
Abstract
Changes in body fat distribution in virologically suppressed HIV-infected patients switching from lopinavir/ritonavir (LPV/r) to atazanavir/ritonavir (ATV/r) were assessed. A prospective comparative study was conducted of 37 patients receiving LPV/r regimens switching to ATV/r with 46 patients continuing with LPV/r. Body composition was assessed with whole-body dual-energy x-ray absorptiometry (DXA). Abdominal CT scans were also performed in a subset of patients. Groups were comparable in baseline demographic, clinical, and anthropometric characteristics. After 12 months, peripheral fat did not change significantly, but an increase in trunk fat was observed only in the ATV/r group (0.87 kg, p = 0.021). The percentage of patients with an increase ≥20% in total fat was 37.8% and 15.2% in the ATV/r and LPV/r groups, respectively (p = 0.018). In the ATV/r group, the increase in trunk fat (9.4%) was significantly higher than in peripheral fat (3.7%) (p = 0.007), leading to a significant increase in fat mass ratio (3.76%, p = 0.028), whereas no significant differences were found among LPV/r patients. CT scans showed that abdominal fat increase corresponded to both visceral (28%, p = 0.008) and subcutaneous fat (42%, p = 0.008). These data suggest that switching from LPV/r to ATV/r is associated with increased trunk fat, both subcutaneous and visceral.
Introduction
H
While thymidine analogues have been strongly implicated in peripheral fat loss, lipoatrophy, 2 the factors involved in the pathogenesis of central fat accumulation are less clearly defined.
Lipodystrophy is a multifactorial syndrome and the exact cause remains elusive. Protease inhibitor (PI) therapy, however, has been implicated in its etiology. To varying degrees, the majority of PIs have been associated with the metabolic disturbances and/or morphological alterations that constitute the lipodystrophy syndrome. 3,4 Atazanavir (ATV), unboosted or boosted with ritonavir (ATV/r), seems less likely to cause dyslipidemia and other adverse metabolic effects compared with other PIs. 5 –9 These findings have been observed both in naive and in pretreated patients. 5 –10 Several studies switching from other PIs, including lopinavir/ritonavir (LPV/r) to ATV/r, have been previously conducted with the aim of simplifying therapy and improving tolerability and the lipid profile. 6,8,9 However, little information is available comparing body fat changes between patients receiving different PIs, and specifically, the effect of switching from LPV/r to ATV/r on changes in body composition remains unclear. 11,12
The objective of this study was to compare the impact on body fat distribution of switching from LPV/r to ATV/r in otherwise healthy virologically suppressed HIV-infected patients. Although a few studies conducted in different scenarios and comparing these two drugs in terms of changes in fat distribution have been presented, this is the first study to be published showing that ATV/r is associated with a greater increase in trunk fat and therefore it adds valuable data to the scant information available in the literature. 12 –14
Materials and Methods
This was a 12-month, prospective, open-label, comparative multicenter study of HIV-1-infected patients aged at least 18 years who switched from LPV/r to ATV/r or continued with the same therapy. Patients were recruited under conditions of daily practice at the HIV Units of five acute-care university-affiliated hospitals in Barcelona, Spain, with extensive experience in HIV management. Virologically suppressed HIV-infected patients who were stable on LPV/r-based regimens were eligible. The study was approved by the Ethics Committee at each center, and all patients gave written informed consent.
An elective switch from LPV/r (400/100 mg twice a day) to ATV/r (300/100 mg every day) was offered to 37 consecutive HIV-positive subjects aged ≥18 years with undetectable viral load (HIV-1 RNA levels <100 copies/ml) for reasons of therapy simplification, lipid disturbances, or other. Subsequently, another group of 46 patients receiving an LPV/r-based regimen, adjusted by age, sex, and weight, was consecutively offered to serve as controls.
Changes in body fat distribution assessed by dual-energy x-ray absorptiometry (DXA) scans were the primary outcome measure. Body composition was assessed at baseline and at 12 months. Whole-body DXA scans were performed using a Lunar DPX-L densitometer (Lunar Radiation Corporation, Madison, WI). Peripheral limb fat was the sum of arm and leg fat mass. Trunk, peripheral, and total fat (absolute and percentage changes) as well as the proportion of patients with ≥20% fat changes and fat mass ratio (defined according to Bonnet et al. 15 ) were evaluated. Clinical variables [demographics, risk transmission group, the clinical stage of HIV infection or AIDS, concurrent nucleoside analogue reverse transcriptase inhibitors (NRTIs) and nonnucleoside reverse transcriptase inhibitors (NNRTIs), use of lipid-lowering drugs, and use of hypoglycemic drugs], anthropometric data [weight, height, body mass index (BMI), waist, waist-to-hip ratio], and laboratory tests [CD4+ T cell lymphocytes, HIV-1 RNA levels, total serum cholesterol, triglycerides, very-low-density lipoprotein (VLDL) cholesterol, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, glucose, insulin, C-peptide, and insulin resistance (HOMA)] were obtained fasting and measured at baseline and at 12 months. Abdominal computed tomography (CT) scans were also performed in a subset of patients.
Between-group differences were analyzed with the Student's t test or the Mann–Whitney U test and within group differences with the paired t test or the Wilcoxon signed-rank test for normally and not normally distributed data, respectively. Categorical variables were compared with the chi-square (χ2) test. Correlation between DXA and CT results was assessed using the Pearson's correlation coefficient. Multivariate logistic regression analysis was used to estimate the best predictors of total fat increase ≥20%. Statistical significance was set at p < 0.05. Statistical analyses were conducted with SPSS, version 15.0 (Chicago, IL).
Results
A total of 83 virologically suppressed HIV-1-infected patients were evaluable; of these 37 switched from LPV/r to ATV/r and 46 continued on LPV/r-based regimens and were chosen as controls. Baseline clinical, laboratory, and DXA data in both study groups were comparable, except for the use of several nucleoside analogues (Table 1). The median trunk fat was 8.21 kg (range 1.44, 30.81) and the peripheral fat 4.87 kg (range 0.95, 25.66).
Data as median (range) unless otherwise stated.
DXA, duel-energy x-ray absorptiometry; ATV/r, atazanavir/ritonavir; LPV/r, lopinavir/ritonavir; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; LDL, low-density lipoprotein; HDL, high-density lipoprotein; VLDL, very low-density lipoprotein; HOMA, homeostatic model assessment.
Regarding lipid changes at 12 months, significant differences between arms were observed only in triglycerides (−24% ATV/r vs. −1.43% LPV/r, p = 0.004) and in VLDL (−24% in ATV/r and −1.08% in LPV/r, p = 0.04).
As shown in Table 2, after 12 months as compared with baseline, there was a statistically significant increase in median trunk fat [0.87 kg (range −6.9, 8.2), p = 0.021] and in median fat mass ratio [3.76% (range −19.3, 52.7), p = 0.028] in ATV/r patients, whereas these changes in the LPV/r group were not statistically significant. Changes in peripheral fat were not significant in any of the two groups. The increase in total fat almost reached statistical significance in the ATV/r group only (Table 2). As shown in Fig. 1, in the ATV/r group, the increase in trunk fat was significantly higher than the increase in peripheral fat [9.4% (range −53.2, 167.3) vs. 3.7% (range −49.9, 122.1), p = 0.007]. In the LPV/r group, trunk and peripheral fat increases were not significantly different [4.3% (range −54.8, 89.6) vs. 2.5% (range −42.7, 83.1), p = 0.223].
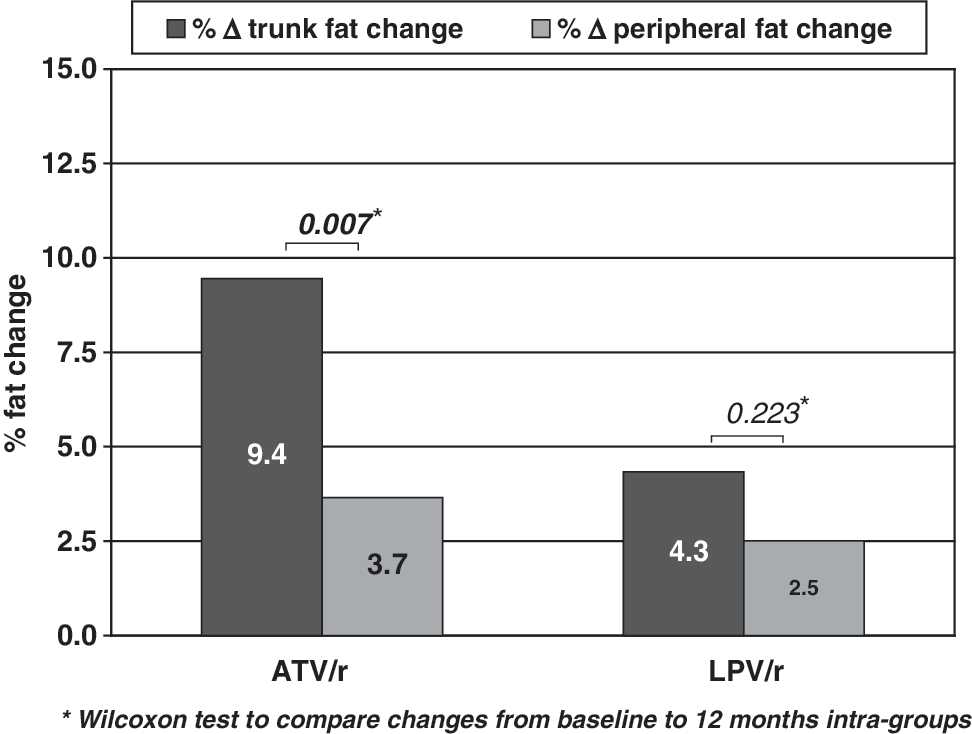
Changes in peripheral and trunk fat according to treatment.
DXA, duel-energy x-ray absorptiometry; ATV/r, atazanavir/ritonavir; LPV/r, lopinavir/ritonavir.
No differences were found between groups in the percentage of patients with a decrease ≥20% in peripheral fat or in the percentage of patients with an increase ≥20% in trunk fat, although the percentage of patients with an increase in total fat ≥20% was 37.8% in the ATV/r group and 15.2% in the LPV/r group (p = 0.018). Increases in trunk fat ≥20% were associated with significant weight and BMI increases in both ATV/r and LPV/r groups as well as with waist and waist-to-hip increases in the ATV/r group (p < 0.05 for all comparisons). However, increases in trunk fat ≥20% were not associated with significant changes in the lipid parameters in ATV/r patients.
Abdominal CT scans were available for 21 patients (ATV/r, n = 13; LPV/r, n = 8). Body fat changes in trunk fat at 12 months as compared with baseline detected by CT and DXA correlated significantly (abdominal fat, r = 0.914, p < 0.001; subcutaneous fat, r = 0.683, p < 0.001; visceral fat, r = 0.843, p < 0.001). Moreover, in eight patients with trunk fat increases ≥20% in whom CT scans were performed, significant increases (p = 0.008) in abdominal fat (32.7%), visceral fat (27.5%), and subcutaneous fat (42.3%) were observed.
In the logistic regression analysis, after excluding BMI and weight, ATV/r was associated with a total fat increase ≥20% (OR = 3.39, 95% CI 1.19, 9.62). No differences were observed in trunk or total fat increase according to the use of thymidine analogues (data not shown). Also, no relationship was found between trunk or total fat increase and lipid or glucose changes at 12 months (data not shown).
Discussion
This prospective study suggests that in patients with virological suppression, a switch from LPV/r to ATV/r increased trunk fat as shown by DXA, and that this increase occurred at the expense of both subcutaneous and visceral fat, according to CT data. In addition, simple anthropometric measurements, such as weight, BMI, and waist circumference, correlated well with DXA findings.
Interestingly, in three other studies, two performed in antiretroviral-naive adult patients and one in stable pretreated patients, ATV/r use was also associated with an increase in abdominal fat and/or an increase in trunk-to-limb ratio. 12 –14 In a substudy of the CASTLE study, which compared ATV/r with LPV/r in 224 patients, the subgroup of patients with low BMI presented a significant increase in both visceral and subcutaneous abdominal fat as measured by DXA, compared with LPV/r patients, as well as a significant increase in the change of the trunk-to-limb fat ratio at week 96. 13 In the BASIC study, comparing ATV/r with SQV/r in 120 patients, again ATV/r use was associated with a significant increase in visceral fat, and in this case, also with an increase in limb fat. 14 In the REAL study, performed in 201 virologically suppressed patients randomly assigned to continue with LPV/r or to switch to ATV/r, a significant increase in trunk-to-limb ratio was observed only in ATV/r patients (2.6% increase in trunk fat, 0.9% in limb fat, difference p = 0.02) after 48 weeks. 12
Conversely, in a small randomized study enrolling only 15 patients (8 vs. 7), the switch from LPV/r to ATV/r was associated with a reduction in visceral fat and an increase in glucose uptake by muscle. 16
Although ATV/r patients had a significant improvement compared to LPV/r patients in some lipid parameters, as observed in other studies, 6,7 we did not find any correlation between metabolic changes and fat increase. Thus, the mechanism of this possible association between ATV/r and abdominal fat increase as well as its clinical relevance remain unclear.
One of the main obstacles for good management of lipodystrophy is a lack of a standard definition of this for HIV-associated complications. It has been suggested that fat mass ratio (FMR) may help in diagnosing lipodystrophy. 15,17 –19 In this study, FMR significantly increased in the ATV/r arm due to a greater increase in abdominal fat than in peripheral fat. The value of prospectively assessing fat mass ratio changes in patients receiving antiretroviral therapy to prevent the development or progression of abnormal fat redistribution is unknown at present but should be studied further.
Our data should be interpreted with caution due to the limitations of the study, in particular the nonrandomized design, the relative small number of patients, and the fact that CT scans were available for only less than half of the study patients. However, groups were well balanced in most baseline characteristics, and no correlation was found between the use of thymidine analogues—the only relevant baseline characteristic not well balanced between both groups of patients—and fat increase. In addition, despite the small sample size, several statistically significant findings were observed both with DXA and CT scan assessment.
Finally, our results suggest that an ATV/r-based regimen as a simplification strategy does not have a favorable impact on body fat redistribution in treatment-experienced HIV-infected patients when compared with those maintaining an LPV/r-based regimen. Moreover, findings regarding increases in visceral fat in those patients switched to ATV/r deserve further study.
Footnotes
Acknowledgments
We thank Marta Pulido, M.D., for editing the manuscript and for editorial assistance. Presented in part as a poster at the 12th European AIDS Conference/EACS, in Cologne, Germany, on November 11–14, 2009.
Author Disclosure Statement
E.F., E.M., P.D., E.R., E.N., M.S., J.M.G., and D.P. have received research grants and/or honoraria for advisories and/or conferences from several pharmaceutical company manufacturers of antiretroviral drugs, including Abbott and BMS.