
Abstract
The diverse Brazilian AIDS epidemic has reached small cities and scant molecular information is available about the epidemic in Northern Brazil, where the incidence is growing. This study describes transmitted drug resistance and subtypes in the protease (PR) and reverse transcriptase (RT) regions among naive patients recruited in Palmas, the capital of Tocantins State, a newly built city in Northern Brazil. PR/RT regions were retrotranscribed from plasma HIV-1 RNA and 52 were sequenced after direct nested PCR. HIV-1 subtypes were assigned by phylogenetic analysis. Transmitted drug resistance was analyzed by the Calibrated Population Resistance tool Stanford Surveillance Drug Resistance Mutation. Most patients included (59.6%) were males, the median age was 30 years and were mainly referred because of heterosexual or homosexual unprotected sex. One male patient was from the Karajás indigenous tribe. The prevalence of transmitted resistance was 11.5% (CI 95%, 4.4–23.4%): nonnucleoside RT inhibitor mutations (n=3), nucleoside RT inhibitor mutations (n=2), and protease inhibitor mutations (n=1). Dual or triple class resistance was not observed. HIV-1 subtype BPR/BRT represented 78.8%, 5.8% were subtype CPR/CRT, and 1.9% were subtype F1PR/F1RT. Recombinant viruses represented 13.5% (07/52): BPR/F1RT (n=1), BPR/BF1RT (n=4), and CPR/CF1RT (n=2). This study about the AIDS epidemic in the recently founded city of Palmas/Tocantins in inland Northern Brazil shows moderate levels of transmitted drug resistance and the circulation of diverse recombinant viruses. This pattern is similar to what has been described in major metropolitan cities, suggesting the influence of imported cases from the south/southeast. Moreover these results indicate that patients from this setting should be monitored regarding transmitted drug resistance mutations.
Introduction
T
Extensive molecular epidemiology data of HIV-1 including several full-length or near full-length recombinant genomes from south/southeast Brazil indicate the prevalence of subtype B, followed by subtypes F1 and C. 10 –12 More recently a growing number of recombinant forms especially involving subtypes B and F1 and subtypes B and C have been described throughout the country. 6,7,9,13 –19
Most of what is known about HIV-1 drug resistance and molecular epidemiology in Brazil reflects the southeast region, considered the epicenter of the epidemic where the prevalence has been considered stable at 0.6% (around 600,000 individuals). 1 However, evidence indicates that the epidemic continues to grow in other parts of the country such as in the Northern region. 1 Scarce molecular information is available about the epidemic in North Brazil, which represents almost half of the country's territory comprising the Amazon region and is characterized by both low demographic density and low AIDS prevalence. 20 –22
This study reports for the first time HIV-1 drug resistance mutations and subtypes circulating among ARV-naive patients recruited in the newest Brazilian State capital, Palmas, located in the inland North State of Tocantins.
Materials and Methods
Study area, patients, and methods
The study area was Palmas City (around 220,000 inhabitants; 10° south/48° west), capital of Tocantins State in the North Brazilian region, legally created in 1989 from the division of Goiás State, which accounts for around 1300 notified AIDS cases. 1 Patients with a confirmed diagnosis of HIV-1 infection were recruited at the regional Public Health Central Laboratory [LACEN, the reference laboratory for CD4 counts and plasma viral load (PVL) assessments] in Palmas between 2008 and 2009. Inclusion criteria were patients with a recent or chronic diagnosis of HIV-1 infection, from both sexes, of any age range, and never treated with any ARV drug. Research Ethical Committees approved this study (HAA/HDT/SUS, CEPMHA/HC/UFG protocol #073/05) and all included patients signed an informed consent. For patients under 18 years, the informed consent was signed by the legal guardian. A standardized questionnaire was used to collect the sociobehavioral, clinical, and laboratory data (HIV RNA load: branched-chain DNA, bDNA, SIEMENS; CD4 counts: FACSCalibur, Becton Dickson).
For the molecular study the RNA was extracted from plasma (QIAamp Viral RNA Mini Kit, Qiagen, Hilden, Germany), reverse transcribed into complementary DNA (cDNA) (Invitrogen), and used as the target for nested polymerase chain reaction (nested-PCR) employing HIV-1 PR and RT K1/K2 external primers and DP10/F2 internal primers, as previously described.
7
The reaction products were sequenced using ABI Prism 3130 Genetic Analyzer (Applied Biosystems, USA). All generated sequences were subjected to quality control analysis by the HIV-1 Quality Analysis Pipeline Tool (available at
HIV-1 genetic subtypes were defined by the REGA automated genotyping tool version 2.0 and by phylogenetic inference. 25 Study sequences were aligned with reference sets from the Los Alamos HIV database (ww.hiv.lanl.gov) using the Clustal X software and adjusted manually by the BioEdit software. 24 Phylogenetic inferences were performed by the neighbor-joining (NJ) method under Kimura's two-parameter correction using MEGA4 software. 26 Bootstrap values (1000 replicates) above 70% were considered significant. Isolates with discordant subtypes in the PR and RT regions were analyzed by SIMPLOT 3.5.1 software in a 200-bp sliding window advanced in 20 bp step size increments (1000 replicates). 27 Sequences were gap-stripped, the transversion-to-transition ratio was set to 2.0, and distances were calculated according to Kimura's two-parameter model.
Transmitted drug resistance was analyzed using the Calibrated Population Resistance (CPR) tool employing the Stanford Surveillance Drug Resistance Mutation (SDRM) database (hivdb.stanford.edu). 28 The ARV mutation susceptibility profile was defined by the Stanford HIV Drug Resistance Database (accessed December 22, 2010).
Frequencies, medians of main variables, and 95% confidence interval (CI) were obtained using the Statistical Package for the Social Sciences (SPSS, 13.0) for Windows (Chicago, IL).
Results
Fifty-two ARV drug-naive HIV-1-infected patients were included in this study: 59.6% (31/52) were males; the median age was 30 years (14–65 years range). The predominant risk factor was heterosexual unprotected sex (73.1%, 38/52), followed by 17.3% (09/52) men who have sex with men (MSM). One injecting drug user, one vertical transmission patient (14 years old), and one blood transfusion case were also included. One of the patients was from the Karajás indigenous tribe (600 inhabitants) from Northern Brazil, 19 patients lived in Palmas City, and the rest came from smaller rural cities from Tocantins State. The median of the CD4 cell counts (n=51) was 380 cells/μl (25–1082 cells/μl range) and the median of PVL (n=50) was 26,605 copies/ml (553–307,834 copies/ml); for one patient the CD4 cell count was not available and for two patients PVL were missing. Almost half of the patients (24/50) had a PVL between 10,000 and 100,000 copies/ml, 12 patients had a PVL below 10,000 copies/ml, and 14 patients had a PVL above 100,000 copies/ml.
According to the SDRM-2010 database, 11.5% (06/52) (CI 95%, 4.4–23.4%) of the isolates presented transmitted drug resistance. The individual mutation profiles of naive patients with transmitted resistance to ARV are depicted in Table 1. Resistance mutations detected were associated with only one class of ARV drug. Three patients presented mutations associated with NNRTIs, two patients had mutations associated with NRTIs, and one patient had mutation associated with PIs. The median age of naive patients with resistance mutations was 30 years (21–42 years range); the median CD4 count was 413 cells/μl (244–611 cells/μl) and the median PVL was 48199 copies/ml (5361–141,124 copies/ml range).
PI, protease inhibitors; NRTI, nucleoside reverse transcriptase inhibitors; NNRTI, nonnucleoside reverse transcriptase inhibitors; PVL, plasma viral load; Hetero, heterosexual; MSM, men who have sex with men; M, male; F, female; ABC, abacavir; ATV, atazanavir; AZT, zidovudine; ddI, didanosine; DLV, delavirdine; d4T, stavudine; EFV, efavirenz; ETR, etravirine; FPV, fosamprenavir; IDV, indinavir; LPV, lopinavir; NFV, nelfinavir; NVP, nevirapine; TDF, tenofovir.
Most HIV-1 pol sequences analyzed (86.5%, 45/52) clustered with one subtype in the PR and RT regions: 78.8% (41/52) were assigned subtype BPR/BRT, 5.8% (03/52) were subtype CPR/CRT, and one patient was subtype F1PR/F1RT (Fig. 1). Seven clusters of HIV-1 subtype B isolates with high support values (>70%) were observed among naive patients. Seven isolates (13.5%) had discordant HIV-1 subtypes in the PR and RT regions and BF1 and CF1 recombinations were confirmed by bootscanning analysis (Fig. 2): BPR/F1RT (n=1), BPR/BF1RT (n=4), and CPR/CF1RT (n=2). In the phylogenetic analysis the two CPR/CF1RT isolates also represented a cluster with high support value (data not shown). All six HIV-1 isolates with transmitted resistance were HIV-1 subtype B. Figure 3 summarizes the HIV-1 genetic diversity among naive patients from Tocantins State.
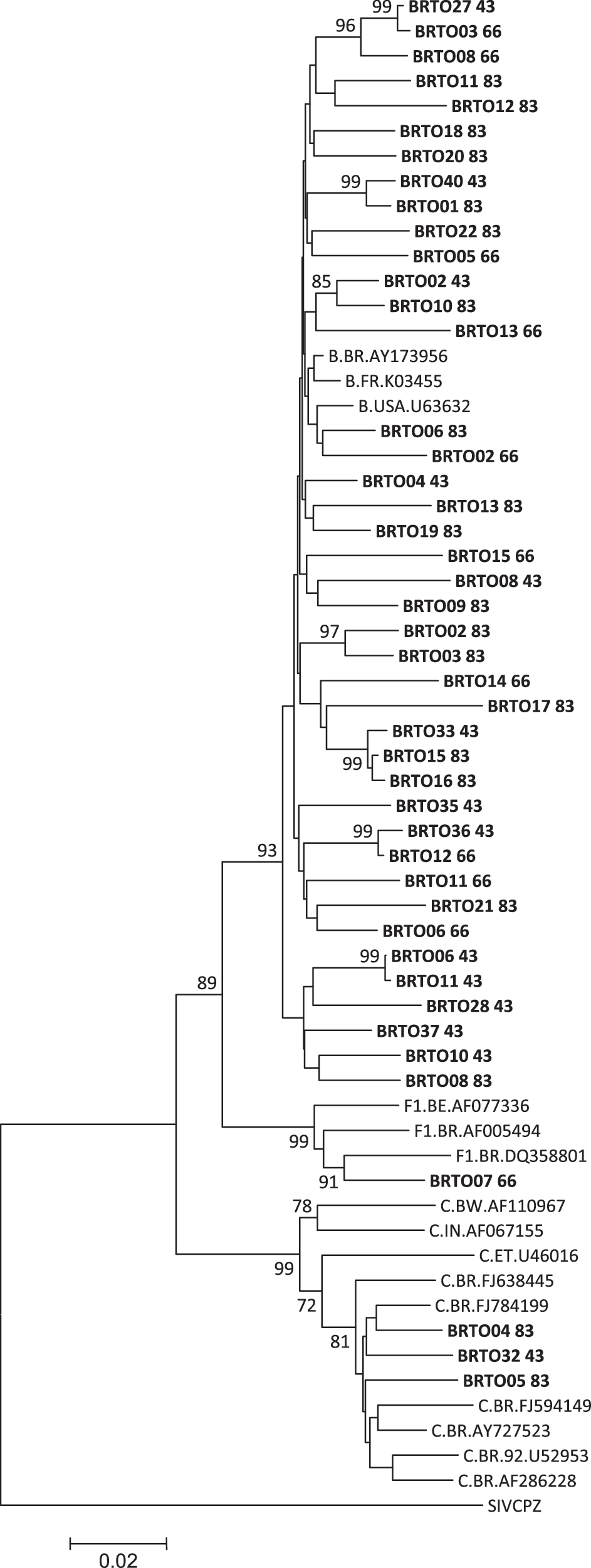
Phylogenetic analysis of HIV-1 isolates in the protease (PR) and reverse transcriptase (RT) regions. The GenBank accession numbers used in the comparative phylogenetic analysis are subtype B: AY173956, K03455, and U63632; subtype C: FJ594149, FJ638445, FJ784199, AY727523, U52953, AF286228, AF110967, U46016, and AF067155; subtype F1: AF077336, AF005494, and DQ358801, and the simian immunodeficiency virus sequence from chimpanzee (SIVcpz): X52154. Sequences from Tocantins State are in bold.

Bootscanning analysis of HIV-1 pol sequences of two of six recombinant viruses from Tocantins State. The GenBank accession numbers used in the analysis are subtype A: AF004885; subtype B: AY173956 and K03455; subtype C: U52953 and AF286228; and subtype F1: AF077336 and AF005494.
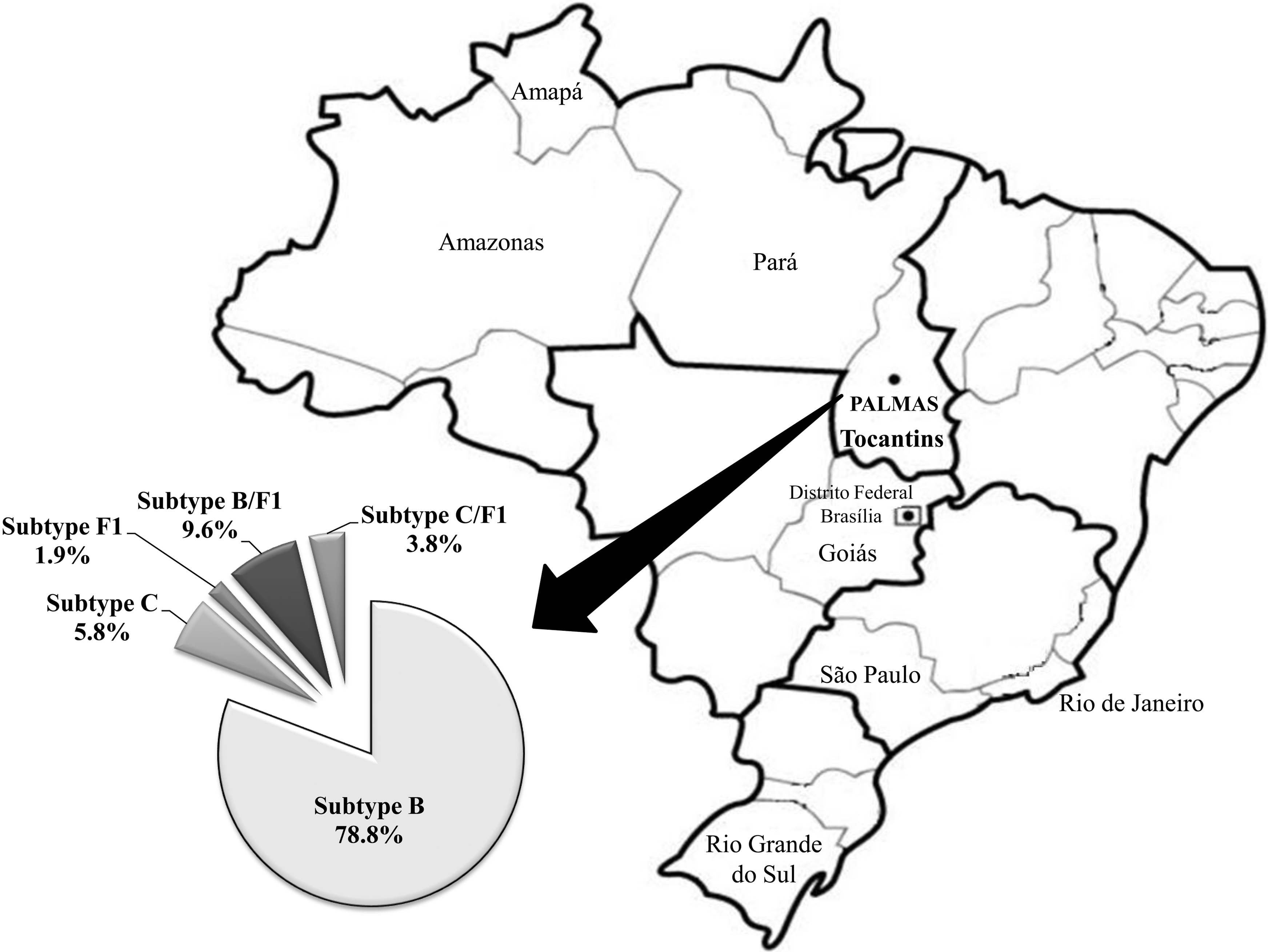
Summary of the HIV-1 subtypes identified in the PR and RT regions among naive antiretroviral patients from Tocantins State, indicated on the map of the Brazilian territory.
Discussion
The diverse Brazilian AIDS epidemic that started in the southeast has reached small cities throughout the country. Not much is known about the prevalence of transmitted drug resistance and the HIV-1 genetic forms circulating in inner smaller cities. This study adds important molecular data about the AIDS epidemic in the newest State capital in Brazil, Palmas City, located in the lowest populated and less industrialized Northern region. So far only three studies have described the molecular epidemiology of HIV-1 in Northern Brazil. 20 –22 This is the first report about the molecular characteristics of the epidemic in Tocantins State, North Brazil. In this setting we observed a moderate level of transmitted drug resistance, similar to observed in other larger metropolitan cities. Moreover, extensive HIV-1 genetic diversity, including distinct recombinant forms, was observed.
This study represents a unique opportunity to describe the molecular characteristics of the HIV-1 epidemic in a new, diverse, and growing setting in inland Northern Brazil such as the recruiting site. Palmas, a new planned city, built in an area that belonged to several farms, is still known as the “capital of opportunities” attracting thousands of migrants from all over the country. In this study half of the patients lived in the capital and the rest came from smaller cities. Although Palmas is only two decades old, most of the other cities in the state date back to the Portuguese colonial period when missionaries from the North and gold seekers from the South arrived and settled. Tocantins State is also the home of some indigenous reservations such as “Karajás Tribe,” from which one the patients, reporting heterosexual risk exposure, came. Sexual relationships with prostitutes from neighboring villages are frequently observed among male indians in Brazil. Nevertheless, the possibility of homosexual practices cannot be excluded for this male indian. 22 We have not investigated the prevalence in this tribe, but a low prevalence of HIV-1 infection has been reported in other tribes from the North Amazon region. 29 –31 A screening study among 155 native indigenous individuals from “Tiriyo Tribe” in the Amazon region showed one male individual infected with HIV-1. 21 The possibility of transmission/dissemination of HIV-1 by this male Karajá indian to his sexual partner(s) within and outside the tribe needs to be pointed out. This issue highlights the importance of assessing and monitoring the prevalence of sexually transmitted infectious diseases, such as AIDS, within unprotected, culturally distinct, and threatened indian communities in remote areas of Brazil to preserve their fertility and life span.
This study reported a moderate level of transmitted drug resistance in this inland city in Northern Brazil (11.5%) similar to rates observed in most studies in the country and in developed nations among recently infected individuals. 32 We believe that the prevalence of transmitted resistance found in Palmas was influenced by migrants infected with HIV-1 who came from larger metropolitan areas characterized by a longer exposure to ARV drugs and higher prevalence of transmitted resistance. The first Brazilian survey in 2001, which showed 6.6% transmitted drug resistance, included 17 samples from Pará State in the Northern region but no resistance mutation was detected. 6
More recent Brazilian multicentric studies reported levels of transmitted drug resistance ranging from 5.7% (95% CI, 4.4–9.6%) to 8.1% (95% CI, 4.8–12.6%) among patients, especially from the biggest metropolitan cities. 8,9 The study showing 5.7% transmitted drug resistance included 387 naive patients from 13 Brazilian cities, mainly from the South/Southeast. 9 The other recent multicentric survey reported 8.1% transmitted drug resistance among patients from the six most populated state capitals in Brazil (São Paulo, Rio de Janeiro, Salvador, Porto Alegre, Brasília, and Belém). In this study, the data from Belém/Pará state in the North and from Brasília in the Central West were analyzed together and three resistant cases were reported. 8 In Recife, Northeast Brazil, 3.6% transmitted drug resistance was observed in patients recruited between 2003 and 2004. 33 A recent study from Goiás State, from which Tocantins State was split, showed 8–10% transmitted drug resistance among naive patients. 7 Although most studies have indicated stable low to moderate levels of transmitted drug resistance in Brazil, high levels were reported in some settings. 34,35 Altogether, these data highlight the need for continued surveillance studies concerning transmitted drug resistance throughout the country, especially in a new, fast growing city such as Palmas.
The first molecular epidemiology data from Northern Brazil described equal proportions of HIV-1 subtypes B and F and 45.16% mosaic forms of subtypes B, C, and F among 31 infected individuals who attended a Counseling and Testing AIDS Center in Manaus, Amazon State. 20 In patients from Belém/Pará State and Macapá/Amapá State in Northern Brazil C2V3 and PR sequences showed a predominance of HIV-1 subtype B, the circulation of subtype F, the introduction of subtype D, CRF02_AG, and several possible recombinant forms. 22 Our study showed in addition to the predominance of HIV-1 subtype BPR/RT, the circulation of HIV-1 subtype CPR/RT, which prevails in Southern states, and one patient infected with subtype F1PR/RT. Similar to what has been described in the Southern states, a significant proportion of isolates (∼14%) was recombinant viruses mostly including subtypes B and F1. Additionally, another recombinant profile CPR/CF1RT, including two subtypes that are not prevalent, was also detected in two naive patients. Because the prevalence of subtypes F1 and C was low in this setting, it is more likely that these recombinants, especially the CF1 forms, were imported from larger metropolitan cities. In Southern Brazil subtypes F1 and C cocirculate at a higher frequence and have a greater opportunity to cause coinfection or superinfection and generate recombinant forms. Overall, our molecular epidemiology data suggest the influence of an epidemic from the South/Southeast characterized by the introduction and dissemination of several subtype B clusters locally. Additionally, one cluster represented by the two CPR/CF1RT isolates was also identified.
The native indigenous patient from Karajás Tribe described in the current study was infected with HIV-1 subtype B, confirming the introduction and circulation of this subtype among indians in Northern Brazil, similar to what was found in the Tiriyo tribe. 21 The first HIV-1 subtype C sequences from Tocantins State formed a monophyletic cluster with other subtype C sequences from the remote Southern region indicating the impact of this region on the epidemic in Northern Brazil. Overall, the molecular epidemiology results from Tocantins State indicate complex genetic patterns similar to what has been described in major metropolitan regions, suggesting the influence of imported recombinant viruses in the epidemic, especially in the recently founded city of Palmas.
Although a relatively small sample size was investigated, this study group represented around 40–50% of ARV-naive patients from this area in that period (personal communication) as both the incidence of HIV-1 infection and the demographic density in this setting are low. Another potential limitation of the study could be undisclosed previous ARV use, if any participant did not report prior treatment. Although this cannot be completely ruled out, evidence that reinforces the contention that the included patients were indeed ARV naive was the absence of dual-triple class drug resistance-associated mutations, which would be expected in ARV-experienced subjects as defined by the International Aids Society (IAS-USA). 36
Although we do not know the date of infection of these naive patients studied, considering the CD4 cell counts, most of them were chronically infected individuals. Recently infected subjects may be more likely to harbor resistance mutations than subjects infected for 1 year or more. However, certain resistance-associated mutations may persist for months or years after detection in ARV-naive individuals, presumably because these mutations do not confer a significant fitness disadvantage to the virus. Resistance-associated mutations with little or no impact on viral fitness can be detected in virus from ARV-naive individuals (or in individuals who have interrupted therapy) for longer periods of time than mutations that impose a great fitness cost to the virus. 37 Transmitted NNRTI resistance-associated mutations represent the best studied of these mutations, and some studies suggest that some of these mutations can persist for years postinfection in untreated, HIV-infected patients. 38 In our study group decreased NNRTI susceptibility predominated among the three drug classes. Mutations that tend to be less stable in the absence of drug selection pressure, and that predominate in newly infected or newly treated patients such as M184V and K65R, were not observed. Seven HIV-1 isolates from this study presented potential low-level resistance mutations (T74S, Q58E, L33F, and V179D/E); however, these mutations do not have clinical significance.
Overall, this survey in Tocantins State, Northern Brazil, indicates a dynamic and complex HIV-1 epidemic suggesting a strong influence of imported cases from the South/Southeast together with several clusters of internal HIV-1 dissemination. In this fast growing setting in a geographically remote area, continuous studies should monitor HIV-1 genetic diversity and transmitted resistance, which should indicate whether these patients might benefit from pretreatment genotypic tests.
Sequence Data
GenBank accession numbers of the sequences presented in this study are GU214066–GU214102, GU214111, and HM583573–HM583586.
Footnotes
Acknowledgments
This study was supported by UNESCO AIDS/STD National Program, Brazilian Ministry of Health (Grant 310-06). M.M.A. Stefani is a recipient of a fellowship from The National Counsel of Technological and Scientific Development/CNPq (Grant 304869/2008-2), B.C. Carvalho was supported by a scholarship from CAPES, and L.P.V. Cardoso (Grant 141820/2006-3) was supported by a scholarship from CNPq.
Author Disclosure Statement
No competing financial interests exist.