
Abstract
E
As a result of metabolic enzyme autoinduction following a month of oral therapy, the half-life of nevirapine (200 mg twice daily) stabilizes at approximately 24 h. Simplification to a once-daily regimen was the objective in developing an extended release formulation. This was achieved by delaying the release of the total nevirapine dose at a slower rate over a 24-h period. Systemic absorption is prolonged for an additional day, thereby minimizing the fluctuations in the peak-to-trough concentrations of the active drug. As long as there is drug in the intestinal tract, 4 this smoothing of the circulating drug concentrations leads to a longer timeframe at which the drug is at therapeutic concentrations, thereby minimizing the impact of a single missed dose of extended release nevirapine. Minimizing the impact of a single missed dose is important for a nonnucleoside reverse transcriptase inhibitor (NNRTI) such as nevirapine, as adherence rates of less than 95% have been associated with inadequate long-term treatment outcome. 5
In the 2NN study, 6 one treatment arm consisting of 208 patients on immediate release nevirapine 400 mg once daily had a median C max concentration of 7.88 μg/ml and a trough concentration of 3.26 μg/ml, resulting in a peak-to-trough ratio slightly greater than 2, consistent with dosing based on the half-life of the drug. In the VERxVE trial, 3 with 418 patients on nevirapine extended release 400 mg once daily, the trough concentration of 3.50 μg/ml was maintained. However, the estimate of C max in a subset of patients was only 3.77 μg/ml, resulting in a peak-to-trough ratio approaching 1, consistent with extended first-order release and absorption matching the elimination rate of the drug.
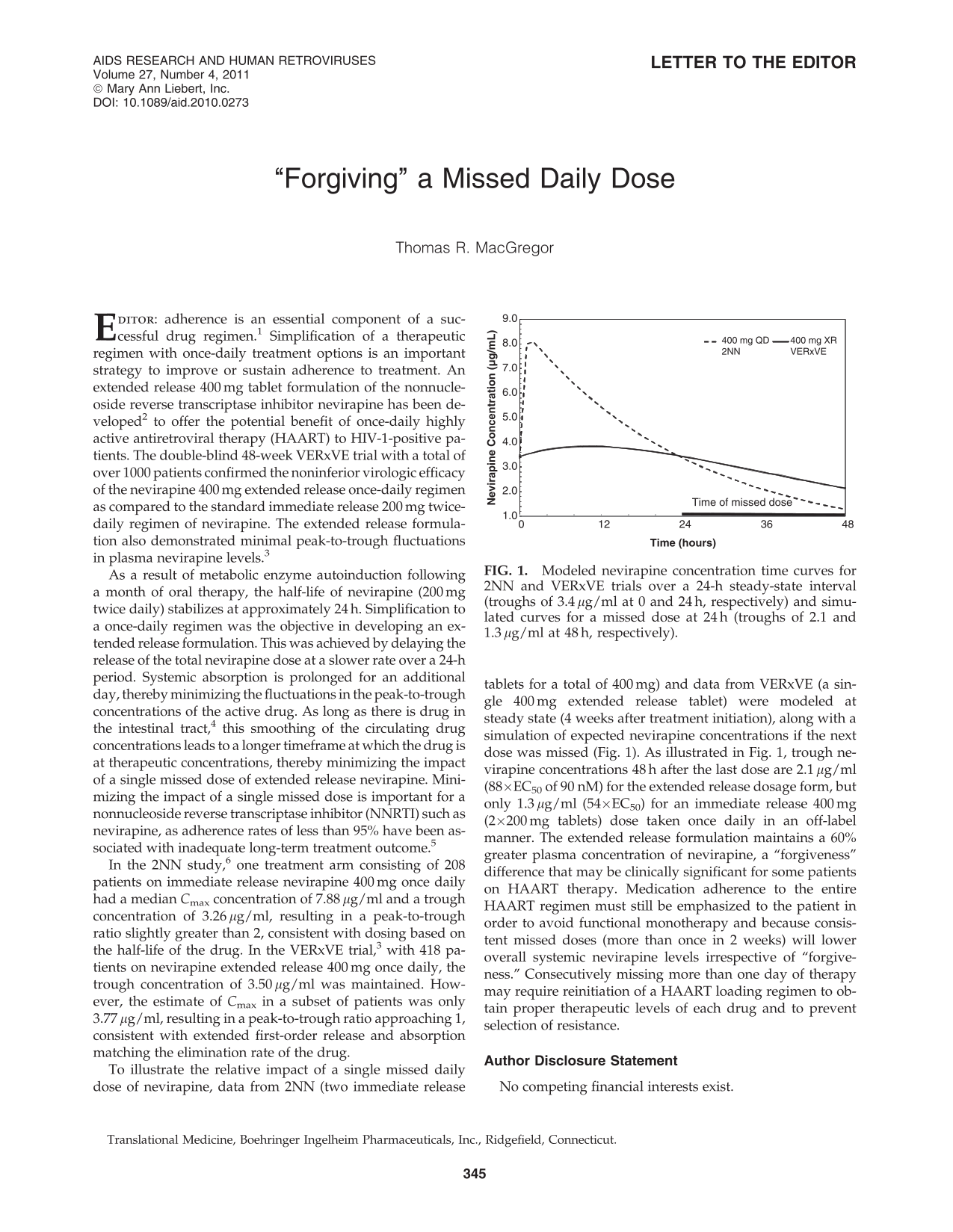
To illustrate the relative impact of a single missed daily dose of nevirapine, data from 2NN (two immediate release tablets for a total of 400 mg) and data from VERxVE (a single 400 mg extended release tablet) were modeled at steady state (4 weeks after treatment initiation), along with a simulation of expected nevirapine concentrations if the next dose was missed (Fig. 1). As illustrated in Fig. 1, trough nevirapine concentrations 48 h after the last dose are 2.1 μg/ml (88 × EC50 of 90 nM) for the extended release dosage form, but only 1.3 μg/ml (54 × EC50) for an immediate release 400 mg (2 × 200 mg tablets) dose taken once daily in an off-label manner. The extended release formulation maintains a 60% greater plasma concentration of nevirapine, a “forgiveness” difference that may be clinically significant for some patients on HAART therapy. Medication adherence to the entire HAART regimen must still be emphasized to the patient in order to avoid functional monotherapy and because consistent missed doses (more than once in 2 weeks) will lower overall systemic nevirapine levels irrespective of “forgiveness.” Consecutively missing more than one day of therapy may require reinitiation of a HAART loading regimen to obtain proper therapeutic levels of each drug and to prevent selection of resistance.

Modeled nevirapine concentration time curves for 2NN and VERxVE trials over a 24-h steady-state interval (troughs of 3.4 μg/ml at 0 and 24 h, respectively) and simulated curves for a missed dose at 24 h (troughs of 2.1 and 1.3 μg/ml at 48 h, respectively).
Footnotes
Author Disclosure Statement
No competing financial interests exist.