
Abstract
Immigration from developing regions to Western countries has resulted in an increased rate of non-B subtypes in the HIV population. However, it is unclear whether these HIV variants remain confined to foreigners or are already spreading among natives. Since many immigrants come from regions in which hepatitis B virus (HBV) and hepatitis C virus (HCV) are endemic, HIV-hepatitis coinfection might be more frequent in newly diagnosed HIV persons. Herein, we report changes in the prevalence and distribution of HIV-1 subtypes in Madrid, Spain over the past 10 years as well as the rate of chronic HBV and HCV coinfection in 1854 newly diagnosed HIV-1 individuals. Overall 18.2% carried HIV-1 non-B subtypes, although the prevalence increased over time reaching a peak of 19.4% in the last period (2007–2010). The most common non-B variants were CRF02_AG (37%), G (12%), A (9.9%), and C (7.8%). In native Spaniards the rate of non-B subtypes increased from 1.5% in 2000–2002 to 7.2% in 2003–2006 and to 11.4% in 2007–2010 (p = 0.04). Chronic hepatitis B and C were found, respectively, in 4.2% and 8.3% of the study population. While the prevalence of chronic hepatitis B has remained fairly stable over time across distinct populations, the rate of chronic HCV infection has experienced a significant decline, mainly in native Spaniards as a result of a reduction in intravenous drug use. In summary, the prevalence of HIV-1 non-B subtypes is rising in newly diagnosed HIV-1 individuals in Spain, including the native population. In contrast, the rate of HBV coinfection remains unchanged and the rate of HCV coinfection has declined.
Introduction
H
The distribution of HIV-1 non-B subtypes, including CRFs and URFs, differs geographically and is continuously changing driven by factors such as immigration, travel/tourism, commerce, and military deployment. For many years subtype B has dominated the HIV-1 epidemic in Western Europe and North America, 6 and although it is still the predominant strain in these areas, other HIV-1 variants proportionally are on the rise. This is clearly recognized in European countries where the prevalence of non-B strains has been relatively high since the beginning of the epidemic. 7,8 In Spain, immigration from developing regions has resulted in an increased rate of non-B subtypes in the HIV population. 9 However, it is unclear whether these variants remain confined to foreigners or are already spreading among native Spaniards.
Besides being infected with HIV, immigrants from developing regions to Spain often come from areas in which chronic hepatitis B virus (HBV) and/or hepatitis C virus (HCV) are endemic. Taking into account that HIV and hepatitis viruses share the same transmission routes, coinfection is relatively common. Thus, an increased proportion of coinfection should be expected among newly diagnosed HIV individuals. This fact has important clinical implications, since liver disease associated with HBV or HCV progresses faster in subjects with HIV infection and the use of antiretroviral therapy is associated with more frequent hepatotoxic events in the coinfected population.
The aim of our study was to analyze the prevalence of HIV-1 non-B subtypes in newly diagnosed HIV-1 individuals over the past 10 years as well as trends in the rate of coinfection with hepatitis viruses in this population.
Materials and Methods
All individuals newly diagnosed with HIV-1 at several clinics in Madrid between January 2000 and February 2010 were identified. The presence of serum HIV-1 antibodies had been demonstrated using two different ELISA assays (AxSYM, Abbott, Madrid, Spain; and BIO-RAD, Marnes la Coquette, France). Reactive samples were confirmed using an HIV-1 viral lysate Western blot (New LAV BLOT I, BIO-RAD). Viral RNA was extracted from plasma samples using the QUIamp viral RNA mini extraction kit (Qiagen, Hamburg, Germany), following the manufacturer's instructions. The HIV pol region, including the complete protease and partial reverse transcriptase (codons 1–247 or 1–335) regions, were amplified using Trugene (Siemens, Barcelona, Spain) or ViroseqTM HIV-1 genotyping System (Celera Diagnostic, Alameda, CA).
The derived nucleotide pol sequences were assigned to distinct HIV-1 subtypes using two different tools. The first was the Stanford HIVDB
10
and another was a genotyping tool that uses a sliding window to generate multiple overlapping segments of a query sequence and its reference dataset.
11
All discordant sequences by both methods and the ones unclassified were evaluated using phylogenetic methods. For that purpose multiple alignments were performed using the Clustal W multiple-sequence alignment software, with a reference set from the Los Alamos HIV-1 database (
All subjects with available specimens were retrospectively further tested for HBV serum antigen (HBsAg) using a commercial enzyme immunoassay. Chronic hepatitis B was diagnosed in patients with positive serum HBsAg in the absence of anti-HBV core IgM. Likewise, all sera were tested for serum antibodies to HCV using a commercial ELISA, and reactive samples were further tested for serum HCV-RNA using a real-time PCR commercial method (Abbott) or Versant 3.0 bDNA assay (Siemens). Chronic hepatitis C was defined as positive serum HCV-RNA in anti-HCV reactive specimens.
Statistical methods
Comparisons of proportions were performed using the Chi-square or Fisher's exact tests, when appropriate. Comparisons of means were assessed using the Student's t test. Multiple logistic regressions were used to examine associations when some variables were considered as potential confounders. All reported p values were two-sided. The SPSS software version 15.0 (SPSS Inc., Chicago, IL) was used for all statistical analyses. Differences were considered to be significant when p values were <0.05.
Results
A total of 1854 newly diagnosed HIV-1 individuals were identified over the past 10 years at two large reference HIV clinics in Madrid, Spain. The main characteristics of the study population are recorded in Table 1. At the time of first HIV-1 diagnosis the median age was 35 years and 83.5% were male. Native Spaniards represented 54.7% of this population, with most of the rest from Latin America (27.8%) and sub-Saharan Africa (12.2%). Most individuals were men who have sex with men (MSM) (69.6%), with the remaining subjects infected through heterosexual contact (24.6%) or intravenous drug use (IDU) (5.5%).
HIV-1 subtype B was the most prevalent variant and overall the rate of non-B subtypes was 18.3%. The distribution was as follows: CRF02_AG (37%), G (12%), A (9.9%), C (7.8%), F (6.7%), CRF01_AE (4.6%), CRF12_BF (3.5%), and CRF14_BG (2.8%). There was an increase in the rate of non-B subtypes from 11.6% in the period 2000–2002 to 18.9% in the period 2007–2010 (p = 0.023). As expected, overall non-B subtypes were more prevalent in immigrants than in native Spaniards (33.6% vs. 7.9%; p < 0.001). Of note, the prevalence of immigrants among newly diagnosed HIV-1 individuals increased over time from 36.3% in 2000–2002 to 44% in 2003–2006 to 52.2% in 2007–2010 (p = 0.001). If the trend over time in HIV-1 non-B subtypes was considered by country of origin, a significant increase was seen across all different groups, except for sub-Saharan Africans in whom non-B subtypes always represented more than 75% of all infections (Fig. 1a).

Trends in the rate of
Chronic hepatitis B was overall recognized in 4.2% of patients. This rate has remained fairly stable over time, declining slightly from 5.9% in the period 2000–2002 to 4.1% in the period 2003–2006 and to 3.7% in the period 2007–2010 (p = 0.34). A nonsignificant reduction was seen in native Spaniards and Africans, which was in contrast with a slight increase among Latin Americans (Fig. 1b).
The overall prevalence of chronic hepatitis C was 8.3% and differed significantly according to transmission group (67.5% in intravenous drug users vs. 1.9% in men who had sex with men vs. 4.9% in heterosexuals) and geographic origin (Fig. 1c). Interestingly, HIV-HCV coinfection has experienced overall a significant decline among native Spaniards (from 16.8% in 2000–2002 to 2.2% in 2007–2010; p < 0.01) and Latin Americans (from 6.7% in 2000–2002 to 0.8% in 2007–2010; p = 0.014). This trend was not seen in Africans, in whom conversely HCV increased slightly during the study period.
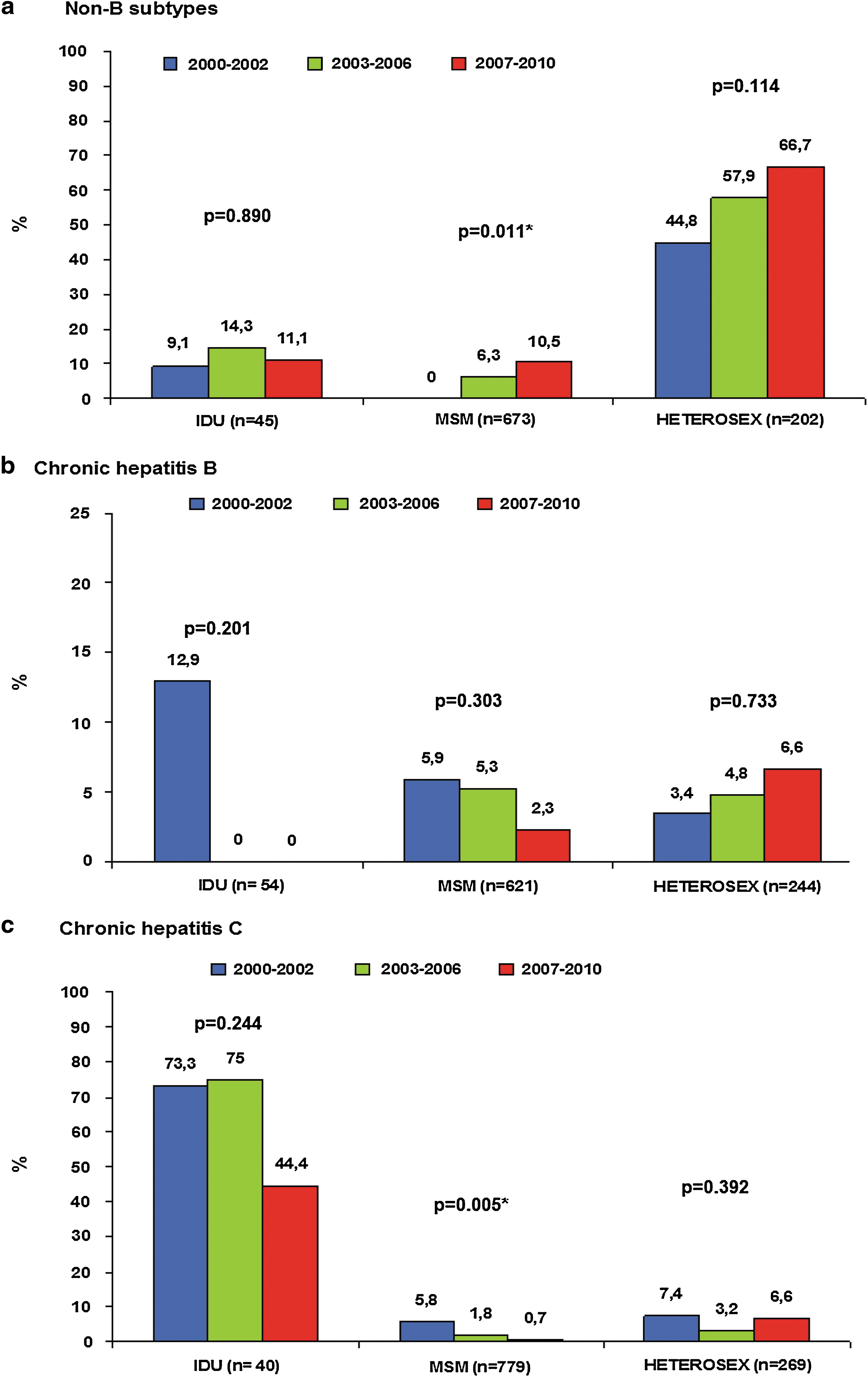
Figure 2 records the trends in non-B subtypes, chronic hepatitis B and chronic hepatitis C over the study period according to the transmission route category. HIV-1 non-B subtypes were by far the most prevalent in all study periods in persons infected by heterosexual contacts, although a trend toward increasing rates was seen over time. In MSM there was a significant increase in non-B subtypes, which represented more than 10% of the new HIV-1 infections after 2007. The rate of non-B subtypes remained fairly stable around 9–14% among IDUs (Fig. 2a). Chronic hepatitis B tended to decline in MSM and conversely tended to increase in persons infected by heterosexual contact, mainly reflecting the fact that implementation of HBV vaccination has mainly occurred among MSM, which was not the case in persons exposed to HIV-1 through heterosexual contacts (Fig. 2b). Finally, the rate of chronic hepatitis C has declined among newly HIV-1-infected IDUs and MSM, most likely reflecting a safer use of syringes. In persons infected by HIV-1 following heterosexual contact, the rate of chronic hepatitis C has remained low and fairly stable around 6% throughout the study period (Fig. 2c). In summary, it seems clear that there is a link between HIV-1 non-B subtypes and heterosexual contacts while HCV infection is associated with IDUs. Changes in the relative proportion of these routes of acquisition of HIV-1 infection over the study period, with an increase in infections due to heterosexual contacts and a decline in injecting drug use, largely seems to explain our overall findings.
Trends in the rate of
Discussion
The HIV-1 epidemic is characterized by an exceptional level of viral diversity and a fast rate of evolution. The dynamic distribution of subtypes and CRF/URFs reflects the complexity of the molecular epidemiology of HIV-1 infection worldwide. It has multiple implications as it may influence the performance of diagnostic tests used to detect and monitor the infection, modify pathogenesis and disease progression, impact the response to antiretroviral therapy, 13 including the development of drug resistance, 14 and complicate vaccine development. 15
In our study, the examination of newly diagnosed HIV-1 individuals in Madrid during the past decade shows that the proportion of non-B subtypes has increased significantly, currently representing nearly 20% of all new HIV-1 infections. It should be emphasized that this is not only due to recognition of infection in immigrants from sub-Saharan Africa or Latin America, as the rate of non-B subtypes has also increased among native Spaniards, who now represent 10% of infections. These results are in agreement with data from other surveys conducted in Spain. 9,16 Moreover, similar trends are seen in other neighboring European countries such as France. 17 Thus, at this time HIV subtyping must be recommended for all newly diagnosed HIV-1 individuals, including the native population. In contrast, this does not seem to be the case in the United States, as a recent large study has reported rates of infection with HIV-1 non-B subtypes of only 3.8% among newly diagnosed HIV-1 individuals, with subtype C being the most prevalent non-B variant. 18
Chronic hepatitis B currently affects 5–10% of individuals with HIV infection in developed countries, despite HBV vaccination being widely available and successful for preventing HBV infection. 19,20 The overall prevalence of serum HBsAg+ in our study population in Madrid was 4.3%, which seems slightly low but it is in agreement with recent figures from other Western European countries. 19 Moreover, our study shows that the prevalence of HIV-HBV coinfection has remained fairly stable over the past decade across all distinct geographic groups. Thus, HBV testing at the time of HIV-1 diagnosis should not be forgotten, as current antiviral therapy for HBV is very effective. 21
Coinfection with HCV has declined in native Spaniards and Latin Americans with newly diagnosed HIV-1 infection in Madrid, largely driven by a reduction in the proportion of subjects infected through intravenous drug use. In contrast, HCV coinfection has shown a slight increase among sub-Saharan Africans. Assuming a low transmission of HCV through sexual contact, the recognition of higher rates of HCV with age supports the view that unsterile injections and other iatrogenic routes of transmission most likely continue to be the main risk factor for HCV infection in Africa. While donated blood is universally tested for HCV in developed countries, this is still not the case in many African countries. Additionally, while injecting drug use is relatively rare in Africa, recent reports have indicated its use in large cities of Nigeria, Kenya, and South Africa. 22 Therefore the high rate of unsterile medical injections, both within and outside the health care system, may account for significant ongoing HCV transmission and serve as the bridge to the general population in Africa. The deleterious impact of chronic hepatitis C on HIV and vice versa is well established, 23 and the recognition of nearly 10% of coinfection in newly diagnosed HIV-1 sub-Saharan Africans in our study reinforces the belief that HCV testing must be performed in all HIV-1 persons at the time of first diagnosis.
In summary, the rate of non-B subtypes is increasing among newly diagnosed HIV-1 individuals in Spain, mainly driven by the large immigration flow, with recent spreading into the native population. In contrast, chronic hepatitis B remains fairly stable, below 5% in newly diagnosed HIV-1 persons, and chronic hepatitis C has declined significantly during the past decade, mainly due to a reduction in intravenous drug use among native Spaniards.
Footnotes
Acknowledgments
This work was supported in part by grants from FIS (CP06/0284 and PI06/1826), FIPSE (36742/08), Fundación Investigación y Educación en Sida (IES), Agencia Laín Entralgo, RIS (Red de Investigación en SIDA, ISCIII-RETIC RD06/006), and the European NEAT project.
Author Disclosure Statement
No competing financial interests exist.