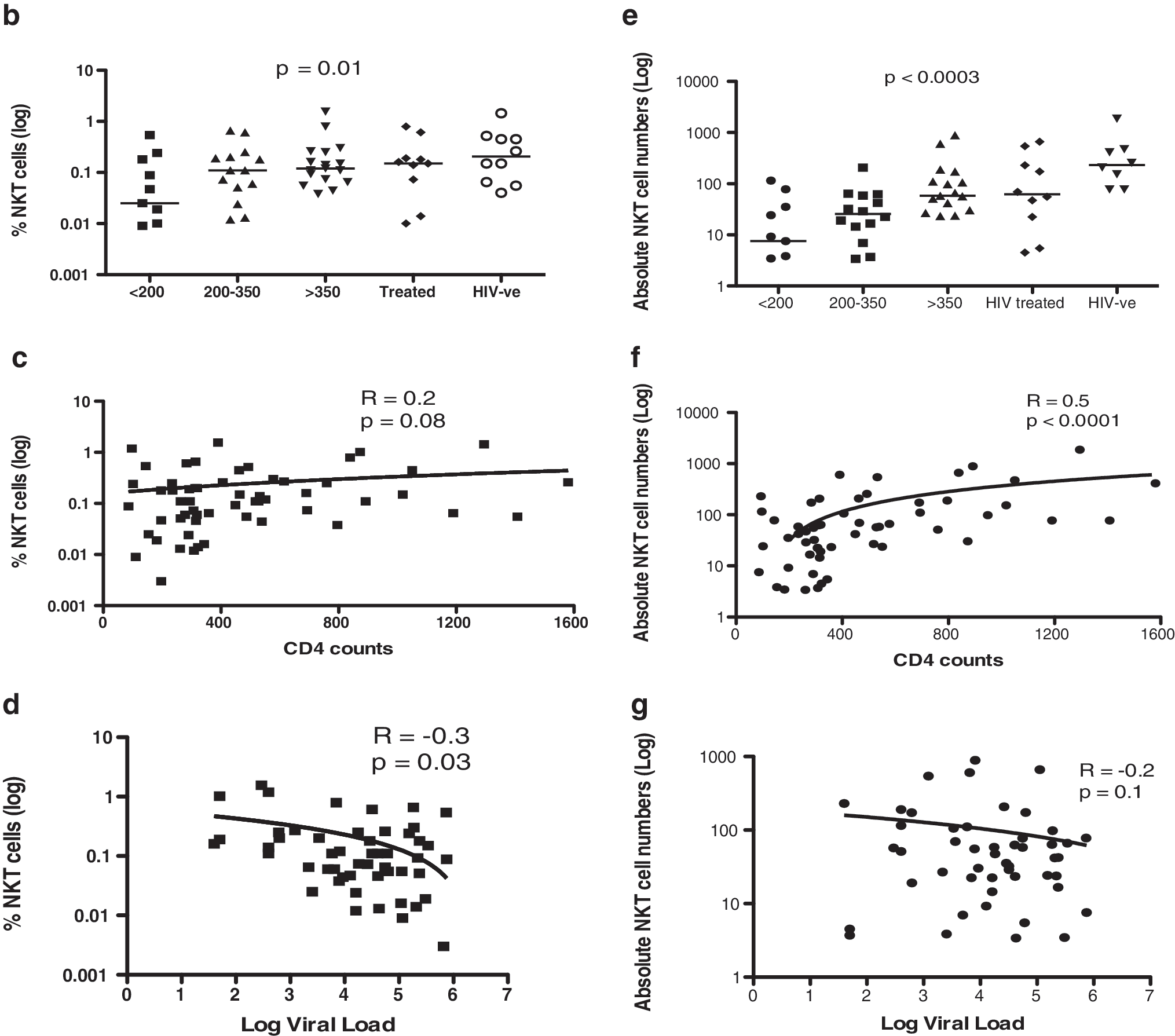
To assess the impact of HIV-1 disease on the frequency of NKT cells, we compared the percent CD1d tetramer-positive NKT cells in study subjects at different stages of HIV-1 disease to HIV-1-infected subjects treated with HAART and HIV-1-negative subjects (Fig. 1). As shown in Fig. 1b, untreated HIV-1-positive individuals with CD4+ T cell counts <200 T cells/μl had a reduced percentage of CD1d tetramer-positive NKT cells compared to HIV-1-uninfected controls. Overall, absolute CD4+ T cell counts were directly correlated to the frequency of NKT cells in the study subjects; however, this correlation did not reach statistical significance (Fig. 1c, R = 0.2; p = 0.08). Furthermore, there was an inverse correlation in HIV-1-infected individuals between HIV-1 viral load and the percent of NKT cells (R = –0.3; p = 0.03). The absolute numbers of NKT cells were also significantly depleted as HIV-1 disease progressed (Fig. 1e; p = 0.003). The CD4+ T cell counts were furthermore directly correlated to the absolute number of NKT cells in this study population, and this correlation reached statistical significance (Fig. 1f, R = 0.5; p < 0.0001). Taken together, these data demonstrate decreased NKT cell frequencies in advanced HIV-1 clade C infection.

Significant reduction of NKT cells in advanced HIV-1 clade C infection.
NKT cell subsets in chronic HIV-1 infection
CD4+ T cells are susceptible to HIV-1 infection, 9 and it has been shown that HIV-1 can directly infect CD4+ NKT cells. 19 We therefore investigated changes in CD4+, CD8+, CD4+CD8+, and CD4–CD8– NKT cell subsets in the study subjects at different stages of HIV-1 disease compared to HIV-1-infected subjects treated with HAART and HIV-1 negative subjects (Fig. 2a). The percent CD1d tetramer-positive CD4+ NKT cells decreased in advanced HIV-1 infection and a significant direct correlation was observed between CD4+ NKT cell population (R = 0.3; p = 0.03) and CD4 T cell counts (Fig. 2b). However, even after adjusting for decreased CD4 T cell counts, the percentage of CD4+ NKT cells was still reduced in advanced HIV-1 disease (data not shown). No significant correlation was observed between the percent CD1d tetramer-positive CD8+ NKT cells and CD4+ T cell counts (Fig. 2c). In addition, the percent CD1d tetramer-positive CD4–CD8– NKT cells was significantly lower in HIV-1-infected compared to the HIV-1-uninfected individuals (p = 0.01; Fig. 2d), and a significant positive correlation was observed between the CD4–CD8– NKT cell population and CD4 T cell counts (p < 0.001; R = 0.3). No significant correlation was observed between the percent CD1d tetramer-positive CD4+CD8+ NKT cell population and CD4 T cell counts (Fig. 2e).
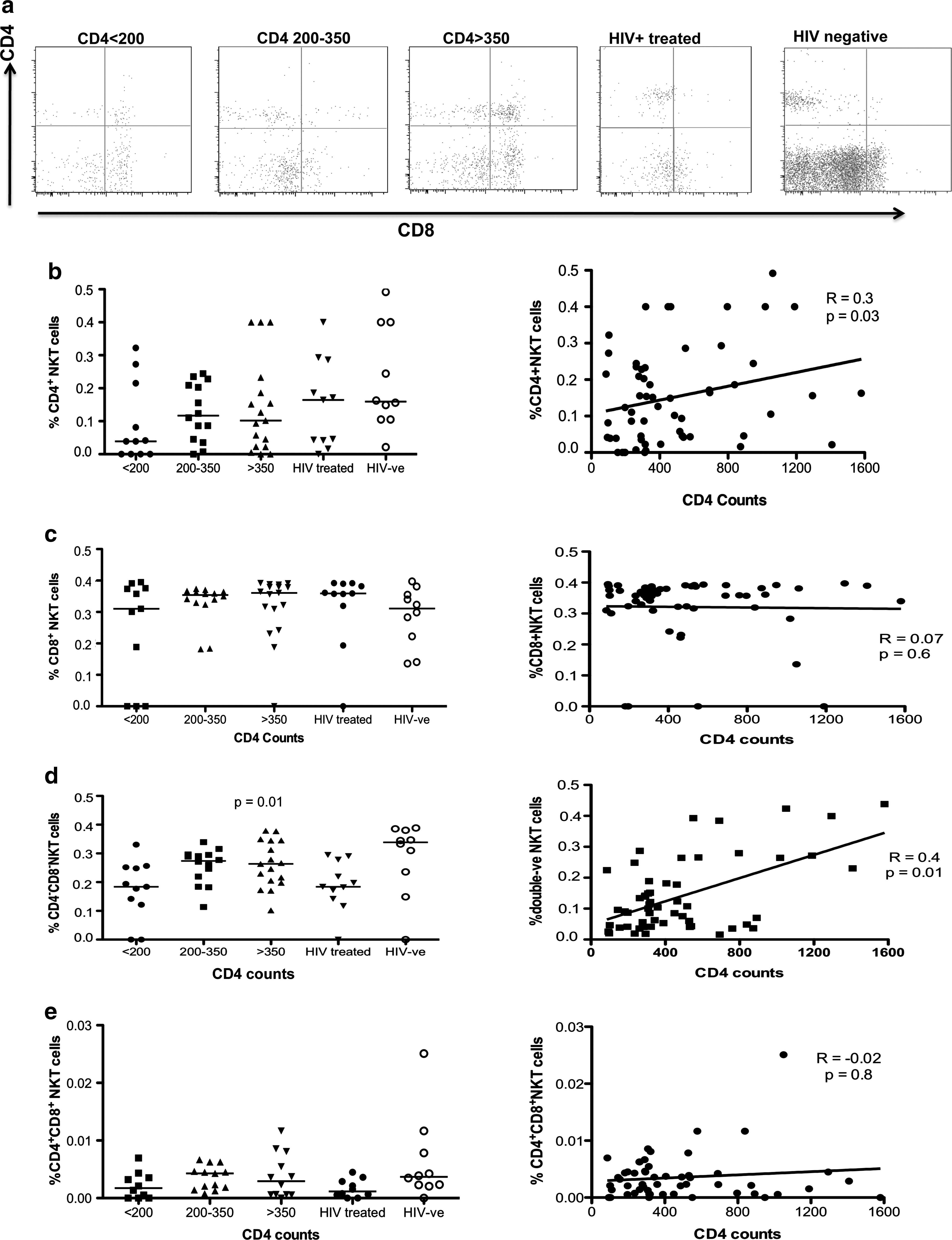
CD4/8 T cell distribution in NKT cells.
Overall, the fraction of CD4+CD8+ NKT cells was very small (less than 5% of all NKT cells, data not shown), while the majority of NKT cells at all disease stages expressed CD4+ or represented double negative (CD4–CD8–) NKT cell subsets. None of the NKT cell subset frequencies correlated with viral loads (data not shown). Taken together, these data show that there are differential consequences of chronic HIV-1 infection on the frequencies of NKT cell subsets, with a significant reduction of CD4+ NKT and CD4–CD8– NKT cell subsets.
Phenotypic characterization of activated NKT cells in HIV-1 disease progression
HIV-1 viremia is associated with persistent activation of the immune system, affecting several cell subsets,
20,21
but the impact of HIV-1 clade C infection on NKT cell activation has not been reported to date. We therefore assessed the levels of NKT cell activation in this cohort using antibodies against CD38 and CD69. As shown in Fig. 3,
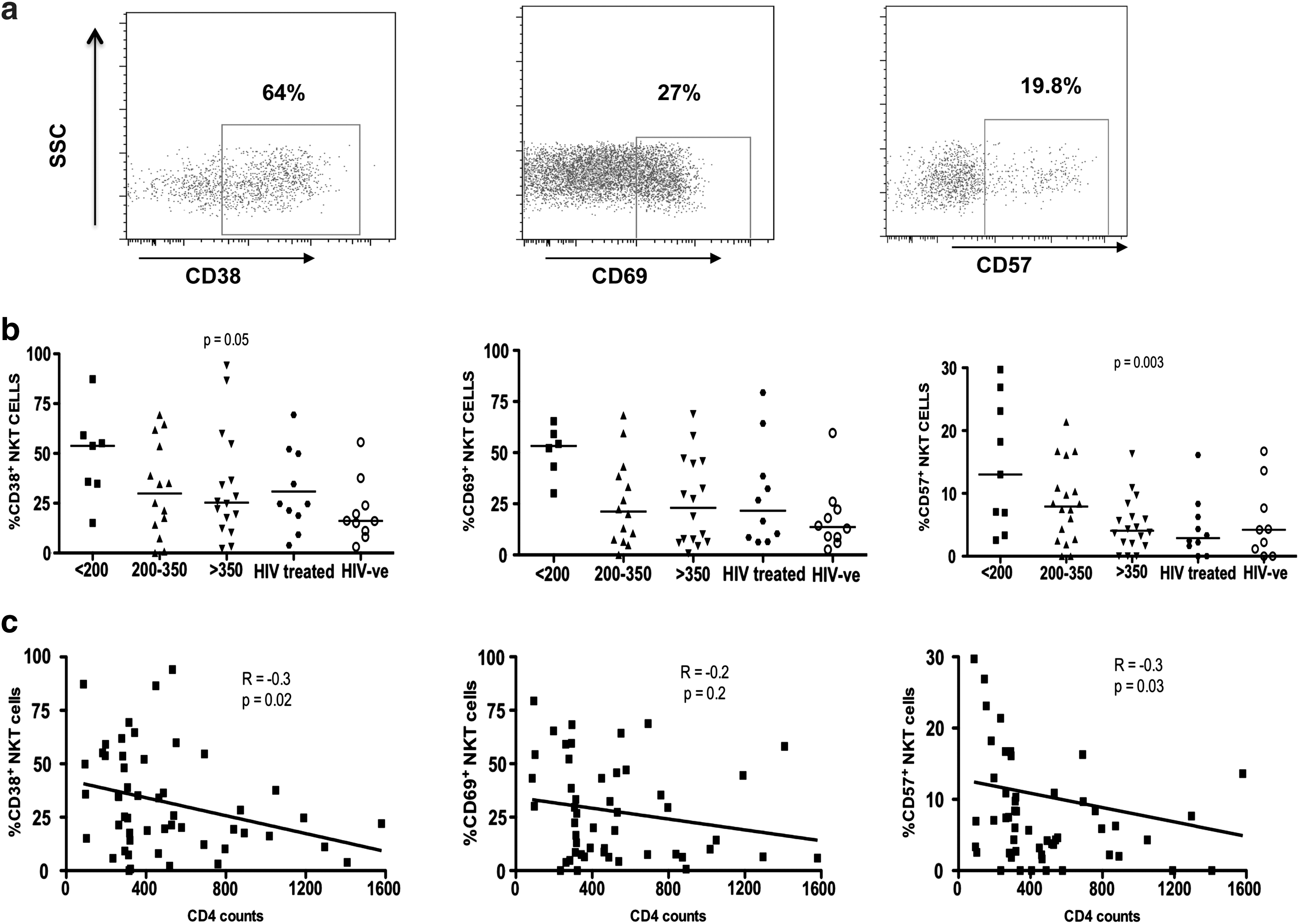
Assessment of markers of immune activation on NKT cells.
Previous studies have shown that chronic HIV-1 infection can result in the expression of CD57, which represents a senescence marker on both adaptive and innate immune cells. 5,22 –24 Similar to the increased expression of activation markers, significantly higher percentages of NKT cells expressed CD57 in individuals with low CD4 T cell counts (p = 0.003; Fig. 3b), and the percentage of CD57+ NKT cells was inversely correlated with CD4 T cell counts (R = –0.3; p = 0.03; Fig. 3c). Again, CD57 expression on NKT cells did not correlate with viral load (data not shown). Taken together, these data demonstrate that significantly more NKT cells are activated in advanced HIV-1 disease, and that these cells express markers of senescence.
Advanced HIV-1 disease affects NKT cell ability to produce cytokines
NKT cells can regulate both adaptive and innate immune responses through the production of Th1 cytokines such as IFN-γ and Th2 cytokines such as IL-4. 5,24 To determine the functional capacity of NKT cells in different stages of chronic HIV-1 infection, we measured the ability of NKT cells from HIV-1-infected individuals who had positive responses above background to produce IFN-γ, TNF-α, and IL-4 after stimulation with PMA/ionomycin, and compared this with healthy individuals (Fig. 4). In HAART-treated individuals, background cytokine production in the unstimulated cells was high and no NKT cell cytokine responses above background were detected. The proportion of NKT cells that produced IFN-γ, TNF-α, and to a lesser extent IL-4 after stimulation was higher in individuals with high CD4 T cell counts (Fig. 4b), but there was no direct correlation between cytokine production by NKT cells and CD4 T cell count (Fig. 4c). Furthermore, no correlation between the ability of NKT cells to produce cytokines and HIV-1 viral load was observed (data not shown). Taken together, these data show that advanced HIV-1 disease alters NKT cell frequency and activation status and also reduces the ability of NKT cells to produce cytokines following PMA/ionomycin stimulation.

Expression of IFN-γ, TNF-α, and IL-4 in NKT cells.
Discussion
Natural killer T (NKT) cells are innate immunoregulatory cells that comprise approximately 0.5% of peripheral lymphocytes and are involved in the recruitment and activation of other immune effector cells. 25 Previous studies have reported reduced numbers of NKT cells in chronic HIV-1 clade B infection, 11,12 and longitudinal studies revealed that NKT cell down regulation and depletion occur largely during the first year after HIV-1 seroconversion. 26 However, no studies have yet assessed the impact of HIV-1 infection on NKT cell number and function in sub-Saharan Africa where HIV-1 clade C is the predominant subtype. 18 Here we studied the phenotypic and functional characteristics of NKT cells in HIV-1 clade C-infected Africans with CD4+ T cell counts ranging from 86 to 948/μl, and observed a significant decline and functional impairment of NKT cells in advanced HIV-1 clade C disease, in line with previous findings observed in HIV-1 clade B and SIV infection. 10 –12,26
NKT cells are thought to play a central role in regulating immune responses to pathogens, including viral infections. 8,27 In HIV-1 infection, many of these pathways have been shown to be dysregulated. 28,29 In addition, high levels of persistent immune activation characterize chronic viremic HIV-1 infection, and the levels of immune activation have been closely associated with CD4 T cell count decline and clinical HIV-1 disease progression. 20,21 In our investigation of changes in the NKT cell compartment in advanced HIV-1 clade C disease, we observed that significantly more NKT cells are activated in advanced HIV-1 disease, in particular in those individuals with low CD4 T cell counts <200 cells/μl. Furthermore, the frequency and absolute number of NKT cells were lower in advanced chronic infection, and their ability to produce cytokines, in particular TNF-α, was reduced. This is in line with a previous study demonstrating that NKT cells from individuals with chronic HIV-1 infection have elevated programmed death-1 (PD-1) expression corresponding to an exhausted phenotype. 9 Taken together, the heightened and persistent immune activation observed in chronic HIV-1 infection might therefore result in activation and accelerated proliferation of NKT cells, leading to their functional impairment and deletion, as previously suggested for other cell subsets, such as effector memory CD4 T cells. 30,31
Different NKT cell subsets differ in their expression of CD4 T cells, and might therefore be differentially affected by HIV-1 infection. 10,11 While we observed a direct correlation between the overall frequency of NKT cells and absolute CD4+ T cell counts, differences emerged when changes within these different NKT cell subsets were assessed. The frequencies of the predominant CD4+CD8– and CD4–CD8– NKT cell populations were reduced in HIV-1-positive compared to HIV-1-negative individuals. This result suggests that the overall decline observed here and previously described for NKT cells in chronic HIV-1 infection is primarily due to the depletion of these subsets. Future studies will need to address the specific mechanisms by which chronic HIV-1 infection leads to the preferential loss of these subsets and in particular the double negative NKT cells from the peripheral circulation.
HIV-1-infected individuals on HAART had a higher percentage of circulating NKT cells and a reduced expression of activation and senescence markers on NKT cells compared to untreated individuals, despite a relatively short time on HAART (range 1–24 months) and without full suppression of viremia. These results are in line with previous studies showing that following the initiation of HAART, NKT cell frequencies recover rapidly, mainly by the redistribution of previously sequestered cells. 14,32,33 Reconstitution of the NKT cell compartment during HAART might therefore contribute to the reduced susceptibility of infected individuals on HAART to opportunistic infections, since NKT cells have been shown to play a critical role in protective immunity to many infections observed in immunocompromised individuals, possibly including Mycobacterium tuberculosis. 34,35
In summary, our data demonstrate a significant impairment of NKT cells, particularly in advanced stages of chronic HIV-1 clade C infection. A better understanding of the role of NKT cells in the regulation of HIV-1 immune activation and associated exhaustion and immunity to opportunistic infections will be needed to determine therapeutic strategies aimed at restoring the NKT cell compartment.
Footnotes
Acknowledgments
We thank Helga Holst and the staff and patients at the Sinikithemba clinic, McCord Hospital. These studies were supported by the Howard Hughes Medical Institute through the KwaZulu-Natal Research Institute for TB and HIV (K-RITH), the Doris Duke Charitable Foundation, the South African Department of Science and Technology/National Research Foundation Research Chair Initiative, and the Mark and Lisa Schwartz Foundation. The Ragon Institute Fund for Innovation and New International Initiatives provided additional support. M.W.M. is supported by a Fogarty International Clinical Research Fellowship (FICRF R24 TWOO 7988), and R.M. was supported by the Columbia University-Southern African Fogarty AIDS International Training and Research Programme (AITRP) funded by the Fogarty International Center, National Institutes of Health (Grant D43TW00231). M.W.M., K.C., and R.M. contributed equally and serve as shared first authors. M.A. and T.N. contributed equally and serve as shared corresponding authors.
Author Disclosure Statement
No competing financial interests exist.