
Abstract
The emergence of resistance-associated mutations to the antiretroviral agents and the genetic variability of HIV-1 impose challenges to therapeutic success. We report the results of genotype testing assays performed between 2002 and 2006 in 240 antiretroviral-experienced patients followed up in an HIV reference center in Brazil. Drug resistance mutations and viral subtypes were assessed through the algorithms from the Brazilian Genotyping Network (RENAGENO—Brazil) and from Stanford University. Mutation 184VI was the most prevalent (70%) and the thymidine analogue mutations that appeared most frequently were 215FY, 41L, 67N, and 210W, in this order. Among nonnucleoside reverse transcriptase inhibitor mutations, 103NS (32.5%) stood out. HIV subtype B was identified in 184 patients (76.7%). A significant increasing trend in the prevalence of non-B subtypes was observed during the study period (p=0.004). The main differences in prevalence of mutations among HIV-1 subtypes were related to viral protease, with 20MRI, 36I, and 89IMT more prevalent among non-B subtypes, and 84V, 10FR, 63P, 71LTV, and 77I more common in subtype B (p<0.05). Most mutations to etravirine had a prevalence lower than 10%, but at least one mutation to this drug was observed in 45% of the patients. In only 11 patients (4.6%) three mutations to etravirine were verified. Regional surveillance of the resistance profile and HIV-1 subtypes is crucial in the context of public health, to prevent the transmission of resistant strains and to guide the introduction of new drugs in a specific population.
Introduction
W
In 2001, the Brazilian Genotyping Network (RENAGENO) 3 was established with the main objective of providing clinicians with decision-making tools to guide therapeutic rescue of antiretroviral-experienced patients. RENAGENO is also a national network that monitors the prevalence of viral drug resistance and HIV-1 genetic variability across Brazilian states. Our service is a member of this program. In this study, we sought to analyze the prevalence of antiretroviral drug resistance mutations by HIV-1 subtypes B and non-B in patients failing antiretroviral therapy for whom information related to previous antiretroviral exposure was available and who had a genotype testing assay between 2002 and 2006 at a HIV reference center in Minas Gerais, Brazil.
Material and Methods
In this study, we analyze the results of genotype testing assays performed between January 2002 and December 2006 on HIV-infected patients aged 18 years or older in instances of failing HAART, followed at the Training and Reference Center for Infectious and Parasitic Diseases (CTR/DIP) of Belo Horizonte, Brazil. CTR/DIP is a public institution maintained by the Belo Horizonte Health Secretary and is affiliated with the University Hospital of Minas Gerais Federal University. It is the largest outpatient service providing care for HIV-infected patients in the State of Minas Gerais, in the southeastern region of Brazil.
During this period, 388 genotype testing assays were performed in this service. Eighty-four tests were excluded because the genotyping system (see below) generated sequence reads in the .fasta and .gt files that were improper for the identification of resistance-associated mutations or for the determination of viral subtype. Fifty-two further cases were excluded because of missing data on previous antiretroviral exposure in the medical charts. To maintain the independence of observations, only first-time genotype testing assay results were analyzed; subsequent assay results from the same patient, which represented 12 cases, were excluded. Overall, 240 reports were analyzed.
The ViroSeqTM HIV-1 Genotyping System (Celera Diagnostic, Abbott Laboratories) was used for the identification of resistance-associated mutations in the HIV-1 polymerase (pol) gene according to the instructions of the manufacturer. All sequences obtained from samples were subjected to quality control assessments using the Blast-RENAGENO resistance analysis program (
The HIV-1 subtyping was based on pol gene sequences (the 297 nucleotides of protease and the first 1003 nucleotides from reverse transcriptase). The sequences were submitted to the rapid HIV subtyping tools of RENAGENO (
The amino acid sequences of the reverse transcriptase (positions 1 to 335) and protease (positions 1 to 99) genes were deduced from the nucleic acid sequences and compared to a subtype B consensus sequence from the Stanford HIV reverse transcriptase as well as protease sequence database (
Categorical variables were described according to their absolute and relative frequencies. Continuous variables were described through measures of central tendency and dispersion more appropriate for data distribution. Normality was tested by means of Shapiro–Wilk and Kolmorogov–Smirnov tests, as well as visual inspection of density histograms. Univariate association between categorical variables of independent groups was tested using Pearson's chi-square (χ2) or Fisher's exact test, as appropriate. Secular trend in prevalence of viral subtypes was assessed using the χ2 for linear trend. Statistical significance was set at α=0.05 (two-sided). All analyses were conducted using SPSS for Windows (version 15.0, SPSS Inc., Chicago, IL).
This study was approved by the Federal University of Minas Gerais Research Ethics Committee. Written informed consent was waived.
Results
We analyzed first-time genotype testing assays of 240 patients who met the inclusion criteria. Most (n=140, 58.3%) were born at the Minas Gerais hinterland. The median age at the time of the genotype testing assay was 39 years (percentile 25–75=34–46), and most patients were male (n=168, 70%), with a ratio of men to women of 2.2:1.
Frequency and length of antiretroviral use within each class before genotyping are shown in Table 1. Sixteen patients (6.7%) were exposed to zidovudine (AZT) monotherapy in the early 1990s, with a median length of use of 18 months (percentile 25–75=9.3–24.8). Ninety-five patients (39.6%) used dual therapy [most often with AZT and didanosine (DDI)] for a median of 19 months (percentile 25–75=9–31). One hundred and seventy-six patients (73.3%) received unboosted PI-based therapy, with a median length of use of 34 months (percentile 25–75=20.3–55.5 months). In this cohort, no patient made use of emtricitabine, etravirine, delavirdine, or unboosted fosamprenavir.
-r=ritonavir boosting.
Subtype B was identified in 184 patients (76.7%) and non-B subtypes in 56 patients (23.3%). Non-B subtypes comprised 35 cases (14.6%) of subtype F1, 20 (8.3%) of recombinant B/F1, and 1 case (0.4%) of subtype A1. Over the years, there was a significant increase in the prevalence of non-B subtypes (p=0.004) as illustrated in Fig. 1.

Secular trends in prevalence of subtype B and subtype non-B among HIV-1 isolates.
Among resistance mutations of reverse transcriptase, 184VI was the most prevalent (70%), followed by clinically relevant thymidine analogue mutations (TAM) [215FY (60.1%), 41L (45.3%), 67N (41.6%), and 210W (30.9%)] and 103NS (32.5%). The 151M complex, associated with multiresistance to NRTIs, was present in 3.3% of viral isolates. In 45% of patients, at least one specific mutation for etravirine was present but, except for 190AE (with 12.8% prevalence), all other mutations showed prevalences lower than 10%. Three mutations for etravirine were verified in only 11 patients (4.6%) and no patient had more than three mutations associated with this drug. Regarding major resistance mutations of viral protease, 90M (28%) and 54VALMT (25.5%) were the most prevalent.
Figures 2 to 5 show the prevalence of each resistance mutation to NRTIs, NNRTIs, and PIs by HIV-1 viral subtype B or non-B.
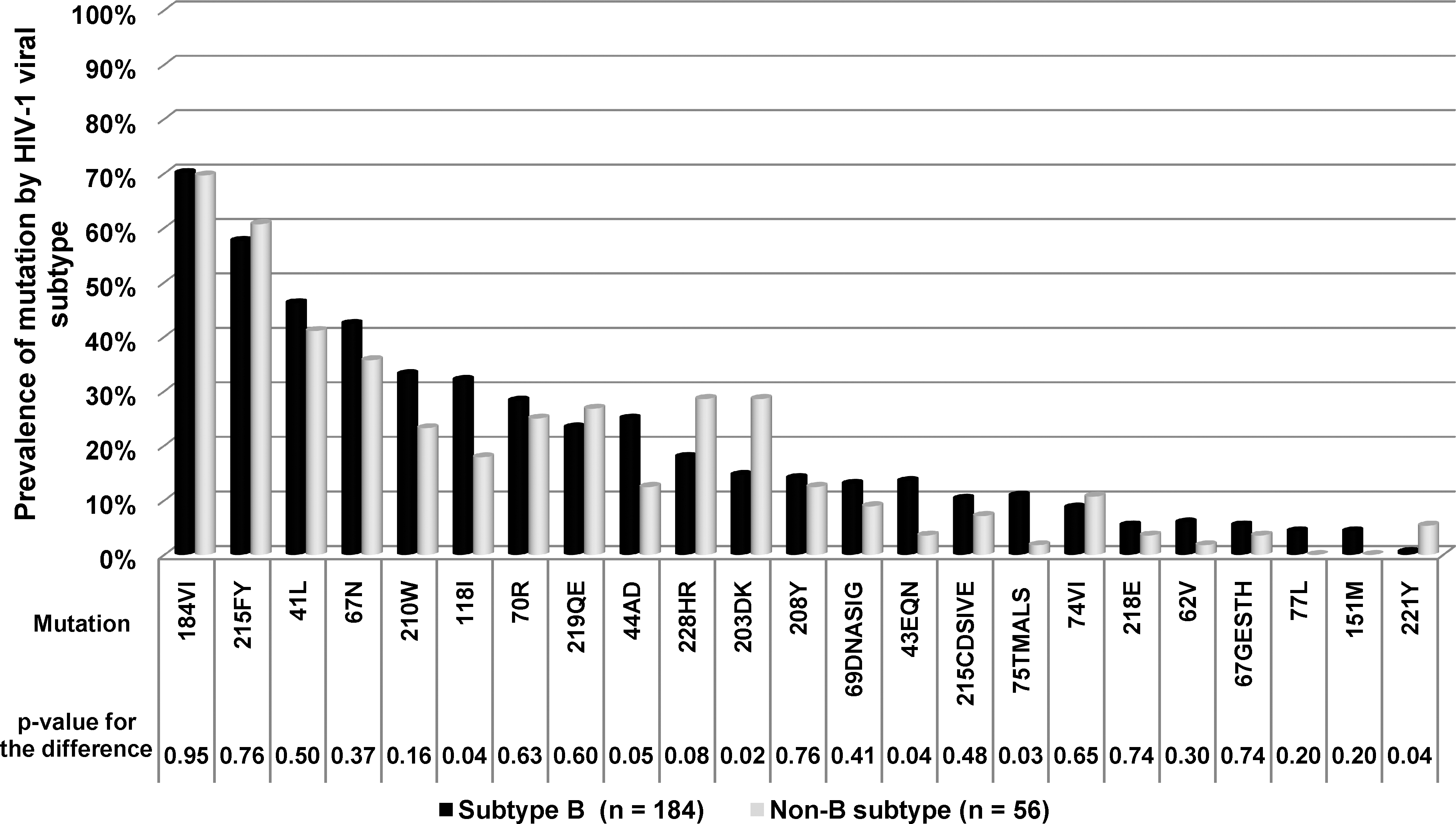
Prevalence of resistance-associated mutations to the nucleoside reverse transcriptase inhibitors by HIV-1 viral subtype.
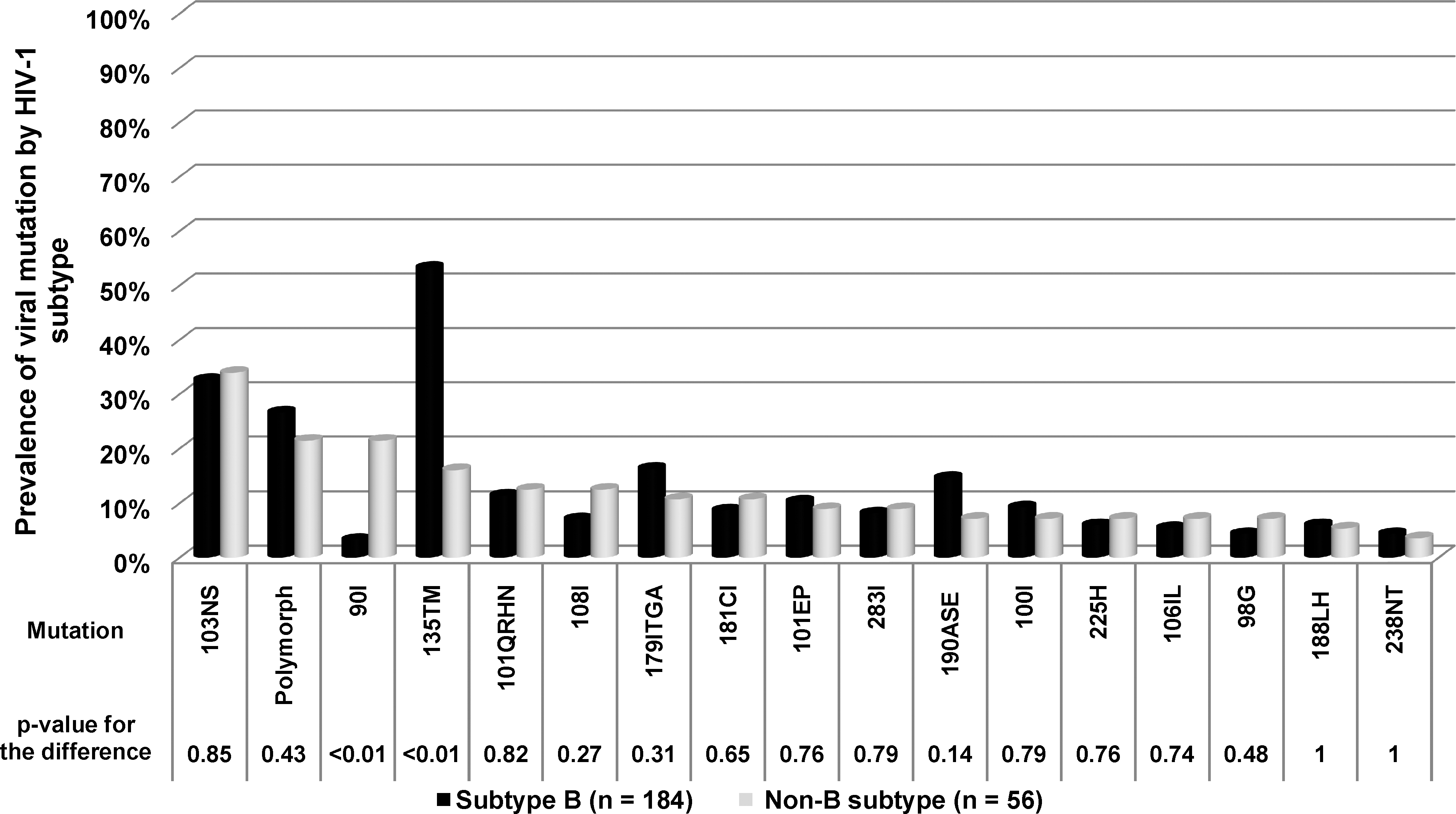
Prevalence of resistance-associated mutations to the nonnucleoside reverse transcriptase inhibitors by HIV-1 viral subtype.

Prevalence of major resistance-associated mutations to the protease inhibitors by HIV-1 viral subtype.

Prevalence of secondary resistance-associated mutations to the protease inhibitors by HIV-1 viral subtype.
Among the NRTI resistance-associated mutations, 203DK and 221Y were more frequently observed in non-B subtype virus; in contrast, 118I, 44AD, 43EQN, and 75TMA were more prevalent in subtype B virus (Fig. 2).
For NNRTI resistance-associated mutations, significant differences in prevalence were confined to 90I and 135TM (Fig. 3). While the former showed a negative association with subtype B when compared to non-B subtypes (OR=0.12, 95% CI=0.04–0.38), 135TM was more common in subtype B virus (OR=5.95, 95% CI=2.76–12.85).
In relation to major resistance mutations of viral protease (Fig. 4), only that of codon 84 showed a statistically significant difference in prevalence among HIV-1 subtypes, being more frequently observed in subtype B (OR=7.09, 95% CI=1.08–298.2). Among secondary resistance mutations of viral protease (Fig. 5), mutations in codons 20MIRTLV, 36ILVTA, and 89IMT were more prevalent among non-B subtypes, while 10FR, 63P, 71ILTV, and 77I were more common in subtype B virus. A high prevalence of polymorphisms was observed in the protease gene of both subtypes, being 98.2% for non-B subtypes and 83.2% for subtype B (p=0.004).
Discussion
184VI was the most prevalent mutation found in several studies published in Brazil and abroad. 4 –8 Although the 184VI mutation confers high-level resistance to lamivudine, it plays an important role when planning salvage regimens, as it reduces viral fitness and increases virus sensitivity to AZT, stavudine, and tenofovir. Its impact is modest on abacavir and DDI activity, but when associated with the 74V mutation, present in 10% of the cases in our study, it causes a high level of resistance to these antiretroviral drugs as well. 5 The high prevalence of 74V in this sample is probably due to the previous use of dual therapy with AZT and DDI in some patients.
The most prevalent TAMs were, respectively, 215FY, 41L, 67N, and 210W, while 70R and 219QE appeared less frequently. This distribution of TAM prevalence is similar to previous reports. 6,9 The presence of the 151M complex in 3.3% of patients in this cohort is remarkable considering that this mutation is rarely observed in genotyping reports, as it affects the capacity of the virus to replicate, becoming a minority population less likely to be amplified in the test. 5
Among resistance mutations to NNRTIs, the high prevalence of 103NS (32.5% of the cases) is noticeable, almost 3-fold higher than other clinically relevant mutations within the same class: 190ASE, 101EP, 181CI, 100I, and 108I, all with a prevalence of about 10%. This pattern of mutations to the NNRTI class is similar to other reports from several countries and in populations with different epidemiological peculiarities. 6 –10 Most mutations to etravirine had a prevalence of lower than 10%, but at least one mutation to this drug was observed in 45% of the patients, and in 11 patients (4.6%) three mutations to etravirine were verified. Although no patient in our cohort made use of etravirive, the observed resistance mutations to this drug are likely explained by cross-resistance due to the previous exposure to efavirenz or nevirapine. In this cohort, we observed that patients who used nevirapine were more likely to develop resistance to etravirine than patients who used efavirenz (data not shown).
90M was the most frequent mutation among those affecting viral protease, which is in agreement with the high rate of previous use of nelfinavir in this cohort. Other mutations related to nelfinavir use, such as 46IL, 30N, and 88DS, were also prevalent. A mutation in codon 54, which can impair viral sensitivity to all PIs, was the second most frequent among the main mutations. Possibly, the codon 50 mutation was observed less frequently because it is specific of newer PIs, namely atazanavir (50L), darunavir, lopinavir-ritonavir, and fosamprenavir (50V), 4,5 which were infrequently used or not used by this population.
In recent studies, the emergence of resistance mutations to antiretroviral agents, regardless of class, was associated with a significant increase in mortality. 11 –15 The presence of 118I in 28.8% of the cases in this cohort was also remarkable. In spite of not being considered one of the main mutations with a strong impact on drug resistance, it often closely follows other mutations of the TAM-1 pathway, and has been linked to advanced disease and to AIDS progression. 16 It is known that an accumulation of a large number of resistance mutations may restore viral fitness, which may explain the more rapid progression of disease seen in these individuals. 14,15 However, more studies are needed to help clarify the association between specific mutations and disease progression and mortality in HIV-infected patients.
The International AIDS Society understands that the evaluation of how the genetic variability of HIV-1 modifies the profile of sensitivity to antiretroviral drugs is essential. 4 According to a recent literature review, there is still controversy as to what extent viral subtypes of HIV-1 affect the emergence of antiretroviral resistance. 17 As the main purpose of our study was to explore possible differences between subtypes B and non-B in relation to the prevalence of resistance mutations, the determination of HIV-1 subtypes using rapid subtyping tools, instead of phylogeny, can be interpreted as a limitation of our study. Nevertheless, studies by Holguin et al. 18 and Yebra et al. 19 found almost complete concordance between the Stanford University tool and phylogenetic analysis for subtype B or non-B assignment, although the identification within non-B clades and circulating recombinant forms other than CRF02_AG may not be accurate with the use of rapid subtyping tools. Because we did not attempt to analyze the prevalence of resistance mutations within specific non-B clades, the use of rapid diagnostic tools can still be viewed as a valid approach for the analysis reported herein.
Brazil is a continental country exhibiting countrywide variations in HIV-1 subtypes. 20 As in all other regions of Brazil, subtype B was the most prevalent in our study, albeit over the years, a progressive increase has occurred in the relative proportion of non-B subtypes, mainly subtype F1 and recombinant B/F1. The same trend has been observed in central-western, 21 northeastern, 8,22 and southeastern 7,23 Brazil, although a study from the central-western region of the country reported an increase in the prevalence of subtypes F1 and C but a slight decrease of recombinant B/F1 in more recent years. 24 In that study, 82.5% of antiretroviral-naive patients were assigned subtype B, 6.2% were subtype F1, and 3.1% were subtype C. 24 We did not observe any case of subtype C virus in our study. In Brazil, subtype C is still mainly concentrated in the southern region, 25,26 although this subtype has been sporadically reported in the northern, 27 northeastern, 22 and central-western regions. 24 In southeastern Brazil, subtype C has spread recently 28 and has been described in many cities, 7,20,23,28,29 including a previous study of vertically infected children in our community. 30 Although we did not conduct a phylogenetic analysis to rule out cross-contamination as the reason for the absence of subtype C, all sequences obtained from samples were subjected to quality control assessments to exclude sample mix-ups or contamination (see Materials and Methods).
The main differences in the prevalence of mutations between viral subtypes were concentrated in the viral protease. It has been suggested that when the subtype B virus develops resistance to nelfinavir, it tends to develop mutation 30N, while non-B subtypes (specially C, F, G) are more likely to develop the 90M mutation. 5,31 Our results suggest otherwise. Among the secondary mutations to PIs, 20MIRTLV, 36ILVTA, and 89IMT were more prevalent in non-B subtypes, while 10FR, 63P, 71ILTV, and 77I were more common in the subtype B virus, data very similar to those described in other studies. 7,17 In a study by Brindeiro et al., 20 mutation 89IMT was 8.3 times more likely to be observed in non-B subtypes. It is important to emphasize that the differences observed were concentrated in 7 of the 12 most prevalent secondary mutations to the PI.
There was a high prevalence of polymorphisms in protease, especially in non-B subtypes. This has been widely documented. 4,32,33 The increased frequency of these natural polymorphisms may affect susceptibility to antiretrovirals by indirect means. 17 Accordingly, it is necessary to create optimized instruments to measure accurately susceptibility to antiretroviral drugs among non-B subtypes, especially in relation to PIs.
The presence of antiretroviral resistance is intrinsic to the use of large-scale antiretroviral therapy. The pattern of resistance mutations in this population was in accordance with the history of the wide use of non-HAART strategies in the past. Patterns of mutations observed among the viral subtypes of HIV-1 are in line with studies from abroad. It is crucial to maintain regional surveillance systems to monitor the prevalence of antiretroviral drug resistance mutations as well as HIV-1 genetic variability. From a public health perspective, such surveillance is of the utmost relevance to better prevent the transmission of resistant strains, to assess the need for developing and introducing newer antiretroviral drugs, and to better understand the impact of HIV-1 genetic variability on diagnosis and prognosis of HIV and on the development of an HIV vaccine. This is underscored by the still limited therapeutic armamentarium, the high cost of newer, patent-protected antiretroviral drugs, and the implied risks to universal access to treatment.
Footnotes
Acknowledgments
We gratefully thank the Federal University of Minas Gerais for performing the genotyping tests.
Author Disclosure Statement
No competing financial interests exist.