
Abstract
The objective of this study was to analyze recent infections and the molecular epidemiology of human immunodeficiency virus type 1 (HIV-1) among different risk groups since the outbreak of circulating recombinant form CRF07_BC among intravenous drug users (IDUs) in 2004 in Taiwan. Phylogenetic analysis was performed using the env and pol fragment sequences amplified from these specimens. The BED IgG capture incidence EIA (BED-CEIA assay) was used to determine recent infections. Among the 683 HIV-1-positive individuals enrolled between 2007 and 2009, 394 (57.7%) were subtype B, 260 (38.1%) were CRF07_BC, 26 (3.8%) were CRF01_AE, two (0.3%) were CRF08_BC, and one (0.1%) was CRF06_cpx. While the percentage of CRF07_BC decreased (58.5–17.9%, p < 0.001) from 2007 to 2009, the percentage of subtype B increased (37.6% to 74.9%, p < 0.001). A concordant decrease in the proportion of recent infections to new infections among IDUs (63.6% to 9.8%, p < 0.001), accompanied with an increase of the proportion of recent infections in MSM (men having sex with men) (22.4–67.1%, p = 0.77) and heterosexual groups (13.1– 23.2%, p = 0.852), was observed. The decrease in CRF07_BC infections and the reduction in the proportion of recent infections among IDUs reflected the success of harm reduction strategies initiated by the government in 2005.
Introduction
H
In Taiwan, the first indigenous AIDS case was reported in 1985. 2 By the end of 2009, a cumulative total of 18,378 HIV-1-infected individuals was reported to the Taiwan Centers for Disease Control. 3 The distribution of HIV-1 subtype viruses from HIV-1-infected persons reported between 1988 and 2000 indicated that subtype B (69.4%) was the most prevalent, followed by CRF01_AE (27.3%) and subtype C (1.3%). 4,5 Nevertheless, an outbreak of HIV-1 CRF07_BC infections among intravenous drug users (IDUs) in Taiwan in 2004 6 –8 dramatically increased the percentage of individuals infected with HIV-1 CRF07_BC (53.4%), which then became the predominant HIV-1 subtype in Taiwan. 9
To control the spread of HIV among IDUs, the government implemented a “Harm Reduction Programme” in August 2005, which is composed of three parts as described below. (1) Information, education, and communication. Expanding HIV testing and monitoring of drug users were adapted to detect new cases and provide timely health education information and communication to correct dangerous behavior. (2) A needle-syringe program (NSP). By November 2010, 930 sites provided IDUs with clean syringe paraphernalia, dilution buffer, educational materials, guidance, and counseling to decrease HIV transmission by the use of HIV-contaminated needles and syringes. (3) Methadone substitution treatment. The major thrust of methadone substitution treatment is providing long-term oral methadone treatment to IDUs as a substitute for comparatively risky intravenous drug use. 10 By November 2010, 100 hospitals and clinics offered substitution treatment services in Taiwan.
The aim of this study was to monitor the distribution of HIV-1 subtypes and HIV-1 recent infections among different risk groups between 2007 and 2009 in Taiwan after the HIV-1 CRF07_BC outbreak in 2004, and to evaluate the effectiveness of the harm reduction program initiated by the government in 2005.
Materials and Methods
Specimen collection
Stratified sampling weighted for the proportion of HIV-1-seropositive patients among different risk groups was performed, and the newly diagnosed patients were selected from different risk groups based on the specified proportion in each year (2007–2009). A total of 683 HIV-seropositive individuals who were reported to the Taiwan Centers for Disease Control between 2007 and 2009 were enrolled for the study. All blood samples were confirmed for HIV infection by Western blot assay (WB) (New LAV Blot I; Bio-Rad, Marnes la Coquette, France) or polymerase chain reaction (PCR) assay (RealTime HIV-1; Abbott, Des Plaines, IL). This study was reviewed and approved by the ethics committee of the Taiwan Centers for Disease Control (DOH97-CDC-2011, DOH98-CDC-2016).
HIV-1 seroconversion
An IgG capture enzyme immunoassay was used to measure the proportion of HIV-1-specific IgG in blood samples among the total IgG for the purpose of identifying infections that were acquired recently. The BED-CEIA (capture enzyme immunoassay; Calypte, MD) is a commercial product, using a trimeric branched peptide. Each branch is composed of a synthetic oligopeptide derived from the immunodominant region of the gp41 glycoprotein of HIV-1 subtypes B, CRF01_AE, and D. 11 It was performed according to the manufacturer's instructions by technicians trained in the use of the assay. Briefly, test specimens were initially run singly. If the normalized OD (ODn) was >1.2, the specimen was classified as being from a long-term seroconverter. Specimens with ODn ≤1.2 were tested again in triplicate to confirm the values. In confirmatory testing, specimens with ODn values ≤0.8 were considered a recent seroconversion. 12 If the ODn of the specimen was >0.8, the specimen was considered a long-term seroconversion.
Nested PCR
HIV-1 viral RNA was extracted from plasma samples with the QIAamp Viral RNA kit (Qiagen, CA) according to the manufacturer's instructions. Nested PCR was performed to generate the C2-V3 fragment of the env gene (nucleotide number, nt 7368–8704) and the pol fragment, containing the entire protease region and the first 335 codons of the reverse transcriptase (nt 2253–3548). 9 Briefly, the C2-V3 fragment was amplified using a Superscript III One-Step RT-PCR kit (Invitrogen, Carlsbad, CA). The broadly reactive first primer set was 1-CV-F (5′-ACA GTR CAR TGY ACA CAT GG-3′) and 1-CV-R (5′-CAC TTC TCC AAT TGT CCI TCA-3′). Thermal cycling conditions were composed of a reverse transcription reaction of 55°C for 30 min and a PCR reaction as follow: 94°C for 2 min, 35 cycles of 94°C for 15 s, 55°C for 30 s, 68°C for 1.5 min, and 68°C for 5 min. The second primer set was 2-CV-F (5′-CTG TTI AAT GGC AGI CTA GC-3′) and 2-CV-R (5′-RAT GGG AGG RGY ATA CAT-3′), and the PCR condition was the same as for the first PCR condition. The pol fragment was generated using the ViroSeq HIV-1 Genotyping System Version 2.8 (Celera Diagnostics, Alameda, CA) according to the manufacturer's recommendations. The RT and PCR amplifications were carried out with appropriate negative controls to detect any possible contamination during the experiments.
Phylogenetic analysis
The PCR products were subjected to a sequencing reaction using the ABI PRISM 3130 Genetic Analyzer (Applied Biosystems, Foster, CA). Sequence fragments were assembled with the Sequencher 4.1.4 software (Gene Codes, Ann Arbor, MI) and aligned with Clustal W. 13 Phylogenetic tree analyses of the C2-V3 and pol fragment sequences were performed using the neighbor-joining method based on a maximum composite likelihood model with 1000 bootstrap replicates, using MEGA version 4.0. 14 DNAML from PHYLIP version 3.6.8 was used to construct a maximum-likelihood tree to verify the topology of taxas shown in the neighbor-joining tree. 15
Nucleotide sequence accession numbers
The GenBank accession numbers of sequences used in this study are HQ657357–HQ658039, AB220944, AB253421, AB253429, AB286851, AF004885, AF005494, AF005496, AF061641, AF064699, AF075703, AF077336, AF082394–95, AF084936, AF103818, AF190127-28, AF286226, AF286229, AF286237–38, AF377956, AJ249235–39, AY008715, AY173951, AY180905.1, AY253311, AY271690, AY331295, AY371157–58, AY423387, AY531116.1, AY535659, AY612637, AY772699, DQ2308411, DQ2308421, DQ373066, DQ676872, EF0782782, EF368370, EF368372, EF614151, K03454–55, L39106, U46016, U54771, U71182.1, U88824, U88826, and GU299789–90.
Statistical analysis
Categorical variables were compared using the χ2 test whereas noncategorical variables were compared using the Student's t test. All tests were two-tailed and a p value <0.05 was considered significant.
Results
The trend of HIV-1 infection among IDUs in Taiwan
By the end of 2009, a cumulative total of 18,378 HIV-1-infected individuals was reported to the Taiwan Centers for Disease Control. Among these, 6330 HIV-1-infected individuals were IDUs. As shown in Fig. 1, the number and percentage of IDUs has increased rapidly since 2002, and reached a peak in 2005. The proportion of IDUs infected with HIV-1 increased gradually from 2.5% (19/768) in 2002 to 9.2% (79/860) in 2003, but jumped to 40.5% (616/1521) in 2004 and to 71.3% (2410/3381) in 2005. The proportion slowly declined to 62.7% (1833/2922) in 2006, and further decreased to 37.9% (733/1932) in 2007, to 22.0% (384/1746) in 2008, and to 10.7% (177/1648) in 2009. 16
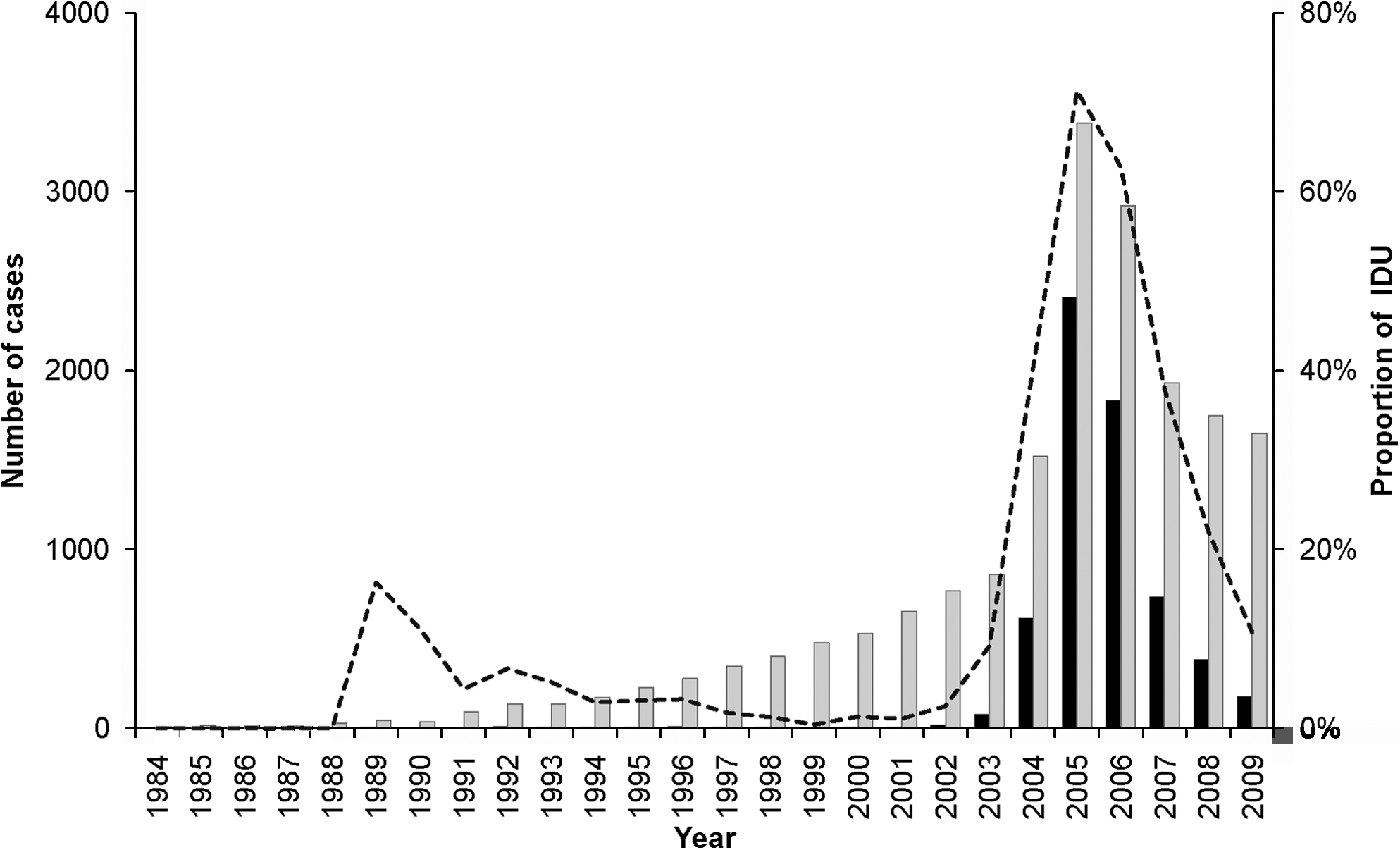
The trend of HIV-1 infection in IDUs in Taiwan. The dotted line indicates the proportion of IDUs; the gray bar indicates the total number of HIV-1 infections; the black bar indicates the number of IDUs infected with HIV-1.
Distribution of HIV-1 subtypes and risk behaviors in HIV-infected individuals between 2007 and 2009
In this cross-sectional study, 683 HIV-1-positive individuals were reported to the Taiwan Centers for Disease Control between 2007 and 2009 and were processed successfully for sequencing and phylogenetic analysis. Among these, 394 (57.7%) were subtype B, 260 (38.1%) were CRF07_BC, 26 (3.8%) were CRF01_AE, two (0.3%) were CRF08_BC, and one was CRF06_cpx. The yearly distribution of HIV-1 subtypes is summarized in Table 1. The percentage of subtype B increased from 37.6% in 2007 to 74.9% in 2009 (p < 0.001). However, the percentage of CRF07_BC decreased from 58.5% in 2007 to 17.9% in 2009 (p < 0.001). The risk behaviors of these individuals were investigated to illustrate the entire picture of the distribution of the risk factors among these HIV-1-positive individuals. As shown in Table 1, the predominant risk behaviors were men having sex with men (MSM) (44.1%), IDUs (33.7%), and heterosexuals (21.8%). Only one case was mother-to-child transmission, and two had unknown risk factors for HIV transmission. While the trends of MSM (24.5–57.9%, p < 0.001) and heterosexuals (17.9–26.7%, p = 0.093) increased, the trend of IDUs decreased (56.8–15.4%, p < 0.001).
CRF, circulating recombinant form; MSM, men having sex with men; IDU, intravenous drug user; MTCT, mother-to-child transmission; SD, standard deviation.
Indicates the percentage of HIV subtype/CRF is significantly different (p < 0.05) between 2007 and 2008.
Indicates the percentage of HIV subtype/CRF is significantly different (p < 0.05) between 2008 and 2009.
Distribution of HIV-1 subtypes and CRFs among different risk groups
As shown in Table 2, the prevalence of HIV-1 subtype/CRF in MSM was 295 (98.0%) subtype B, four (1.3%) CRF01_AE, and only two (0.7%) CRF07_BC. In heterosexuals, 90 (60.4%) were subtype B, 37 (24.8%) were CRF07_BC, 19 (12.8%) were CRF01_AE, two (1.3%) were CRF08_BC, and only one (0.7%) was CRF06_cpx. In IDUs, CRF07_BC was the most prevalent (95.7%). In addition, one vertical transmission case was enrolled in this study, which was CRF07_BC.
CRF, circulating recombinant form; MSM, men having sex with men; IDU, injection drug user; MTCT, mother-to-child transmission.
Recent infections among HIV-1-positive individuals
Among the 683 HIV-1-positive individuals, 299 individuals (43.8%) were identified as recent infections by the BED-CEIA assay. As shown in Table 3, the proportion of recent infections decreased from 46.7% in 2007 to 42.1% in 2009 (p = 0.420). A drastic increase of MSM in recent infections was observed from 2007 (22.4%) to 2008 (68.2%) (p < 0.001), while a great reduction of IDU was simultaneously monitored (63.6–10.9%, p < 0.001). A similar trend was observed in subtype distribution, with a major increase in subtype B (29.9–85.4%, p = 0.013) and a decrease in CRF07_BC (69.2–12.2%, p < 0.001).
CRF, circulating recombinant form; MSM, men having sex with men; IDU, intravenous drug user; MTCT, mother-to-child transmission.
p value indicates a significantly difference (p < 0.05) between 2007 and 2009.
Discussion
The AIDS Prevention and Control Act from December 1990 serves as the legal basis for the HIV/AIDS control policy in Taiwan. The Act stipulates that clinicians have the responsibility to report HIV/AIDS cases, within 24 h, to local health authorities. For active surveillance, the Taiwan government has been undertaking mandatory screening of blood donors for HIV since 1988, military draftees since 1989, prison inmates since 1990, and foreign laborers since 1991. A screening program for pregnant women was launched in 2005. Although there is no mandatory HIV testing for pregnant women, each of them will receive an HIV/AIDS educational pamphlet and be encouraged by their obstetricians to take a free HIV test (paid by the government) during prenatal care. 17
Before 2004, the HIV epidemic grew slowly and the major transmission pathway for HIV infection was sexual contacts. However, the number of newly reported HIV-positive individuals has risen sharply since 2004, and IDUs have become the largest contributing risk behavior to the HIV/AIDS epidemic in Taiwan. With the first HIV-infected IDU reported in 1988, subtype B was the predominant subtype among IDUs and the prevalence was kept very low for almost 15 years. 18 However, an outbreak of HIV-1 CRF07_BC infections among IDUs was reported in 2004. Ninety-eight percent of IDUs were infected with CRF07_BC, which thus surpassed subtype B and became the predominant subtype among HIV-infected individuals in Taiwan. 19
The HIV incidence in cities with an NSP decreased significantly from 13.9 to 13.3 per 100,000 persons, while an increase of HIV incidence from 11.5 to 15.3 per 100,000 persons was observed in cities without an NSP. 10 The number and percentage of IDUs have increased rapidly since 2002, and reached a peak in 2005, then decreased after 2006. As shown in Table 1, the percentage of CRF07_BC decreased significantly from 58.5% in 2007 to 17.9% in 2009. Furthermore, the proportion of IDU in individuals who showed evidence of recent infection also decreased significantly (63.6–9.8%, p < 0.001). These data indicate that the Harm Reduction Program indeed decreased the spread of HIV among IDUs in Taiwan.
The distribution of certain HIV subtypes in different risk groups was noticed (Table 2). As reported previously, 6,20 subtype B and CRF07_BC were mainly circulating among MSM and IDU groups, respectively. No introduction of CRF07_BC into the MSM group was observed. The observation that 24.8% of heterosexuals were infected with CRF07_BC might be derived from survey bias. Since injection drug use was a criminal offense in Taiwan, some IDUs might be afraid of identifying themselves as IDUs. Such a bias might underestimate the distribution of IDUs and is a major limitation in our study.
In summary, our Harm Reduction program has been shown to decrease the spread of HIV among IDUs. Nevertheless, the proportion of recent infections in IDUs increased from 2008 to 2009. Therefore, to carry out an NSP thoroughly and continuously was important to decrease the further spread of HIV in IDUs. In addition, continuous ongoing monitoring of the molecular epidemiology of HIV can be useful to monitor the spread of HIV in order to establish and modify public health efforts to prevent new infections.
Footnotes
Acknowledgments
We thank Ms. Ying-Chen Lin of the HIV/AIDS Control and Study Center of National Taiwan University and Ms. Kuan-Lin Chen of the Taiwan Centers of Disease Control for their technical assistance. This research was supported by funds from the Taiwan Centers for Disease Control (DOH97-DC-2011, 98-0324-01-F-20 and DOH98-DC-2016). The first three authors contributed equally to this work.
Author Disclosure Statement
No competing financial interests exist.