
Abstract
The prevalence of HIV-1 drug resistance mutations (DRMs) was determined for a cross-section of individuals (n=8654) in five centers across Vietnam (Hanoi, Hai Phong, Da Nang, Khanh Hoa, and Can Tho) between 2008 and 2009. Following serological screening for HIV infection, HIV-1 viral load was determined, using an in-house real-time reverse transcriptase polymerase chain reaction (RT-PCR) assay. Samples with quantifiable viral loads [all either commercial sex workers (CSW) or intravenous drug users (IDU)] underwent DRM analysis. Sequences were obtained for 92 treatment-naive individuals, the majority of whom were infected with HIV-1 CRF01_AE (99%), with one instance of subtype A1 also detected. DRMs were detected in seven treatment-naive individuals (7.6%). The most common DRMs observed were M184V, V75A/M, M41L, and K65R (NRTI) and K103N, G190A, and Y181C (NNRTI). Overall, the data from this first multicenter survey of DRMs in Vietnam indicate that the problem of transmitted drug resistance is of major concern in the highest-risk groups of IDU and CSW.
I
The rapid roll-out of ART into the resource-limited context of Vietnam may, however, be accompanied by the emergence of antiretroviral drug resistance mutations (DRMs). A number of previous studies have examined the rate of DRMs in HIV-1-infected individuals. One of the earliest, carried out in Ho Chi Minh City (HCMC) in 2003, found DRMs in 6.5% of treatment-naive individuals. 4 DRM rates of less than 5% have been reported by studies carried out in and around Hanoi, Hai Phong, and also in a more recent report from HCMC. 5 –7 The most recent data published for Hanoi indicate a DRM rate of 6.2% in untreated individuals. 8
The WHO guidelines for monitoring the emergence of HIV-1 drug resistance in resource-limited settings, such as Vietnam—so-called “threshold surveys”—involve the monitoring of a comparatively restricted cohort of individuals (specifically, people under 25 years old, and, if pregnant, experiencing their first pregnancy) and within a limited geographic range. However, it is generally accepted that the HIV-1 epidemic in Vietnam is concentrated in high-exposure risk groups such as commercial sex workers (CSWs) and injecting drug users (IDUs). 1 The aim of the current study was to determine the prevalence of HIV-1 DRMs in a cross-section of Vietnamese individuals, recruited at a number of collection centers, and examining not only these high-risk groups, but also low-exposure risk individuals. This investigation represents part of a larger epidemiological study of blood-borne viruses, carried out under the auspices of the Ireland–Vietnam Blood-Borne Virus Initiative (IVVI), established as a collaborative partnership between the National Virus Reference Laboratory (NVRL) in Ireland and the National Institute of Hygiene and Epidemiology (NIHE) in Vietnam, with the aim of developing institutional capacity and infrastructure for clinical and diagnostic virology in that country.
Plasma and serum samples were collected from 8654 individuals with various exposure histories—CSWs, IDUs, blood donors, military recruits, pregnant women, dialysis patients, elective surgery patients, and recipients of multiple blood transfusions. Recruitment was carried out between 2008 and 2009 in five centers across Vietnam: Hanoi (n=1750) and Hai Phong (n=1750) in the North, Da Nang (n=1750) in the Central region, and Khanh Hoa (n=1725) and Can Tho (n=1679) in the South. All samples and information were obtained anonymously and ethical approval was obtained from the National Institute of Hygiene and Epidemiology (NIHE). The Genscreen HIV Ag-Ab serological screening kit (Bio-Rad) was used to determine the prevalence of HIV infection.
Recruited individuals were surveyed at the time of sample collection and individuals self-reporting prior experience of ART were separated into cohorts reporting no prior ART exposure (“Naive”) or those with prior experience of ART (“Treated”) before further molecular analyses. Viral RNA was manually extracted from 500 μl of selected HIV-1-seropositive plasma samples using the QIAamp Viral RNA kit (Qiagen); following an ultracentrifugation step (22000 g for 80 min), the pellet was lysed and RNA extracted as per the manufacturer's protocol. HIV-1 viral load (VL) was determined using an in-house real-time reverse transcriptase polymerase chain reaction (RT-PCR) assay using primers and probes previously published by Drosten et al. 9 The assay utilizes in-house, plasmid-derived HIV-1 RNA standards, brome mosaic virus (BMV) RNA (1 pg/sample) as an internal quality control, 10 and the Superscript III Platinum Taq One Step RT-PCR kit (Invitrogen), running on the ABI 7500 FAST real-time platform (Applied Biosystems). The assay was validated with a 95% limit of detection of 180 copies/ml plasma (2.26 log10 c/ml) and a linear dynamic range of 180–1×108 copies/ml (2.26–8.00 log10 c/ml). Samples with quantifiable viral loads were further examined for the presence of DRMs using the ViroSeq HIV-1 Genotyping System (Abbott) or the TRUGENE HIV-1 Genotyping Platform (Siemens), according to the respective manufacturer's instructions. The sensitivity of the ViroSeq assay was improved by using a modification of the ViroSeq protocol incorporating a nested PCR amplification step. Codons 4–98 of the protease (PR) and codons 38–248 of the reverse transcriptase (RT) regions of the HIV-1 pol gene were analyzed for the presence of DRMs using the software provided with the respective genotyping platforms.
Additional DRM analysis and genotype determination was performed using the Stanford University online sequence analysis tool (
Of the 8654 individuals screened for HIV infection, 471 tested positive for HIV by serology. Unsurprisingly, the bulk of this HIV burden was attributed to the IDU (309) and the CSW (147) cohorts. HIV prevalence among the low-exposure risk study groups (one HIV-positive individual in the elective surgery group, two HIV-positive individuals in each of the dialysis patient, military recruit, blood donor, and multiple blood transfusion recipient groups, and six HIV-positive pregnant women) came to 0.2%, below the estimated prevalence of HIV in the general Vietnamese population of 0.5%, although that estimate does include both high- and low-risk individuals. 1 Of the 471 HIV-seropositive individuals, 234 (166 treatment-naive, 68 treated) were examined further for plasma viral load (Table 1), including all 15 low-risk seropositive individuals and a random sampling of the CSW and IDU groups. HIV-1 RNA was detected in 122 of 166 treatment-naive samples (73.5%; all IDUs or CSWs). Twelve samples had detectable HIV-1 RNA below the 180 copies/ml assay quantification cut-off; viral loads were calculated for the remaining 110 samples (median 3.99 log10 copies/ml; range 2.30–5.67). Likewise, 28 of 68 specimens from treated individuals (41%; all IDUs or CSWs) contained detectable HIV-1 RNA. Eight samples contained detectable HIV-1 RNA below the linear dynamic range of the assay, while the 20 quantifiable samples yielded a median viral load of 3.89 log10 copies/ml (range 2.33–4.76). Surprisingly, none of the 15 low-risk individuals had a detectable HIV-1 viral load.
Calculated for samples with VL >2.26 log10 copies/ml (LoD).
LoD, limit of detection; VL, viral load.
Sequence data were obtained for 106 HIV-1 RNA-positive specimens (92 naive, 14 treated). As determined by the Stanford sequence analysis tool, the majority of individuals were infected with the CRF01_AE subtype, well established as the predominant HIV-1 subtype in Vietnam, 13 but, for the first time in Vietnam, one case of infection with HIV-1 subtype A1 (1%) was also detected, in a CSW from Hanoi. A total of 16 major and four minor RTI resistance-conferring mutations were detected in the treatment-naive study group, distributed among seven individuals (7.6%; Table 2).
NRTI, nucleoside reverse transcriptase inhibitor; DRM, drug resistance mutation; NNRTI, nonnucleoside reverse transcriptase inhibitor.
The most common NRTI DRM observed was M184V (n=3), with two instances each of V75A/M, M41L, and K65R also detected. Each of these mutations will confer resistance to lamivudine (3TC) or stavudine (d4T). The NNRTI resistance mutations detected included three instances of K103N (always occurring with M184V) and two individuals with both G190A and Y181C. In addition to these major resistance mutations, four minor NNRTI DRMs were also detected: P225H (n=2, occurring in the same individuals as the M184V / K103N combination), A98G, and V179D. Each of these NNRTI major or minor DRMs confers resistance to nevirapine (NVP) and/or efavirenz (EFV). In our “treated” cohort, five individuals were found to possess major resistance mutations (35.7%), and the same major NRTI and NNRTI mutations were detected, along with additional mutations conferring major (T215F/Y) and minor (D67N, L210W) resistance to NRTIs (Table 3).
Also RT polymorphism K219Q.
Also RT polymorphisms E44D, F77L, and V118I.
NRTI, nucleoside reverse transcriptase inhibitor; DRM, drug resistance mutation; NNRTI, nonnucleoside reverse transcriptase inhibitor; CSW, commercial sex worker; IDU, intravenous drug user; dHT, stavudine; 3TC, lamivudine; NVP, neviripine.
Two treated individuals in particular demonstrated a broad range of resistance mutations, along with a number of nonresistant polymorphisms (E44D, F77L, V118I, and K219Q). The profile of DRM observed corresponds well with the national guidelines for first-line ART in Vietnam, where the combinations (d4T+3TC+NVP or d4T+3TC+EFV) are the recommended treatment regimens. No major PI drug resistance mutations were found in our study cohort; however, a recent report from Hanoi identified a protease inhibitor DRM rate of 1.7%. 8 One sequence from an individual in our treated study group, but who reported no exposure to PI, contained the polymorphism M46V, a PI-selected substitution with an as yet unknown effect on PI susceptibility. Currently, the use of PI is recommended only in second-line ART regimens in Vietnam. The accessory mutation L10I/V was detected in 16.8% of all sequences obtained [15/92 naive (16.3%), 3/14 treated (21%)], a frequency comparable to that previously reported for CRF01_AE strains in Southeast Asia. 14,15
Phylogenetic analysis of the treatment-naive cohort demonstrated that our Vietnamese sequences formed several clusters, corresponding with geographic origin, although not all sequences obey this trend (Fig. 1). As previously noted, sequences from samples collected in Northern Vietnam tend to cluster with reference sequences from Southern China and, similarly, Southern Vietnamese sequences generally show greater similarity to HIV-1 isolates from Thailand. 6,8,13 No distinction could be made between the clustering of our exposure groups within the “Northern” or “Southern” clades, suggesting that infections are transmitting between the study groups. The CRF15_01B HIV-1 recombinant form combines genetic material of subtype B and CRF01_AE, and has recently been reported in Vietnam. 5 CRF15_01B reference sequences included in our phylogenetic analysis (all from Thailand) clustered with CRF01_AE strains from Thailand, suggesting that the region of the pol gene under investigation is unsuitable for discriminating between CRF15_01B and its CRF01_AE ancestral strain(s).
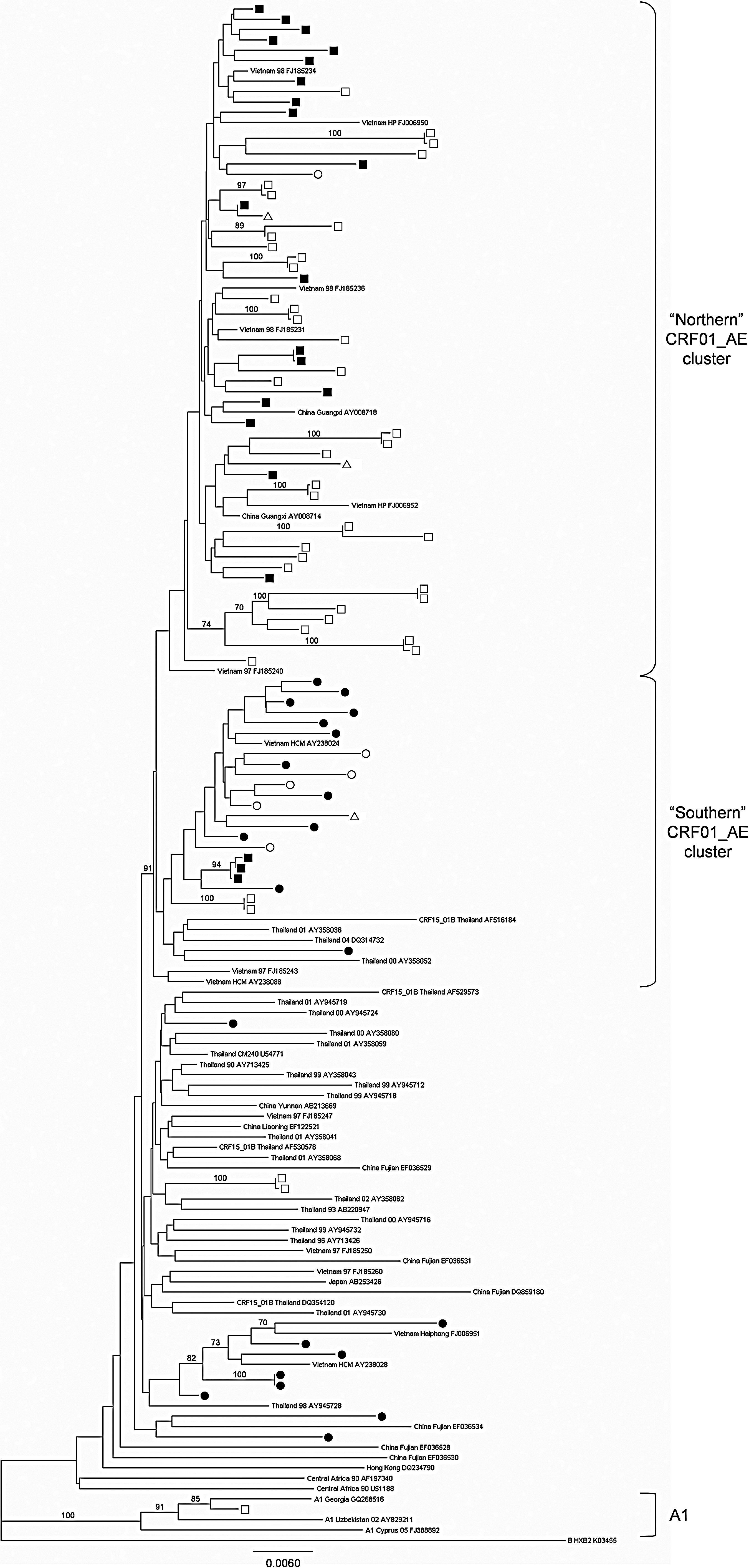
Phylogenetic tree of HIV-1 strains from 92 treatment-naive CSW/IDU from Hanoi, Hai Phong, Da Nang, Khanh Hoa, and Can Tho. The tree is based on concatenated sequences incorporating 287 bases from the pol gene protease region and 630 bases from the pol gene reverse transcriptase region (total, 917 bp). □, strains from Hanoi; ▪, strains from Hai Phong; (▵, strains from Da Nang; (○, strains from Khanh Hoa; (•, strains from Can Tho. The 92 study sequences were aligned with 57 reference sequences from the Los Alamos HIV database including 50 CRF01_AE pol sequences (22 from Thailand, 14 from Vietnam, 10 from China, 2 from Central Africa, 1 from Japan, and 1 from Hong Kong); 3 A1 sequences and the HXB2 subtype B sequence were used as an outgroup. Bootstrap values above 70% are shown.
The prevalence of antiretroviral drug resistance mutations among treatment-naive HIV-1-positive individuals, sampled between 2008 and 2009 in five centers across Vietnam, was 7.6%. This is higher than the rate previously reported in studies conducted in the North (Hanoi and Hai Phong) 5,6 and South (Ho Chi Minh City) 7 of Vietnam. DRM rates of >6% have, however, been previously reported for ART-naive patients in Ho Chi Minh City, 4 and in a more recent study from Hanoi. 8
One reason our data yielded a DRM rate higher than those rates previously published may be our use of an open recruitment policy, putting no limitations on the age or rehabilitation status of the individuals recruited, and utilizing a study population broader than that suggested by the WHO HIV Drug Resistance Threshold Survey (HIVDR-TS) protocols and including high-risk populations. 5,6 It is also possible that because our sampling and analysis are more recent than other studies, our data may indicate an upward trend in the instance of DRMs, and transmitted resistance in particular, in Vietnam. This could reflect the increased use of ART and/or the expansion of HIV infections during the study period.
As the availability of antiretroviral drugs continues to expand, but the socioeconomic restraints on drug access persist, problems may arise in accessibility to ART, particularly where the drugs are being sourced through private channels. Poor therapy adherence is also a major risk for DRMs in resource-limited settings. High exposure risk behavior among groups such as IDUs and CSWs may put them among the first to acquire these DRMs via transmission, and it is possible that this trend is reflected in our study population. However, as our therapy information is self-reported, it is possible that inaccuracies in reporting ART experience could also contribute to the differences observed herein. The present study is also unable to determine what effect, if any, the history of HIV infection and treatment in the different geographic regions investigated may have had on the observed rate of DRMs. Further studies with larger sample numbers are required to determine if there are geographic differences in DRM rates in Vietnam.
Without a common framework for study design and execution, along with shared and/or comparable methodologies, it is difficult to draw complete comparisons between this and previously published studies on the prevalence of HIV-1 DRMs in Vietnam. Although our data may indicate that the rate of DRMs is increasing in Vietnam, the data from this first multicenter survey indicate that the problem of transmitted drug resistance is of major concern in the highest-risk groups of IDUs and CSWs.
Footnotes
Acknowledgments
The Ireland Vietnam Blood-Borne Virus Initiative (IVVI) is supported by Irish Aid, the Government of Ireland's program of assistance to developing countries, and the Atlantic Philanthropies. The authors would also like to thank the staff at the Laboratory for Molecular Diagnostics at NIHE in Hanoi, and at the National Virus Reference Laboratory in Dublin.
Author Disclosure Statement
No competing financial interests exist.