
Abstract
Serological assays are increasingly being used to measure HIV incidence in cross-sectional studies, but their specificity to determine incident infections remains problematic. We estimated the specificity of the BED assay in a cohort of long-term HIV-infected adults before and during antiretroviral treatment (ART) and evaluated an HIV avidity assay to detect BED-based false-recent results. We used the BED assay to test stored specimens from known long-term HIV-1-infected adult Ugandans before and at 3, 12, and 24 months after ART initiation. We evaluated the frequency of false-recent classifications by ART status and CD4+ T+ cell count. Specimens classified as BED false-recent were further tested with an avidity assay. In all, 950 blood specimens from 253 adults were tested with the BED assay. Of these, 149 (15.7%) specimens tested false-recent and 64 (24.9%) individuals tested false-recent at least once. Among all specimens tested, the proportion of false-recent rose with increasing CD4+ cell count (<250 cells/μl: 11.3%, 250–499: 17.8%, ≥500: 21.4%; p for trend=0.002). Of 197 persons with all four BED results available, 75.6% were classified as long-term infected throughout and 8.1% as false-recent throughout; the remainder changed classification once (12.2%) or twice (4.1%). Of 105 false-recent specimens retested with the avidity assay, 101 (96.2%) were correctly classified as “long-term.” The BED assay's specificity varied with CD4+ cell count and use of ART. Knowledge of these parameters for blood samples could improve incidence estimates using the BED assay. The additional use of an avidity assay may help to minimize the proportion of BED false-recent specimens.
Introduction
W
One of the most widely used serological incidence assays is the BED IgG capture immunosorbent assay 1,2 that detects recent HIV infections occurring within a mean of 197 days [95% confidence interval (CI) 173–220] with a separate estimate of 236 days for subtypes A/D/G in Africa. 3 However, the use of the BED assay is, as for others, impeded by suboptimal specificity to determine incident infections. 4,5 The reliability of this assay may be particularly poor when applied to persons taking antiretroviral treatment (ART) and yet the ART status of persons is not always known, particular in resource-constrained settings. We evaluated the reliability of the BED assay in known long-term HIV-infected but ART-naive adult Ugandans before and during 2 years of ART. We also investigated the utility of a second serological HIV incidence assay, an avidity-based assay, 6 as an additional test to detect BED-based false-recent HIV results.
Materials and Methods
Specimens and data
Patient specimens and data originated from two consecutive care and treatment studies in rural Tororo and Busia Districts, Eastern Uganda. The first study commenced in April 2001 and evaluated the effect of a home-based safe water system (SWS) and cotrimoxazole prophylaxis on the morbidity and mortality in HIV-infected but ART-naive individuals. All selected individuals were known to be HIV-infected longer than 9 months with a median time since the first available HIV-positive result of 2.4 years [interquartile range (IQR) 1.1–4.0, range 0.8–11.1]. In 2003, the Home-Based AIDS Care (HBAC) study was initiated in the same area and offered enrollment to all ART-eligible SWS study participants. HBAC's primary objective was to compare different clinical ART monitoring strategies. SWS and HBAC study data included demographic, behavioral, and laboratory parameters. Blood was drawn regularly over time from SWS and HBAC participants and transported to the Centers for Disease Control and Prevention (CDC) in Entebbe for testing; plasma was stored at −80°C. For the purpose of this analysis, we selected all study participants from whom specimens were available during both their SWS and HBAC participation. From these specimens, we selected the last available SWS plasma specimens (pre-ART) as well as HBAC plasma collected 3, 12, and 24 months after ART initiation.
Both studies from which the selected specimens originated as well as the additional testing for the study described here were reviewed and approved by the institutional review boards of the Ugandan Virus Research Institute and the CDC in Atlanta, Georgia.
Laboratory methods
All testing for this analysis was performed at the CDC laboratory in Entebbe, Uganda. Most HIV infections in Uganda are subtype A and D 7 ; however, we did not determine our study participants' HIV subtypes. The CD4+ cell counts were determined with TriTest reagents on a FACSCan instrument (Becton Dickinson, Franklin Lakes, NJ). Viral load was measured using Cobas Amplicor HIV-1 Monitor (Roche Diagnostics, Mannheim, Germany). Viral load values <400 copies/ml were classified as undetectable and values of 400 or above were classified as detectable. All selected plasma specimens were tested between April and August 2006 with the BED IgG capture immunosorbent assay (Calypte Biomedical Corporation, Lake Oswego, OR) according to the manufacturer's guidelines. Specimens with a BED optical density (OD) ≥1.2 were classified as long-term HIV infected. Specimens with an initial BED OD <1.2 were retested in triplicate.
Because all study participants were known to be long-term (i.e., longer than the BED assay's recency duration) HIV-1-infected, specimens that tested with a mean OD <0.8 were then classified as false-recent (false-positive), whereas those with ODs ≥0.8 were classified as (true) long-term infected. BED false-recent specimens were then further tested with the avidity assay using modified Genetic System rLAV EIA from Bio-Rad (Redmond, WA), using the manufacturer's guidelines and controls, with a dissociation step added to a duplicate well. Specimens were incubated in two microwells and allowed to bind antigen. After 1 h of incubation, a dissociating agent, potassium thiocyanate (2.5 M KSCn), was added to one well and further incubated at room temperature for 15 min, allowing low-affinity HIV-1 antibodies to dissociate. An avidity index (AI) was then calculated by dividing the OD of the well containing the dissociating agent by the OD of the untreated well, multiplied by 100. Specimens with an AI of ≤80 were classified as recent (with an estimated recency duration of ∼180 days); those with an AI of >80 were classified as long-term. 8
Data analysis
Data were analyzed using Epi Info v6.04 (CDC, Atlanta, GA) and Microsoft Excel. We determined the proportion of specimens testing BED false-recent prior to ART initiation as well as 3, 12, and 24 months post-ART initiation. Furthermore, we evaluated the association between BED test result and CD4+ count, ART duration, and viral load. Lastly, we determined the proportion of BED false-recent specimens that the avidity assay could correctly classify as true long-term HIV infection.
Results
BED reactivity
We tested 950 specimens collected from 253 individuals: 226 specimens were drawn prior to ART initiation, 252 were collected at 3 months after ART initiation, 249 specimens at 12 months post-ART, and 223 specimens at 24 months post-ART. Table 1 shows the various patterns of BED reactivity within the same individuals over time. Overall, 149 (15.7%) specimens tested false-recent by the BED assay and 64 (24.9%) individuals tested false-recent at least once. Of 197 individuals for whom all four test results were available, 16 (8.1%) tested false-recent throughout, 24 (12.2%) changed their BED status once, and 8 (4.1%) changed their BED status twice.
L, long-term HIV infection; R, false-recent HIV infection. The first letter in all cases denotes the pre-antiretroval treatment (ART) specimen. Result patterns shorter than four letters indicate missing ART specimens.
Figure 1 depicts the association between BED test result, ART status, and CD4+ cell count. The proportion of specimens testing false-recent was similar pre-ART and 3 months post-ART initiation but then increased with increasing time on ART (pre-ART: 12.4%, 95% CI 8.4–17.4%; ART 3 months: 11.9%, 95% CI 8.2–16.6; ART 12 months: 15.3%, 95% CI 11.0–20.3%; ART 24 months: 23.8%, 95% CI 18.3–29.9%). Among all specimens tested, the proportion testing false-recent increased with increasing CD4+ cell count (<250 cells/μl: 11.3%, 250–499: 17.8%, ≥500: 21.4%; p for trend=0.002). A similar trend was seen for pre-ART specimens only, but was not significant (p for trend=0.189).
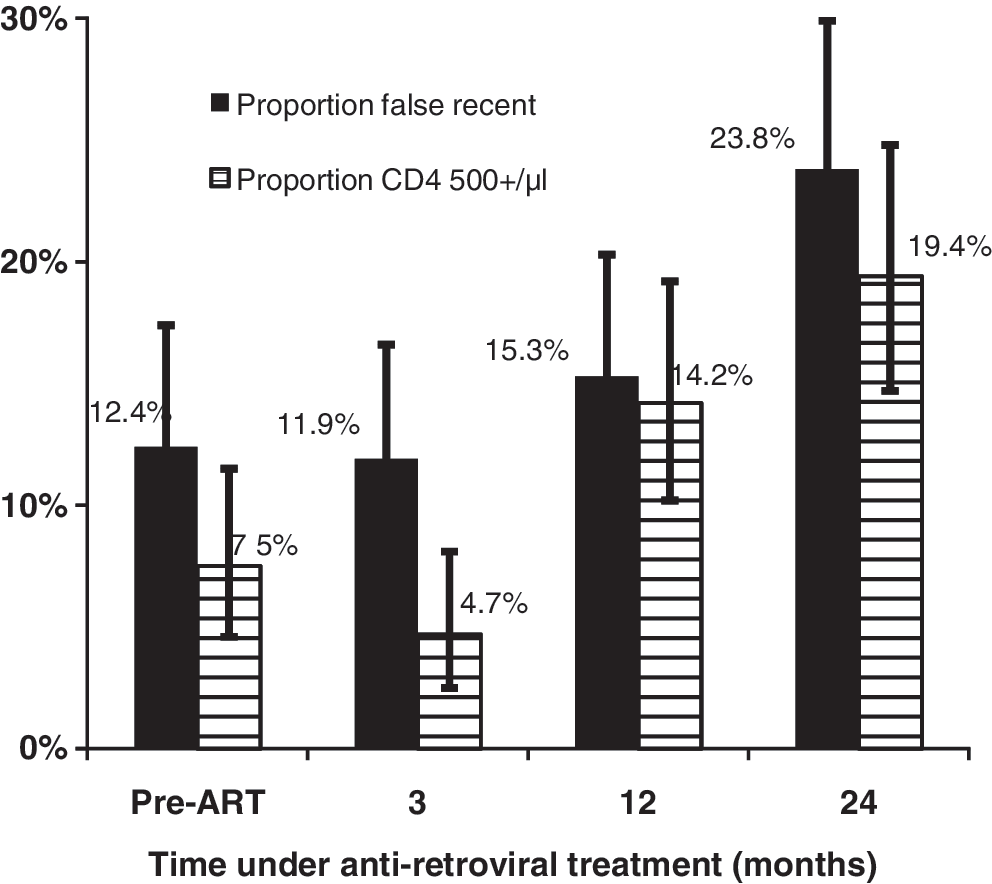
Association between BED test result, ART status, and CD4+ cell count.
Viral load data were available for 945 specimens originating from all four time points (pre-ART, 3, 12, and 24 months post-ART initiation). The proportion of specimens with undetectable viral load was 1.6% (pre-ART), 92.5% (3 months on ART), 95.2% (12 months on ART), and 97.2% (24 months on ART). Overall, 687 (72.7%) specimens had undetectable viral load and a total of 147 (15.6%) specimens were classified as BED false-recent. Specimens with undetectable viral load were more likely to test BED false-recent (17.0%) than specimens with detectable viral load (11.6%, p=0.04). When analysis was stratified by time of testing, the same association between viral load and BED false-recency was observed but was not significant at two time points whereas at each of the remaining two time points one cell value was zero.
Of the 149 BED false-recent specimens, 105 (70%) were available for further testing with the avidity assay; the remaining specimens were exhausted. Only one specimen tested by the avidity assay was drawn pre-ART; all other avidity-tested specimens originated from participants under ART. Of the 105 specimens tested, 101 (96.2%) were correctly classified as long-term, while the remainder (n=4, 3.8%) were again classified as false-recent. Overall, the median AI was 99.9 (IQR, 97.1–101.0; range 62.2–106.1). Among AI false-recent specimens, the median AI was 74.4 (IQR, 65.8–79.7; range 62.2–79.9); among AI long-term specimens, the median AI was 100.0 (IQR, 97.3–101.1; range 80.8–106.1). After additional testing with the avidity assay, the combined rate of false-recency was 0.4% (4/906, removing 44 exhausted specimens that could not be tested with the avidity assay).
Discussion
We tested known long-term HIV-infected Ugandan adults with the BED assay and evaluated the utility of an avidity-based assay to identify BED false-recent specimens. Approximately 16% of all specimens were classified false-recent by the BED assay. Prior to ART initiation, some 12% of individuals were classified false-recent, and a similar proportion tested false-recent soon after ART initiation. Although the sample sizes in our study were relatively small and the resulting CIs were therefore wide, there was a trend of decreasing BED specificity in patients with increasing CD4+ counts and time on ART. Specimens with undetectable viral load were more likely to test BED false-recent than specimens with detectable viral load. The Bio-Rad-based avidity assay correctly categorized the majority of BED-misclassified specimens as belonging to long-term infected individuals.
The advent of serological incidence assays in the past decade heralded a new era for HIV surveillance. Their main advantages are compelling–a relatively large “window” period and their applicability to cross-sectional samples. The BED assay recently facilitated the generation of revised HIV incidence estimates in the United States 9 and risk factors for HIV acquisition in a large population-based survey sample in Uganda. 10
Our study design allowed the examination of the BED assay's reliability and the Bio-Rad avidity assay's ability to identify only BED false-recent test results. Our study did not examine the Bio-Rad avidity assay's sensitivity, i.e., its ability to accurately identify recent HIV infections. Hence, before applying a serial BED Bio-Rad testing algorithm to identify recent HIV infections and “screen out” long-term infections, validation of the reliability of the Bio-Rad assay as well as that of a combined BED-avidity index-based algorithm is warranted. Such validation work is ongoing in various parts of the world, 8,11 including Africa. 12,13 Furthermore, only the minimum duration of HIV infection—based on the earliest known date of an individual's HIV-positive test result—was known. It is likely that most individuals' HIV infection was acquired substantially earlier than their first known HIV-positive test result, as all our study participants initiated ART soon after the date of their pre-ART specimens used in this study.
BED-based incidence estimates are usually computed using a standardized algorithm that adjusts the raw incidence data for the assay's imperfect specificity and sensitivity 1 or specificity alone. 14 The McDougal formula assumes a long-term false-recent rate of 5.6%. In comparison, the proportion of pre-ART specimens testing (long-term) false-recent in our sample was 12.4%. Such differences may help explain why the BED assay in this geographic region may produce higher than expected HIV incidence rates. 5 Indeed, the utility of the BED assay alone to evaluate HIV incidence rates appears limited in regions with low assay specificity unless measures are available to reliably identify patients with advanced HIV disease.
The BED assay's OD depends on the ratio of anti-HIV IgG to total IgG. Our observation that the proportion of individuals testing BED false-recent increased with time taking ART might be explained by the continuing decline of anti-HIV IgG levels with ongoing viral load suppression over the first 24 months of ART. The proportion of individuals under ART testing BED false-recent in our study (rising from 11.9% to 23.8%) is substantially smaller than reported in the study by Hayashida et al. in which five of seven (71%) patients on ART for >2 years tested BED false-recent, 15 or that by Marinda et al. (56% false-positive by 2 years on ART). 16 This large difference may be due to chance (small numbers in Hayashida et al.) or indicate that the trend of decreasing specificity with increasing time on ART continues beyond 24 months. The BED assay is not supposed to be applied to samples from persons taking ART and the commonly used statistical adjustment formulas do not account for false-recent results due to ART. Our results confirm that samples for which individuals are not confirmed ART naive may contribute to an overestimation of HIV incidence and that with increasing time on ART this overestimation increases. Documenting non-ART experience of sampled individuals will therefore become more important over time and the temptation to apply the BED and possibly other incidence assays to stored samples with poor accompanying data may pose a corresponding hazard.
The literature reports the evaluation of several serological incidence assays, 17 –20 none of them yet reaching satisfactory performance characteristics for incidence estimation. The addition of the avidity assay in our study greatly reduced the proportion of BED-based false-recent classifications, very similar to another study in Uganda. 17 Combining incidence assays in algorithms whereby specimens are classified as “recent” if classified as such by more than one assay may increase the specificity but introduces additional complications. The use of combined incidence assays with different recency periods would warrant the re-estimation of the resulting algorithms' recency durations. Study participants who are tested within the recency period of one assay but outside that of another assay would thus be classified as long-term infected thereby decreasing the estimated number of recently infected individuals. However, in our study, all individuals were known to be infected for more than 9 months (and likely substantially longer than that) so that this situation did not arise here.
Although the Bio-Rad assay performed well in this sample it should be mentioned that this assay uses subtype B antigen and its performance on non-subtype B infections may be variable. Furthermore, this assay has yet to be formally calibrated and validated against observed HIV-1 incidence.
Assays to estimate HIV incidence cross-sectionally are powerful tools for surveillance and the evaluation of HIV prevention efforts. Research to improve the accuracy of these assays and the establishment of appropriate algorithms should be a priority. 21
Footnotes
Acknowledgments
We thank Prosper Behumbiize for assistance with data management and Bharat Parekh and Andrea Kim for advice on laboratory testing and interpretation. All authors substantially contributed to the study's design and conduct, or to data analysis and interpretation. All approved the final version for publication. The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the CDC or the U.S. Department of Health and Human Services.
Author Disclosure Statement
No competing financial interests exist.