
Abstract
The determinants of HIV-associated cardiovascular disease (CVD) are not well understood. Periodontal disease (PD) has been linked to CVD but this connection has not been examined in HIV infection. We followed a cohort of HIV-infected adults to ascertain whether PD was associated with carotid artery intima media thickness (IMT) and brachial artery flow-mediated dilation (FMD). We performed a longitudinal observational study of HIV-infected adults on HAART for <2 years with no known heart disease. PD was characterized clinically and microbiologically. Cardiovascular disease was assessed by IMT/FMD. Linear mixed models assessed cross-sectional and longitudinal associations between PD and FMD/IMT. Forty three HIV+ adults completed a median of 24 (6–44) months on the study. Defining delta to be the change in a variable between baseline and a follow-up time, longitudinally, on average and after adjusting for change in time, CVD-specific and HIV-specific potential confounding covariates, a 1-log10 increase in delta Porphyromonas gingivalis was associated with a 0.013 mm increase in delta IMT (95% CI: 0.0006–0.0262; p=0.04). After adjusting for the same potential confounding covariates, a 10% increase in delta gingival recession was associated with a 2.3% increase in delta FMD (95% CI: 0.4–4.2; p=0.03). In a cohort of HIV-infected adults, an increase in subgingival Porphyromonas gingivalis, a known periodontal pathogen, was significantly associated with longitudinal increases in IMT, while increased gingival recession, which herein may represent PD resolution, was significantly associated with longitudinal improvement in FMD. In the context of HIV infection, PD may contribute to CVD risk. Intervention studies treating PD may help clarify this association.
Introduction
H
Periodontal disease (PD) has been linked to CVD by numerous epidemiological and animal studies. 24 –27 PD-related bacterial genomes have been identified in excised human vascular tissue. 28 Recently, prospective studies treating PD in HIV-negative cohorts have reported improvements in FMD and IMT directly related to improved periodontal health. 29,30 Our group has previously found high levels of severe PD in our HIV-infected cohort. 31 This study examined whether severity of PD in HIV-infected adults was associated with an accelerated progression of FMD and IMT.
Materials and Methods
Subject selection
Adult patients receiving primary HIV care at University Hospitals Case Medical Center (UHCMC), The Cleveland Clinic Foundation (CCF), and MetroHealth Medical Center (Metro) were recruited into this IRB-approved study by physician referral or response to posted advertisements. All subjects provided written informed consent prior to any study procedures. Clinical data were obtained from an electronic database (UH/CMC) or electronic/paper medical records (Metro and CCF). Eligible subjects had HIV infection and were age 18 years or older. To increase cohort homogeneity, we included those who were planning to initiate HAART in the next 2 months or had been treated for less than 2 years. Subjects with clinical evidence of CVD manifested as myocardial infarction, cerebrovascular accident, transient cerebral ischemia, or angina pectoris were excluded as were patients who were pregnant, required antibiotic prophylaxis before dental procedures, 32,33 had fewer than 20 teeth, a diagnosis of cancer in the past 5 years, other uncontrolled systemic illnesses, evidence of ongoing medication noncompliance, or diabetes mellitus. Study subjects were seen between May 2005 and March 2009.
Study design
This was a prospective longitudinal study. All subjects were seen at baseline to perform ultrasound and PD measurements and to obtain 12-hour fasting blood work. These measures were repeated during one or more final follow-up study visits at a median of 24 months after enrollment (range: 6–44). Dental care was discussed in detail; information on sources of dental care was provided, but no dental treatment (i.e., periodontal treatment, prophylaxis, restorations, or extractions) was provided by the investigator throughout the study. Dental visits were as per self-report at recall visits and tooth loss was determined using raw data and examination of digital photographs.
Assessment of endothelial function
Endothelium-dependent FMD was obtained on all subjects by one experienced registered vascular technician (RVT), following an established protocol. 34 Subjects were seen in the morning after a 12-hour fast and 8 h after their last cigarette. Before testing, subjects rested supine for 20 min. Baseline flow velocity and vessel diameter measurements were obtained on the right brachial artery approximately 4.5 cm proximal to the elbow crease. Optimal longitudinal arterial sections were determined using an Echo-Doppler ultrasound system (Acuson L10, Aspen Advanced, GPS Medical, Indianapolis, IN) with a 10-MHz multifrequency linear array transducer. Reactive hyperemia (RH) was induced above the antecubital fossa using a blood pressure/tourniquet cuff (Model SC5, Hokanson, Bellevue, WA). Absence of arterial flow was verified using color Doppler flow and maintained for 5 min. RH-induced velocity and vessel diameter were measured 10–15 s and 60 s after cuff deflation, respectively. Arterial diameter was determined off-line using edge-detection software (Vascular Research Tools 5, Medical Imaging Applications, Coralville, IA). We obtained 60 image frames over 3 s (approximately 3–5 heart beats) from the cine-loop video clip. Low-quality images (based on edge detection software) were identified on-line and deleted prior to automated analyses. For longitudinal assessments, stored baseline images were visualized on a laptop computer to identify anatomical landmarks and obtain images from the same vessel location. Blood pressure (BP) was measured using an automated monitor (Vital Signs Monitor 300, Welch/Allyn, Skaneateles Falls, NY) applied to the left arm before and after ultrasound testing.
Assessment of arterial structure
B-mode ultrasonographic examination was performed on the right common carotid artery, just proximal to the carotid bulb, on all subjects using the ultrasound system described above. Measurements of the carotid artery IMT were obtained on the far wall by the same designated sonographer certified by a core laboratory for the Study of Fat Redistribution and Metabolic Change in HIV infection (FRAM) 35 using an established protocol. 36 Carotid artery IMT was determined off-line using the same edge-detection software as above. Both IMT and FMD images were saved on magnetic optical disks (230 MB, Verbatim Optical, Charlotte, NC), and edge-detection software results were saved on disk. The one designated ultrasound technician was trained and certified for FMD and IMT at core training laboratories (Tufts-New England Medical Center, Boston, MA) prior to the study initiation.
Measurement of periodontal disease
Periodontal disease measurements were performed at six sites per tooth on all teeth by one dentist (L.T.V.) as previously described. 31 PD was quantified as the percent of teeth (0–100%) with ≥1 of 6 sites meeting or exceeding the following cut-points: ≥5.0 mm for periodontal probing depth (PPD), >0 mm (i.e., loss of gingival tissue relative to the cemento-enamel junction) for gingival recession (REC), and ≥4.0 mm for clinical attachment level (CAL). 31 Bleeding on probing (BOP) was defined as the percent of teeth with ≥4 of 6 sites exhibiting BOP. We also collected subgingival dental plaque samples and quantitated DNAs for specific bacteria associated with severe PD, 37 i.e., Porphyromonas gingivalis (Pg), Treponema denticola (Td), and Tanneralla forsythia (Tf), by real-time PCR in units of log genome copy number per μg total DNA as previously reported (NCBI accession numbers D64081.1, U29399.1, and AY423857.1, respectively). 31,38 We also measured total bacterial DNA levels by quantifying gene copies for the bacterial 23S ribosomal RNA using real-time PCR as we reported previously. 31 A pooled plaque sample of eight sites was collected from two predetermined sites in each quadrant of the mouth as previously described. 31 PD data, which were collected either on or after the ultrasound examination dates, were obtained more often than ultrasound data. Since PD data were collected within 1 month of ultrasound data on 96% of subjects, and PD data in this observational study were not expected to change significantly within 1 month, the PD data collection date was set to the ultrasound data collection date in the final analyses.
Cardiovascular risk factors
At the baseline visit and subsequent study visits, the number of pack per day years (ppd-yrs) of cigarette smoking, compliance with HAART, and use of antihypertensive and lipid-lowering medication were recorded; family history of CVD was obtained at baseline. Fasting blood work included a lipid panel (i.e., total cholesterol, HDL, LDL, VLDL cholesterol, HDL/total cholesterol ratio, and triglycerides), insulin, glucose, and high sensitivity C-reactive protein (hs-CRP); all values were measured as previously reported. 31 Time since date of first known HIV seropositivity, nadir CD4+ T cell count, and months on HAART were abstracted from the medical record. All CD4+ T cell counts and HIV RNA levels were measured within 4 months of the baseline study visit; these prebaseline data were used as a surrogate for baseline values. Homeostasis model assessment of insulin resistance (HOMA-IR) was calculated as previously reported. 39
Statistical analyses
Baseline variables were summarized using standard descriptive statistics. To characterize disease progression during the study and to adjust for variability of time on study, we estimated the average change in study variables from baseline to 24 months using a linear mixed-effects model that included a random intercept and slope to model the subject-specific trajectory over time, assumed an unstructured within-subject correlation structure, and adjusted for the change in time between baseline and follow-up times.
For each measure of PD, a linear mixed-effects repeated-measures model was also used to jointly estimate the association between PD at baseline and FMD or IMT at baseline (termed the cross-sectional effect) as well as the association between delta PD and delta FMD or IMT (termed the longitudinal effect), where delta was defined to be the change in the variable between baseline and the follow-up time. Random effects were also incorporated into each model using a random intercept and slope and unstructured within-patient correlation structure. Because time on study varied, time was treated as a continuous variable and the change in time between baseline and follow-up time was adjusted for in all models. For both FMD and IMT models, baseline covariates in each model included CVD-specific variables: age, male gender, total smoking exposure, body mass index (BMI), systolic BP, and hs-CRP as well as HIV-specific baseline covariates: HAART duration, CD4+ T cell count, HIV RNA, and time since first seropositive. We selected these variables based on prior published studies. 4,5,10,13 –17,40,41
Results
Among the 58 enrolled subjects, 11 did not have follow-up visits, two did not definitively initiate HAART, and two had full-mouth extractions during the study, resulting in an analytic sample of 43 subjects. For these 43 subjects, the median time on study was 24 months (range: 6–44), with 81% completing one ultrasound follow-up visit and 19% completing two or more ultrasound follow-up visits, resulting in a total of 94 visits. During the study, 33 subjects (77%) reported one or more dental visits; however, only seven subjects (16%) reported any scaling and root planning visits. As well, eight subjects (19%) had a total of 18 teeth extracted (excluding seven teeth with loss of clinical crown but retained root); median tooth loss was one tooth (range: one to eight teeth) extracted and was primarily due to dental caries. The subject recruitment flow diagram is depicted in Fig. 1.
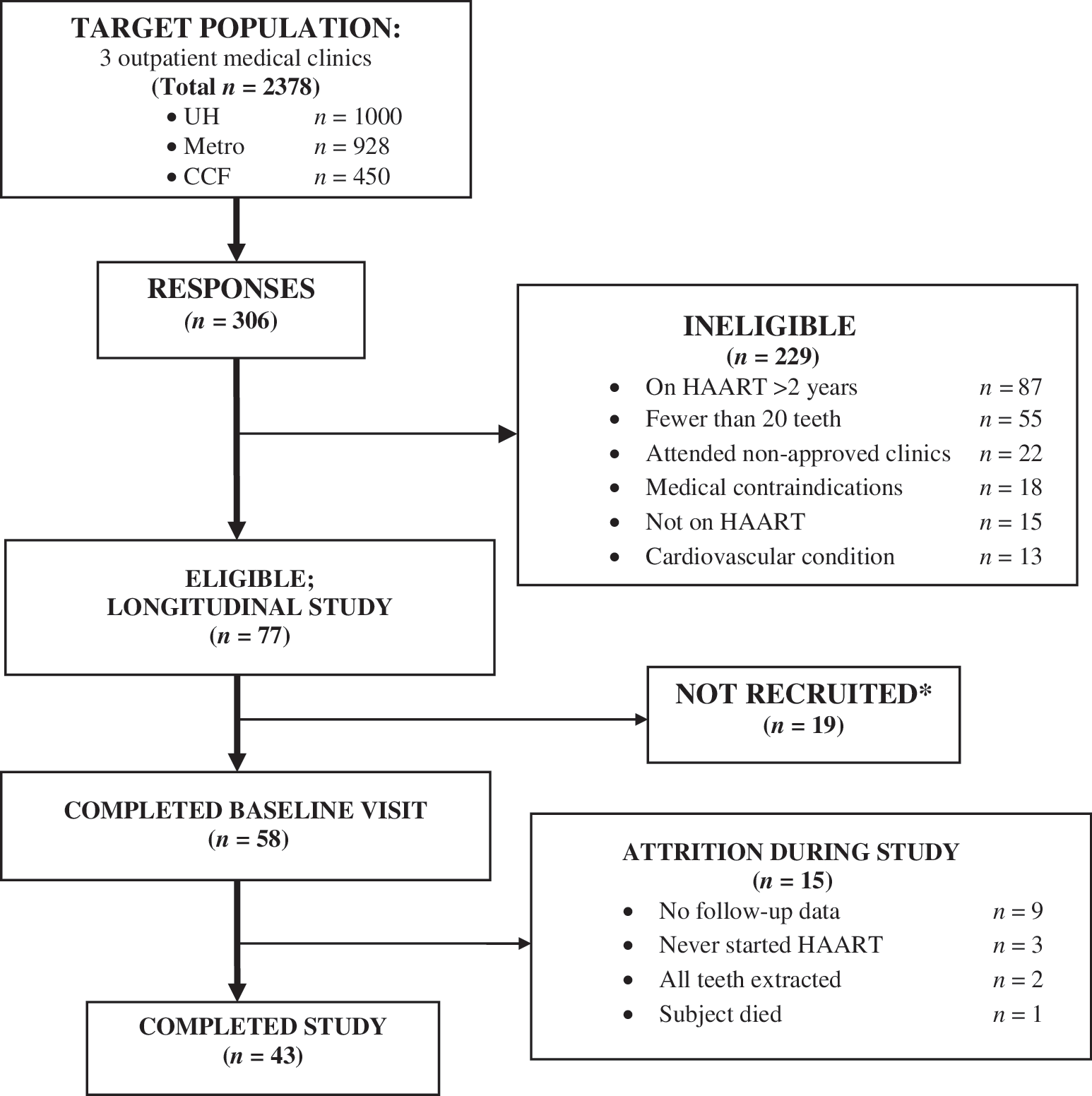
Subject recruitment flow diagram. *Reasons for non-recruitment: could not be reached by phone, subject lost interest, scheduling conflicts.
Subjects had a mean (±SD) age of 38 (±8) years. Most subjects were black (57%), males (77%) who received federally-funded medical insurance (70%), and had other risk factors for heart disease: a smoking history (72%) and a family history of premature cardiovascular disease (CVD) (21%) (Table 1). The baseline median CD4+ T cell count was 363 cells/μl and the baseline median nadir CD4+ T cell count was 230 cells/μl. The median plasma HIV RNA level for the four subjects who were not on HAART at baseline was 55,552 copies/ml, and 879 copies/ml for the remaining 39 subjects on HAART at baseline. At baseline, 39 (91%) were on HAART and four (9%) were naive to antiretroviral therapy. Of those on HAART at baseline, most (98%) were on a “backbone” nucleoside/nucleotide analogue (NUC), with 54% on a protease inhibitor (PI)-containing regimen and 46% receiving NUCs and a nonnucleotide reverse transcriptase inhibitor (NNRTI). During the entire study, 34 subjects (79%) remained on HAART, one subject (2%) was off HAART for less than 2 weeks, and eight subjects (19%) were off HAART for more than 2 weeks. For those off HAART during the study, the mean (median) time off HAART was 9.2 (10) months.
Data are shown as median (first and third quartiles), unless otherwise specified.
HAART, highly active antiretroviral therapy; CVD, cardiovascular disease.
Table 2 shows the estimated average change in key variables over 24 months. In terms of PD progression over 24 months, PPD, CAL, and BOP decreased significantly by 11.9±2.2 (p<0.0001), 11.2±2.6 (p≤0.001), and 13.6±3.0 (p≤0.001) percent of teeth exceeding cut points (see Materials and Methods; measurement of PD), respectively; meanwhile, bacterial measures of PD were reduced insignificantly over time. Mean CD4+ T cell count increased significantly (140.3±29.8 cell/μl; p<0.0001) and mean plasma HIV RNA levels decreased significantly by 1.6±0.4 log copies/μl (p < 0.001). HDL cholesterol increased by 5.7±2.5 mg/dl (p=0.03) and the cholesterol/HDL ratio decreased significantly by 0.65±0.22 (p=0.006). Levels of glucose, insulin, and HOMA-IR decreased insignificantly (p>0.32 for all variables) over the estimated 24-month period, while levels of triglycerides and VLDL increased insignificantly (p≥0.91 for both variables; full data not shown).
IMT, carotid artery intima media thickness; FMD, brachial artery flow-mediated dilation; Hs-CRP, high sensitivity C-reactive protein; PPD, periodontal probing depth; REC, gingival recession; CAL, clinical attachment level; BOP, bleeding on probing; BP, blood pressure; HDL, high-density lipoprotein; LDL, low-density lipoprotein. *Units are in log genome copy number per μg DNA.
Overall, we found that IMT increased by 0.007±0.021 mm (p=0.76) over 24 months (Table 2). In the longitudinal analysis, after adjustment for change in time and the CVD and HIV-specific potential confounding covariates, we found that a 1-log10 increase in delta Porphyromonas gingivalis was associated with a 0.0134 mm increase in delta IMT (95% CI: 0.0006–0.0262; p=0.04, Fig. 2 and Table 3). In cross-sectional and longitudinal analyses, no other markers of PD were significantly associated with IMT (Table 3).
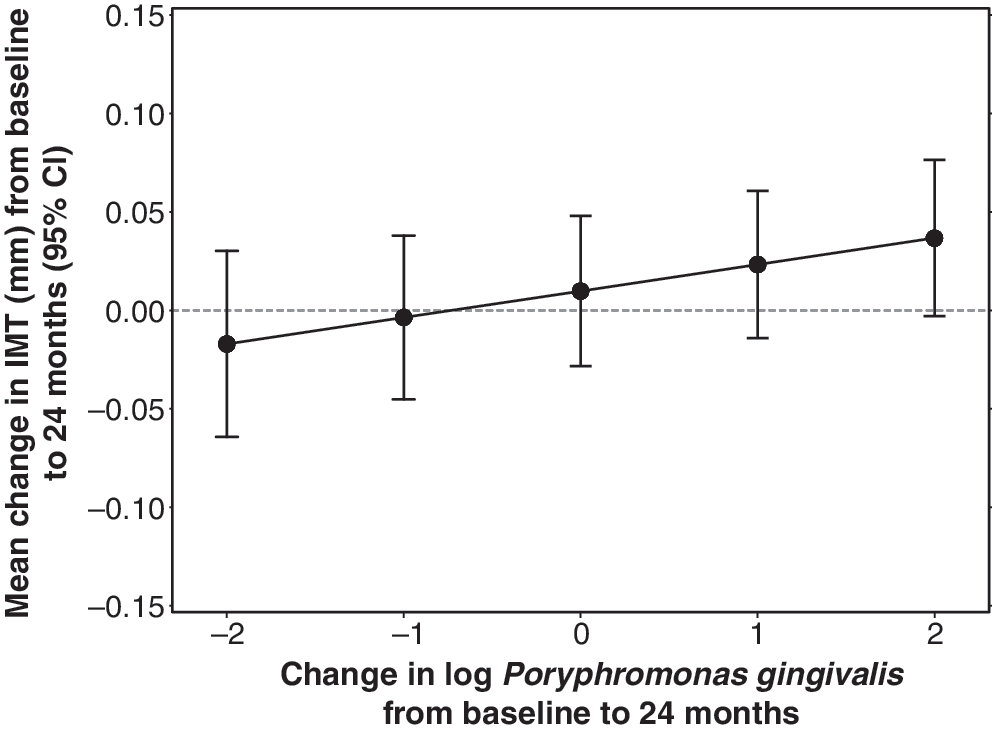
Longitudinal effect of subgingival Porphyromonas gingivalis on intima media thickness (IMT).
PD, periodontal disease; IMT, carotid artery intima media thickness; PPD, periodontal probing depth; REC, gingival recession; CAL, clinical attachment level; BOP, bleeding on probing; P. gingivalis, Porphyromonas gingivalis; T. denticola, Treponema denticola; T. forsythia, Tannerella forsythia; 23S rRNA, 23S ribosomal RNA. Model adjusted for change in time and the CVD and HIV-specific potential confounding covariates.
We also found that FMD increased by 0.7±1.9% (p=0.72) over 24 months (Table 2). In the longitudinal analysis, after adjustment for change in time and the CVD and HIV-specific potential confounding covariates, we found that a 10% increase in delta gingival recession was associated with a 2.27% increase in delta FMD (95% CI: 0.37–4.17; p=0.03, Fig. 3 and Table 4). There was no evidence of a cross-sectional or longitudinal association between any other markers of PD and FMD (Table 4).
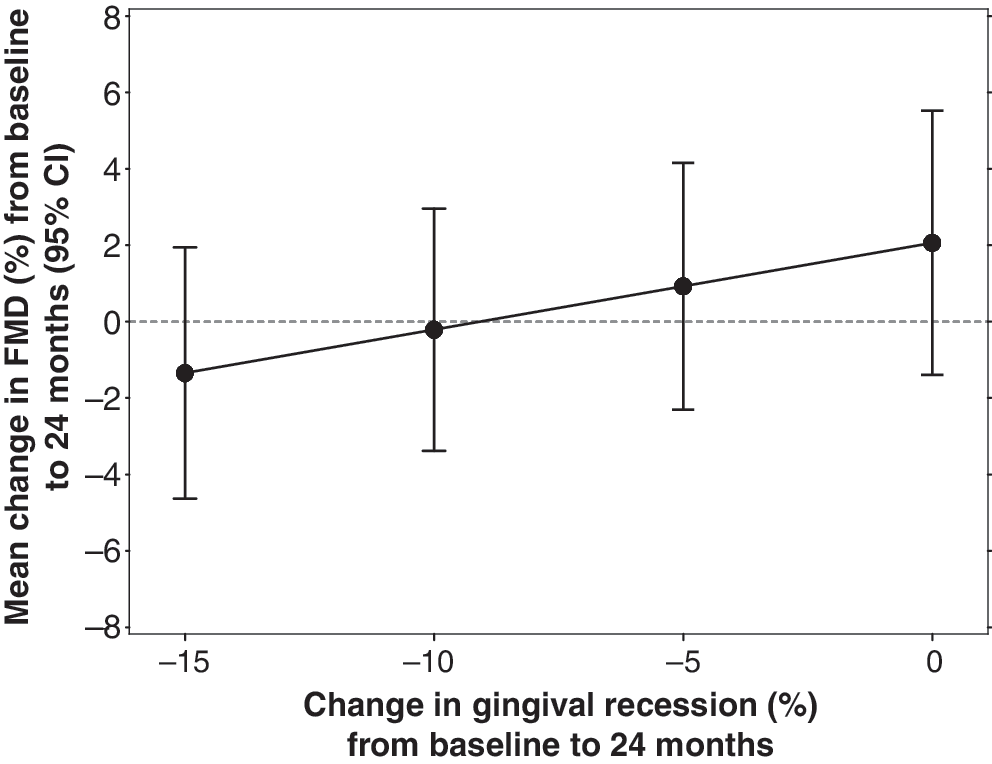
Longitudinal effect of gingival recession (REC) on flow-mediated dilation (FMD).
PD, periodontal disease; IMT, carotid artery intima media thickness; PPD, periodontal probing depth; REC, gingival recession; CAL, clinical attachment level; BOP, bleeding on probing; P. gingivalis, Porphyromonas gingivalis; T. denticola, Treponema denticola; T. forsythia, Tannerella forsythia; 23S rRNA, 23S ribosomal RNA. Model adjusted for change in time and the CVD and HIV-specific potential confounding covariates.
Discussion
In our HIV-infected cohort, we found a statistically significant longitudinal association between increased levels of P. gingivalis and increased (worsened) levels of carotid artery IMT. Furthermore, we found a statistically significant longitudinal association between increased gingival REC and increased (improved) levels of brachial artery FMD. CD4+ T cell count and level of HIV RNA improved significantly during the study, implying successful therapy and immune reconstitution on HAART.
The longitudinal association between levels of P. gingivalis and levels of IMT emerged only after adjusting for preselected CVD-specific and HIV-specific potential confounding covariates (see Supplementary Tables S1A and B; Supplementary Data are available online at
Historically, clinical measures of PD were developed to quantify clinical signs of PD, 48 not the mucosal exposure to microbes and their byproducts that could trigger systemic effects. Therefore, it is not surprising that clinical measures of PD in our cohort were unrelated to IMT; these findings are consistent with a study of almost 5000 subjects by Beck et al. in the Atherosclerosis Risk in Communities (ARIC) Study. These authors found that clinical measures of PD were not associated with coronary heart disease (CHD) while serum IgG antibodies to known periodontal pathogens were significantly associated with CHD. 49
Our data herein support the growing literature that quantification of periodontopathogenic bacteria in subgingival biofilm 50,51 is a more direct and specific measure of PD as an exposure contributing to CVD risk. Comparing our longitudinal findings in an HIV-infected cohort to the general population is limited at present because ongoing studies such as The Oral Infections and Vascular Disease Epidemiology Study (INVEST) have, to our knowledge, published only cross-sectional reports. 50 –53 These authors have linked the cumulative level of periodontopathogenic microbial DNA to increased IMT, 50 hypertension, and blood pressure. 51 Our findings support these earlier cross-sectional associations 50,51 and extend them into an HIV-infected population examined longitudinally.
While it is plausible that P. gingivalis could have increased virulence in an HIV-infected host, our limited sample size did not permit us to analyze whether or not P. gingivalis is acting as an independent risk factor for IMT. Our present longitudinal study, “Immune and Inflammatory Consequences of Intensive Periodontal Disease Treatment in HIV-Infected Adults,” is designed to more effectively address the mechanisms of our finding linking PD to IMT in this population.
Our finding of an association between apparently worsening REC and improving FMD over time deserves further attention (see Supplementary Tables S2A and 2B for a time-adjusted model and the model adjusted for time and CVD-specific covariates; Supplementary Data are available online at
Beck et al. proposed that when examining the connection between periodontal disease and systemic disease, components of PD (i.e., PPD, REC, and CAL) may individually influence outcome measures. 54 This concept was clearly demonstrated in our earlier work wherein immune-related and metabolic independent variables were differentially associated with the dependent outcome variables PPD, REC, and CAL in a cross-sectional cohort of 112 HIV+-infected adults. 31 Herein, our study findings that components of traditionally defined PD are differentially related to established markers of cardiovascular disease (i.e., IMT and FMD) further support this concept. Whether REC, a component of PD, is related to brachial artery FMD in HIV-uninfected cohorts is, to our knowledge, unknown.
This study revealed that defining PD more broadly (i.e., microbiologically and as several clinical constructs) uncovered associations linking PD to markers of cardiovascular disease. It is possible that the associations detected herein may be due to residual confounding; however, we identified and included a priori many critical confounding variables in our analytic model. Based on our results, including both CVD-specific and HIV-specific confounding covariates appears to be critical when examining markers of CVD in an HIV-infected cohort.
Our results showing a slight improvement in FMD over time in HIV-infected adults on HAART (Table 2) are in agreement with findings of improved FMD at 4 and 24 weeks after HAART initiation as reported by Torriani et al., 8 but differ from findings of worsened FMD over 1 year in a more heterogeneous cohort of HIV-infected adults as reported by Obueyungbo et al. 17 We propose that our results are more similar to those of Torriani et al. because, like their cohort, ours had recently started HAART, had a relatively low baseline CD4+ T cell count, and most but not all of our subjects (59%) achieved plasma HIV RNA levels <50 copies/ml at the final study visit. In the context of other longitudinal studies, our findings suggest that the stage of HIV disease and the specific immune profile of an HIV-infected cohort may influence the trajectory of change in subclinical CVD markers across time.
Our finding that IMT worsened by 0.0035 mm per year (i.e., 0.007 mm/2 years) agree with four previous longitudinal studies of HIV-infected cohorts, 14 –17 but are closest to findings by Currier et al. indicating that IMT progressed a median of 0.0096 mm/year in a PI-treated group and 0.0058 mm/year in a non-PI-treated group. 15 Among several pooled HIV-negative cohorts, the annual mean change in common carotid IMT is 0.015 mm 55 ; thus, the institution of HAART and possibly other unmeasured effects (i.e., improved care, health education) might have played a role in putting our subjects at a risk profile similar to the general population. The fact that FMD improved but IMT worsened during our study may represent either that the time frame of change is longer for IMT than for FMD or that FMD and IMT may be influenced by different mechanisms in HIV-infected adults. Longitudinal findings in an HIV-infected cohort reported by Obueyungbo et al., wherein traditional risk factors for CVD (i.e., age, male gender, and smoking status) were significantly related to IMT but not FMD, would tend to support the latter interpretation. 17
Our study had several strengths. We followed a relatively homogeneous cohort in terms of stage of HIV disease—as most of our cohort had recently started HAART. We measured PD thoroughly and often (a median of four times over 2 years) and were able to quantify this exposure as a continuous variable. We defined PD microbiologically as well as clinically—as a variable broken down into separate readouts (i.e., PPD, REC, and CAL) as advised by Beck et al. 54,56 We measured both IMT and FMD longitudinally, and collected and quantified numerous potential confounding variables. We reported a thorough immunological profile of our cohort (including time on HAART, time since first seropositive, nadir CD4+ T cell count, and time since nadir CD4+ T cell count). Finally, this is the first report relating PD to IMT and FMD in an HIV-infected cohort. CVD is a leading cause of death in HIV-infected adults. 1,57,58 We have previously found high levels of severe PD in a predominantly black urban male cohort of HIV-infected adults, 31 and since black males are disproportionately affected with HIV/AIDS in the United States, 59 these findings may be broadly generalizable. Finally, if PD represents a previously unrecognized modifiable risk factor for CVD in HIV-infected adults, this finding could have great public health importance.
Our study also had a number of limitations. Foremost, the sample size is small and, against the backdrop of significant immune reconstitution, may be underpowered to detect clinically significant cross-sectional and longitudinal associations between measures of PD and markers of CVD risk. Given the complexity of our statistical model, the necessity to include both cross-sectional and longitudinal effects of PD exposure on markers of CVD risk as well as our small sample size, the number of confounders that could be included in our final analytic model was limited; however, we included many previously identified confounding variables. 4,5,10,13 –17,40,41 Another limitation is that most subjects in our cohort had moderate to severe PD since a comparison group of HIV+ adults on HAART with low levels of PD was not readily available. 31 Thus, our within-subjects study design controlling for time on HAART is a reasonable and practical approach to addressing this question.
This study suggests a potential link between PD and CVD risk in HIV-infected adults on HAART. Since PD is a chronic oral infection that can be reduced or eliminated, an intervention study designed to reduce PD in HIV-infected adults would help determine whether this association reflects a modifiable risk factor for CVD.
NCBI Accession Numbers
Porphyromonas gingivalis: NCBI accession number D64081.1; Treponema denticola: NCBI accession number U29399.1; Tannerella forsythia: NCBI accession number AY423857.1. 23S rRNA (Housekeeping gene; NCBI accession number not applicable).
Appendix
Probes and primers for select periodontal bacteria:
Note: Probe and primer sequences were as previously reported in Vernon et al. 31 :
Forward primer: 5′-TCTCGGAGAAAGGTACGCCTAT-3′
Reverse primer: 5′-TCATCGCACGTGTTTCAGAAA-3′
Forward primer: 5′-GGAAAGGCCGGTGTTCATG-3′
Reverse primer: 5′-CAATCCCATACCTAAATACGGCTTA-3′
Forward primer: 5′-AGCCCCAGTAAACGGCG-3′
Reverse primer: 5′-AATTTCGCTACCTTAGGACCGTTA-3′
Footnotes
Acknowledgments
We especially thank all of our research participants. We appreciate the professional suggestions, scientific input, and/or assistance from Drs. Christopher Whalen, Isaac Rodriguez-Chavez (R-21 Program Director, see below), Robert Kalayjian, Judith Currier, Robert Asaad, Yiping Han, Nabil Bissada, Wendy Armstrong, Mr. Alan Chiunda, Mr. Gene Doverspike, Ms. Leslie Anderson, and Ms. Katie Przepyszny. Supported by NIDCR, Grants K23 DE15746-01A1 and R21 DE21376-01, the Center for AIDS Research (CFAR), AI36219, the William T. Dahms, M.D. Clinical Research Unit (Dahms CRU) of the CTSC, UL1 RR024989, NIH, M01 RR000080, the General Clinical Research Center (GCRC), the CWRU Department of Biological Sciences, OPR892521 and the Case Western Reserve University/Cleveland Clinic CTSA Grant, UL1 RR024989 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health and NIH roadmap for Medical Research.
An abstract was submitted to the International Association of Dental Research (IADR) on 10/08/2010; 89th General Session and Exhibition of IADR, San Diego, California, meeting March 16–19, 2011. It was withdrawn prior to the meeting.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.