
Abstract
HIV subtype characterization is an important tool to monitor the genetic variation of the HIV epidemic. This study investigated the current HIV subtype distribution and recombination among the northern Thai population. An in-house genotypic assay of HIV protease and reverse transcriptase genes was performed on 420 plasma specimens from HIV-infected patients residing in several northern Thai provinces. HIV subtyping was determined by phylogenetic analysis. Three hundred and ninety-eight sequences (94.8%) were identified as CRF01_AE with the genetic distance of 1.848±0.957% and 12 (2.9%) as subtype B with the genetic distance of 4.186±0.849%. In addition, two sequences (0.5%) of HIV subtype C were found, suggesting that these patients were either immigrants from another country or were infected through heterosexual contact with HIV-infected subjects from another country. Bootscan analysis showed that there were eight (1.9%) unique recombinant forms (URFs) consisting of a recombinant of CRF01_AE with subtype B or subtype C. The information from this study is useful for prevention programs to halt the onward transmission of a particular HIV outbreak. However, characterization of the full genome of these CRF01_AE/B and CRF01_AE/C intersubtype recombinants, and also subtype C, is required for confirmation and elucidation.
Introduction
A
Three phylogenetic groups of HIV-1 have been recognized, namely, major (M), outlier (O), and non-M, non-O (N). Most HIV-1 infections are caused by group M viruses, which are subdivided into nine genetic subtypes (subtypes A, B, C, D, F, G, H, J, and K) and more than 48 intersubtype recombinants known as circulating recombinant forms or CRFs [
The pandemic of AIDS can be seen as several epidemics of separate subtypes. The major factor in its spread is sexual transmission. 5 In Thailand, it was found that transmission of HIV is primarily through heterosexual contact, and the major subtype is CRF01_AE. During the first HIV epidemic, intravenous drug users (IDUs) were commonly infected with HIV subtype B, similar to those homosexuals and IDUs in western countries. 6,7 However, the HIV epidemic in Thailand has changed in the past several years. CRF01_AE now accounts for the majority of new infections in both risk groups (heterosexuals and IDUs). In addition, an increasing number of CRF01_AE/B recombinants have been documented. 8,9 The epidemiology of HIV is constantly changing, possibly from viral evolution, resulting from the high mutation rate of reverse transcriptase, high viral turnover, viral genomic recombination, as well as immune and therapeutic selection pressures. Other factors that can influence the global distribution and prevalence of HIV subtypes include human travel and migration and human genetics. The regional distribution of subtypes and recombinant forms is subjected to rapid shifts, both through newly generated strains and the introduction of established strains to new populations, countries, and regions. The aim of this study was to investigate the current HIV subtypes and CRF distribution among the Northern Thai population.
Materials and Methods
The study was conducted among the HIV cohort at Chiang Mai University Hospital, Chiang Mai, Thailand, a 1800-bed tertiary-care and referral hospital serving the northern part of the country with a catchment population of 5.7 million people or 9.0% of the population of Thailand, from July 2007 to March 2010. Ethical clearance of this study was obtained from the Human Ethics Committee of the Faculty of Medicine, Chiang Mai University (ethics certificate of approval number: 215/2010).
A total of 420 clinical specimens from consecutive HIV-infected patients residing in several provinces throughout Northern Thailand who visited the HIV Clinic during the study period were collected and tested using an in-house genotypic assay of HIV protease (PR) and reverse transcriptase (RT) genes. This in-house HIV-1 genotyping method is part of the external quality assurance (EQA) of the Thailand National Institute of Health (NIH) and the Treat Asia Quality Assessment Scheme (TAQAS) of the Australian National Serology Reference Laboratory (NRL). 10
Extraction, polymerase chain reaction and sequencing
The pol-PR and pol-RT gene were used as the templates in the amplification reaction. The primers covered the whole protease gene (PR, 1–99 amino acid base sequence) and part of the reverse transcriptase gene (RT, 1–260 amino acid base sequence). The viral RNA was extracted from 150 μl of individual plasma sample using a NucleoSpin Viral Isolation kit (Macherey-Nagel, Germany). The single-stranded HIV-1 RNA was reverse transcribed and concurrently amplified by the one-step RT-polymerase chain reaction (PCR) technique using Superscript III one step RT-PCR with platinum Taq (Invitrogen, USA). The primer pairs used for the PR gene were the DRPRO5, 5′-AGACAGGYTAATTTTTTAGGGA-3′ and DRPRO2L, 5′-TATGGATTTTCAGGCCCAATTTTTGA-3′; those used for the RT gene were DRRT1L, 5′-ATGATAGGGGGAATTGGAGGTTT-3′ and DRRT4L, 5′-TACTTCTGTTAGTGCTTTGGTTCC-3′. 11 –13 After reverse transcription and the amplification step, double-stranded DNA was amplified by nested PCR using a KOD polymerase kit (Toyobo, Japan). Primers, DRPRO1M, 5′-AGAGCCAACAGCCCCACCAG-3′ and DRPRO6, 5′-ACTTTTGGGCCATCCATTCC-3′ were used for the PR gene, whereas primers DRRT6L, 5′-TAATCCCTGCATAAATCTGACTTGC-3′ and DRRT7L, 5′-GACCTACACCTGTCAACATAATTGG-3′ were used for RT gene.
The purified DNA was analyzed for its nucleotide sequences using an ABI Prism 3100 Genetic Analyzer (Applied Biosystems, USA).
Analysis of sequences
The nucleotide sequences of 420 plasma samples were obtained and edited using SeqScape software V2.6 (Applied Biosystems, USA) and compared to the HIV reference sequence strain HXB2. The edited sequences were interpreted for HIV subtype using the REGA HIV-1 automated subtyping tool version 2.0.
14
The pol-PR and pol-RT (1050 bp) sequences obtained also were aligned. Multiple sequence alignments were performed with CLUSTAL X, version 2.0.10 software.
15
The results were used for phylogenetic analysis after artificial adjustment. Putative parental strains of different subtypes and CRFs were downloaded from the Los Alamos HIV Database for phylogenetic and bootscan analysis [
Analysis of recombination
Using the BootScan method, pol gene sequences were reanalyzed by SimPlot, version 3.5.1 to identify recombination breakpoints in samples with undetermined subtypes or CRFs. 18 HIV-1 B subtype isolate B.TH.90.BK132.AY173951, CRF01_AE isolate CRF01_AE.TH.90.CM240.U54771, and C subtype isolate C.95IN.95IN21068, which were selected as putative parental strains, with D subtype isolate 01CM-01CM_4412HAL, F1 subsubtype isolate 93BE-V1850, G subtype isolate 96BE-DRCBL, H subtype isolate 93BE-V1991, J subtype isolate 97CD-J-97DC-KTB147, and K subtype isolate 97CD-EQTB11C as background strains. The bootstrap values were plotted for a window of 200 base pairs (bp) and moved in increments of 20 bp along the alignment.
Results
General characteristics of the 420 plasma specimens
These samples were collected from 420 HIV-infected patients; 236 (56.2%) were male, 183 (43.6%) female, and 1 (0.2%) transgender. The average age was 37.8 years (range 20–73 years). Modes of transmission were heterosexual, homosexual, intravenous drug use, and unknown in 350 patients (83.3%), 54 (12.9%), 11 (2.6%), and 5 (1.2%), respectively. One hundred and twelve patients (27.2%), 66 (15.7%), and 242 (57.1%) were asymptomatic, symptomatic HIV infected, and AIDS cases, respectively. Two hundred and ninety-five patients (70.2%) were antiretroviral treatment naive, and the remaining were cases with antiretroviral treatment failure. All of the treatment-naive patients with CD4 cell ≤200 cells/mm3 were eligible for antiretroviral therapy and were tested before initiation of treatment.
Analysis of HIV-1 subtype by REGA HIV-1 subtyping tool
From 420 plasma specimens, 398 samples (94.8%) were CRF01_AE with 99.79±0.57% support, 11 (2.6%) subtype B with 99.45±1.51% support, and 2 (0.5%) subtype C with 100% support. Nine of the 420 samples could not be subtyped. The HIV subtype analysis by the REGA HIV-1 subtyping tool is shown in Table 1.
SD, standard deviation.
Phylogenetic tree and genetic distance analysis
Analysis of the HIV subtype by phylogenetic tree is shown in Fig. 1, and the analysis of genetic distances in Table 1. Eight of the 420 sequences (1.9%) were undetermined subtypes or CRFs. It was evident from the phylogenetic tree that 398 CRF01_AE sequences (94.8%) were clustered together with subtype CRF01_AE.TH.90.CM240.U54771 (Fig. 1). In comparison with the sequence of respective international strains, CRF01_AE.TH.90.CM240.U54771 shared the genetic distance of (1.848±0.957)% with 93% bootstrap support. Twelve HIV subtype B sequences (2.9%) were clustered together with subtype B.TH.90.BK132.AY173951. In comparison with the sequence of respective international strains, B.TH.90.BK132.AY173951, the genetic distance was (4.186±0.849)% supported by 97% bootstrap value. Two subtype C sequences (0.5%) were clustered together with subtype C.95IN.95IN21068 and shared the genetic distance of (3.9512±2.355)%, which was supported by a 100% bootstrap value.
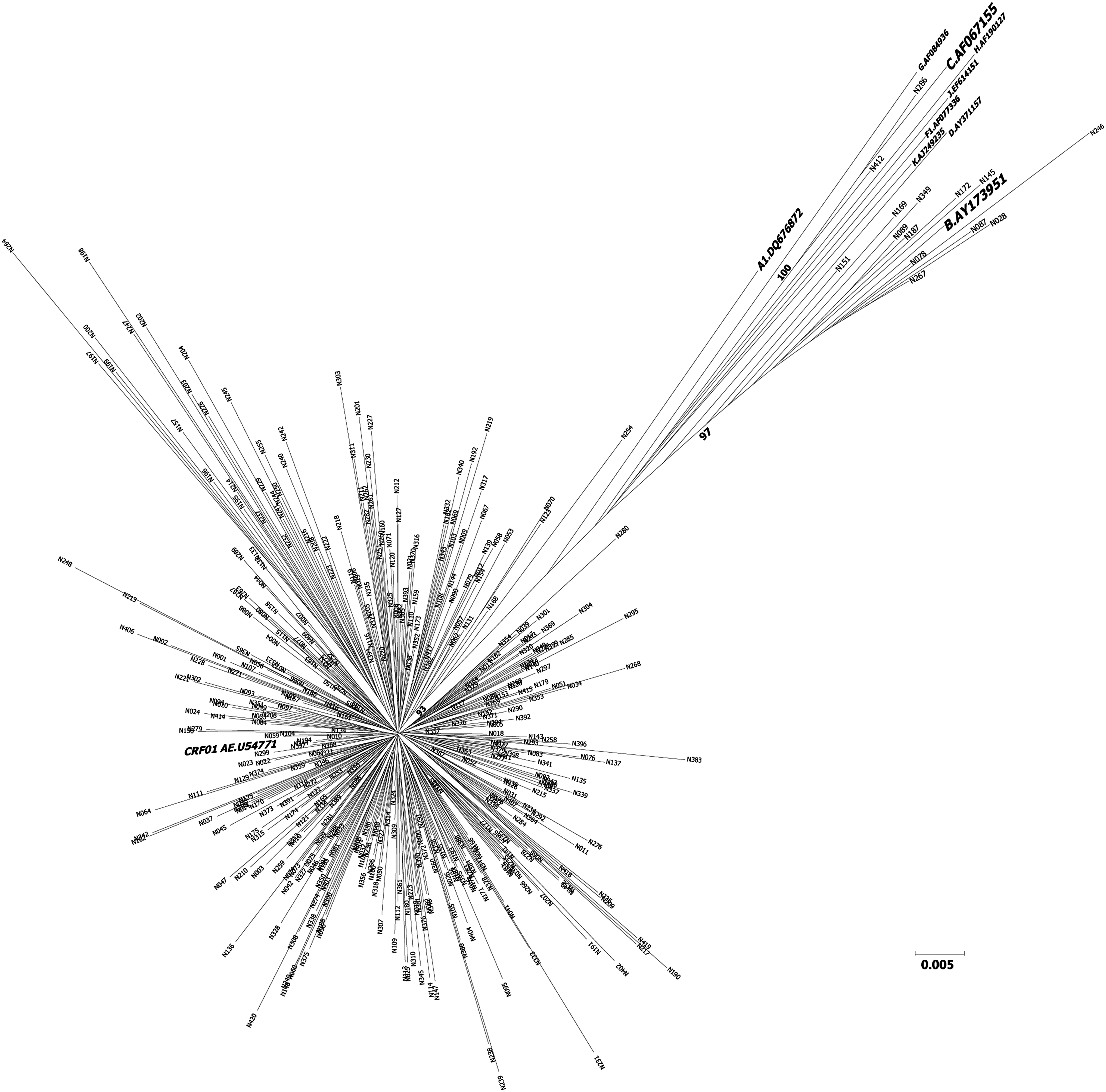
Phylogenetic analysis of the HIV-1 pol-PR and pol-RT region.
Analysis of recombination
Eight unclassified samples from pol-PR and pol-RT genes were subjected to bootscan analysis by SimPlot. Among these eight patients, six were male and two were female. Modes of transmission were homosexual, heterosexual, and intravenous drug use in five, two, and one patient, respectively. Bootscanning plots revealed that all eight samples had a unique recombination profile in the pol-PR and pol-RT genes. Seven samples (N006, N030, N118, N256, N270, N367, and N377) were intersubtype recombinants of HIV-1 CRF01_AE and subtype B. One sample (N130) was identified as an intersubtype recombinant of HIV-1 CRF01_AE and subtype C (Fig. 2).

Bootscanning plots of the pol-PR and pol-RT gene sequences of HIV-1 isolates to identify the new recombination with the reference sequences. The X axis indicates the nucleotide positions along the alignment and the Y axis indicates the percentage of bootstrap replicates supporting the clustering with the reference strains. Samples are N006
Discussion
The HIV molecular epidemiology in Northern Thailand was investigated among a total of 420 plasma samples in this study. These specimens were from patients from provinces in Northern Thailand served by Chiang Mai University Hospital, the only tertiary-care university hospital in the region. The demographic data of these 420 patients (age, sex, exposure category) were similar to those of 80,985 northern Thai patients reported to the Ministry of Public Health in 2009. The overall results suggested that HIV-1 CRF01_AE is still largely predominant, followed by HIV subtype B, in the HIV epidemic in Northern Thailand. These results confirmed the finding of previous survey studies in Thailand. 6,19,20
A single subtype or CRF of HIV usually dominates the epidemic in a particular geographic area. In many regions, however, several subtypes cocirculate, and intersubtype recombinants are detected among them, mainly as unique recombinant forms (URFs). 21 –24 An increasing number of CRF01_AE/B recombinants has been documented, constituting 15% of the strains in IDUs in the northern province of Chiang Mai. 9 Even though the majority of these recombinants were URFs, similar findings were reported in Malaysia, where 20% of partial genome sequences were CRF01_AE/B recombinants. 8 In this study, there were eight URFs consisting of CRF01_AE recombined with subtype B or C. By phylogenetic analysis, sample N270 appeared to be closely related to CRF33_01B and sample N118 to CRF15_01B with 100% bootstrap support.
Another interesting observation was the presence of HIV subtype C in two patients. Both patients acquired HIV from heterosexual contact. One patient was an immigrant from China and the other was a spouse of an HIV-infected subject from another country. This finding suggests that the infection with HIV subtype C originated from outside the country. The CRF01_AE/subtype C recombinant has also been detected in Thailand in another study. 9,25 The emergence of newer strains in Northern Thailand as well as selected recombinant forms was likely due to infected immigrant populations, who were from areas with a high prevalence of other HIV subtypes.
The genetic diversity of HIV may have an impact on viral determination. 26,27 However, the quantitative HIV-1 assays have been regularly updated to improve their ability to detect various HIV-1 subtypes. 27 The impact of genetic diversity on the performance and interpretation of genotypic drug resistance assays has been demonstrated by several studies. 26,28,29 It may be essential to learn the distribution of HIV subtypes within a treatment population in order to better interpret the results of antiretroviral drug sensitivity. 30,31
In conclusion, the investigation of HIV molecular epidemiology suggests that HIV CRF01_AE was predominant in Northern Thailand. HIV subtype C was also found. There were also URFs consisting of recombinant CRF01_AE with subtype B or C.
Footnotes
Acknowledgments
The authors are indebted to the patients who participated in the study. We wish to thank the National Research University Project under Thailand's Office of the Higher Education Commission and the Graduate School, Chiang Mai University for financial support. Ethical approval: This study was conducted in accordance with the ethical standards of the Ethic Committee at the Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand.
Author Disclosure Statement
No competing financial interests exist.