
Abstract
In the combination antiretroviral therapy (cART) era, renal dysfunction remains common. The Study to Understand the Natural History of HIV/AIDS in the Era of Effective Therapy (SUN) (ClinicalTrials.gov number, NCT00146419) is a prospective observational cohort study of HIV-infected adults. At baseline, comprehensive data were collected, including cystatin C and measures of renal function. Univariate and multivariate regression analyses were performed to identify factors associated with baseline renal dysfunction [estimated glomerular filtration rate (eGFR) <90 ml/min/1.73 m2 calculated using the simplified Modification of Diet in Renal Disease equation] and elevated cystatin C (>1.0 mg/liter) in a cross-sectional analysis. Among 670 subjects with complete data (mean age 41 years, mean CD4 cell count 530 cells/mm3, 79% prescribed cART), the mean eGFR was 96.8 ml/min/1.73 m2. Forty percent of subjects had renal dysfunction; 3.3% had chronic kidney disease (eGFR <60 ml/min/1.73 m2). Elevated cystatin C was present in 18% of subjects. In multivariate analysis, renal dysfunction was associated with older age, non-Hispanic white race/ethnicity, higher body mass index (BMI), hypertension, higher cystatin C levels, and current prescription of ritonavir. Factors associated with elevated cystatin C included hepatitis C coinfection, hypertension, current smoking, older age, current tenofovir use, detectable plasma HIV RNA, and elevated microalbuminuria. The prevalence of chronic kidney disease (CKD) was low in this contemporary HIV cohort. However, mild to moderate renal dysfunction was common despite the widespread use of cART.
Introduction
In the era of combination highly active antiretroviral therapy (cART), HIV infection has evolved into a manageable chronic medical illness with reduced morbidity and mortality for patients who remain engaged in care. 1,2 During the past decade, the incidence of HIV-associated nephropathy (HIVAN), renal failure, and end-stage renal disease has declined significantly, 3 –7 primarily as a result of more widespread use of cART. However, up to 30% of HIV-infected patients have evidence of renal dysfunction. 8 Additionally, a variety of cART-related renal adverse events have been noted, including proteinuria, renal tubular damage, interstitial nephritis, and nephrolithiasis. 9 –14 Furthermore, other comorbidities such as hypertension, insulin resistance, obesity, and type 2 diabetes, which are increasingly prevalent among contemporary HIV-infected patients in care, may increase the risk for renal dysfunction over time. 15,16
In 2005, guidelines for screening and treating renal disease in HIV-infected persons were published by the HIV Medical Association of the Infectious Diseases Society of America. These guidelines recommended that all HIV-infected patients be screened annually for proteinuria and have their glomerular filtration rate (GFR) estimated using one of a number of calculations based on serum creatinine and other clinical factors. 8,17 Creatinine-based equations are helpful to identify persons with kidney disease, but serum creatinine may be affected by factors other than glomerular filtration, notably muscle mass, liver disease, dietary intake, age, race/ethnicity, and gender. 18 While the calculated equations account for some of the effects of muscle mass, age, race/ethnicity, and gender, they overestimate glomerular function for persons with lower creatinine intake or production, as can occur in persons with liver disease and possibly advanced HIV infection. 18
Serum cystatin C, a small (13-kDa), nonglycosylated protein that is produced by all nucleated cells at a constant rate and is exclusively cleared by glomerular filtration, has been proposed as an alternative marker of renal function. 19 –21 Recent data illustrate that formulas utilizing serum cystatin C provide GFR estimates equivalent to serum creatinine-based measures that are not affected by muscle mass or decreased creatinine production. 22 The use of cystatin C is particularly relevant for older populations and for persons with chronic illnesses such as HIV infection. 23,24 Several studies have examined cystatin C as a marker of kidney function in HIV-infected persons 25 –27 and specifically proposed using serum cystatin C as an alternative marker for renal impairment in this population. In the present analysis, we evaluated renal function of participants in a contemporary cohort of HIV-infected patients treated only with cART or who were antiretroviral naive to describe the prevalence of and risk factors associated with renal dysfunction and to examine the association of elevated cystatin C levels with preclinical renal dysfunction in this population.
Materials and Methods
Participants
The SUN Study (ClinicalTrials.gov number, NCT00146419) is a prospective, observational cohort study funded by the Centers for Disease Control and Prevention (CDC) that monitors the clinical course of HIV-infected adults treated only with cART or who were antiretroviral naive. Patients were enrolled at seven HIV specialty clinics in four U.S. cities: St. Louis, Missouri; Providence, Rhode Island; Minneapolis, Minnesota; and Denver, Colorado. The study's main objectives were to monitor the incidence of and identify risk factors for metabolic and other medical complications related to the treatment of HIV infection and attendant prolonged survival; the detailed study protocol has been described elsewhere. 28 In brief, seven hundred HIV-infected adults were enrolled between March 2004 and June 2006 into a closed cohort. Eligible participants were ≥18 years of age with confirmed HIV infection, had a CD4 count >100 cells/mm3, and were either antiretroviral naive or had been treated solely with cART with no more than 30 days of cumulative exposure to any mono- or dual-antiretroviral regimen; cART was defined as the use of at least three drugs from two different antiretroviral drug classes, or the use of three or more nucleoside reverse transcription inhibitors (NRTIs). The current cross-sectional analysis includes 670 subjects with complete data available at baseline.
Clinical and metabolic data collection
Comprehensive clinical and demographic data were collected on all subjects at enrollment including past medical history, all active diagnoses, results of all laboratory testing, and type and duration of all prescribed medications. Many of the clinical and laboratory data elements necessary for the study were already collected as part of routine care. Additional study-specific laboratory testing included urinalysis and spot measurement of urine microalbumin and creatinine. Each subject completed an anonymous audio computer-assisted self-interview to obtain behavioral risk data and other health-related information including selected family history variables and use of tobacco, alcohol, and recreational drugs. Laboratory data were measured by commercial assay at each site according to the care provider's usual standard of care. Fasting status (at least 8 h) was verified at the time of specimen collection.
Laboratory tests used for research purposes only [i.e., fasting insulin, highly-sensitive C-reactive protein (hsCRP), 25-hydroxyvitamin D, cystatin C] were performed by the Diabetes Research and Training Center Radioimmunoassay Core Laboratory, Washington University School of Medicine. Serum and plasma used for these tests were iced and centrifuged at the time of blood draw then stored at −70°C until time of batched assay. Methods for these assays were as follows: cystatin C was analyzed by an immunoturbidometric assay using Dako reagents (Dakocytomation, Glostrup, Denmark) on a Hitachi 917 analyzer (Roche Diagnostics, Manheim, Germany); insulin was analyzed by radioimmunoassay using 125I-labeled tracer from Millipore (Millipore, Billerica, MA); hsCRP was analyzed by a latex particle-enhanced immunoturbidometric assay (Kamiya Biomedical Company, Seattle, WA) on a Hitachi 917 analyzer; and vitamin D was analyzed by a two-step radioimmunoassay (RIA) (Diasorin Inc, Stillwater, MN).
Renal function
Using the recommendations of the National Kidney Foundation,
17
we defined renal dysfunction as having an eGFR <90 ml/min/1.73 m2 and chronic kidney disease (CKD) as an eGFR <60 ml/min/1.73 m2 using the simplified Modification of Diet in Renal Disease (sMDRD) equation:
To explore the role of cystatin C as a marker of preclinical renal dysfunction, we dichotomized cystatin C concentrations and defined an elevated cystatin C concentration as a serum value of >1.0 mg/liter. This level was selected based on the upper limit of the normal reference range (0.55–1.41 mg/liter) for cystatin C 29 as well as previous data that have identified an increased risk of mortality, cardiovascular events, and of progression of kidney disease among persons with cystatin C levels above this level. 30 –32
Statistical analysis
The outcome variables included eGFR <90 ml/min/1.73 m2 and eGFR <60 ml/min/1.73 m2 calculated using the sMDRD formula and serum cystatin C level >1.0 mg/liter. Data were analyzed using the χ2 or Fisher's exact test for categorical variables and Student's t-test or the Mann–Whitney U test for normally and nonnormally distributed continuous variables, respectively. Univariate correlation testing was used to test the strength of association between renal dysfunction and other clinical variables. Variables were assessed for significant interaction and redundant variables were removed from the model. Multivariate logistic regression models were used to explore the associations with the outcome variables. Variables with a p-value <0.10 in bivariate analysis were entered stepwise into regression models in order to determine the most parsimonious multivariate model. Age, race/ethnicity, and gender were included in all models regardless of statistical significance. All p-values were two-tailed and considered significant if the p-value was <0.05. All statistical analyses were performed using SAS, version 9.1 (SAS Institute, Inc., Cary, NC).
Results
Subject characteristics and prevalence of renal dysfunction
At enrollment, among the 670 subjects for whom complete evaluable data for the present analysis were available, most were male (77%) and non-Hispanic white (59%, compared with 29% non-Hispanic black, 10% Hispanic, and 2% Other/unknown). The mean age was 41.0 years (Table 1) and the mean time since HIV diagnosis was 6.1 years. Nadir and baseline mean CD4 cell counts were 228 and 530 cells/mm3, respectively. The majority of subjects (79%) were prescribed cART, of whom 89% had a plasma HIV RNA <400 copies/ml.
Characteristics of SUN Study Participants
Includes acyclovir, pentamidine, foscarnet, cidofovir, or amphotericin B.
ACE, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker inhibitor; BMI, body mass index; CRP, C-reactive protein; HAART, highly active antiretroviral therapy; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PI, protease inhibitor.
Overall, the mean eGFR by the sMDRD equation was 96.8 ml/min/1.73 m2. Forty percent of subjects had renal dysfunction (eGFR <90 ml/min/1.73 m2), but only 3.3% had CKD (eGFR <60 ml/min/1.73 m2). Eighty-one subjects (13%) had proteinuria by urine dipstick and 69 subjects (11%) had microalbuminuria (urine albumin >30 mg/dl). In univariate analyses, persons with renal dysfunction were more likely to be older (43.5 vs. 39.3 years, p<0.001), to be of non-Hispanic white race/ethnicity (65% vs. 55%, p=0.040), to have higher BMI (27.0 vs. 26.1 kg/m2, p=0.066), to have hypertension (39% vs. 26%, p<0.001), to use an angiotensin-converting enzyme (ACE) inhibitor or angiotensin receptor blocker (ARB) (21% vs. 15%, p=0.024), to have microalbuminuria (15% vs. 8%, p=0.005), to have higher mean hemoglobin (14.6 vs. 14.4 g/dl, p=0.041), to have higher mean cystatin C levels (0.94 vs. 0.87 mg/liter, p<0.001), and to have higher mean 25-hydroxyvitamin D levels (27.0 vs. 23.0, p<0.001). In univariate analyses, persons with renal dysfunction were less likely to be current smokers (39% vs. 47%, p=0.035) or intravenous drug users (1% vs. 3%, p=0.031). The following HIV-related parameters were also associated with renal dysfunction in univariate analysis: currently taking tenofovir (46% vs. 36%, p=0.013) or ritonavir (any dose) (39% vs. 24%, p<0.01) or both (23% vs. 14%, p<0.001) and having controlled HIV viremia (HIV RNA <400 copies/ml) (77% vs. 70%, p=0.027). In multivariate analysis, the following parameters remained independently associated with renal dysfunction: older age, non-Hispanic white race/ethnicity, higher BMI, having hypertension, higher cystatin C levels, and current prescription of ritonavir (Table 2).
Factors Associated with Renal Dysfunction and Increased Cystatin C Levels
Age, race/ethnicity, and gender were included in all models regardless of statistical significance.
CI, confidence interval; sMDRD, simplified Modification of Diet in Renal Disease; GFR, glomerular filtration rate; cART, combination antiretroviral therapy.
Factors associated with CKD (eGFR <60 ml/min/1.73 m2) in univariate analysis included older age (48.0 vs. 40.7 years, p<0.001), female gender (45% vs. 23%, p=0.012), non-Hispanic black race/ethnicity (59% vs. 28%, p=0.016), higher BMI (29.2 vs. 26.4 kg/m2, p=0.029), hypertension (77% vs. 29%, p<0.001), receipt of an ARB/ACE inhibitor (45% vs. 17%, p=0.002), chronic HCV infection (32% vs. 13%, p=0.010), microalbuminuria (24% vs. 10%, p=0.043), elevated mean cystatin C (1.20 vs. 0.89 mg/liter, p<0.001), lower nadir CD4 cell count (123 vs. 230 cells/mm3, p=0.002), history of an opportunistic infection (50% vs. 22%, p=0.002), and currently taking cART (100% vs. 78%, p=0.007), specifically ritonavir (50% vs. 29%, p=0.039). Because of the small number of patients (n=22) with CKD, a multivariate analysis was not conducted.
Cystatin C results
Eighteen subjects did not have an evaluable stored sample for cystatin C measurement. Among the remaining 652 subjects who had complete baseline data and cystatin C results, the mean cystatin C level was 0.90±0.01 mg/liter. There was a significant correlation between cystatin C and eGFR as calculated using the sMDRD equation and between cystatin C and urine albumin levels (r=–0.35 and 0.14, respectively, p<0.001 for both; see Figs. 1 and 2). One hundred and twenty subjects (18%) had a cystatin C level >1.0 mg/liter. In univariate analysis, persons with an elevated cystatin C level were older (42.9 vs. 40.6 years, p=0.008), more likely to be hypertensive (41% vs. 28%, p=0.007), to be prescribed an ARB/ACE inhibitor (25% vs. 16%, p=0.016), to currently smoke tobacco (61% vs. 40%, p<0.001), to have viral hepatitis C (HCV) (29% vs. 10%, p<0.001) or chronic viral hepatitis B coinfection (9% vs. 4%, p=0.023), to have lower mean hemoglobin (14.0 vs. 14.6 g/dl, p=0.001), lower mean total cholesterol (177 vs. 187 mg/dl, p=0.027), lower LDL cholesterol (100 vs. 111 mg/dl, p=0.005), and to have microalbuminuria (20% vs. 8%, p<0.001). These patients also had lower baseline CD4 cell counts (453 vs. 547 cells/mm3, p<0.001), were less likely to have an undetectable HIV viremia (≤400 copies/ml) (60% vs. 76%, p<0.001), were less likely to be prescribed cART (72% vs. 81%, p=0.029), and were prescribed cART for a shorter mean duration (2.3 vs. 3.1 years, p<0.001).
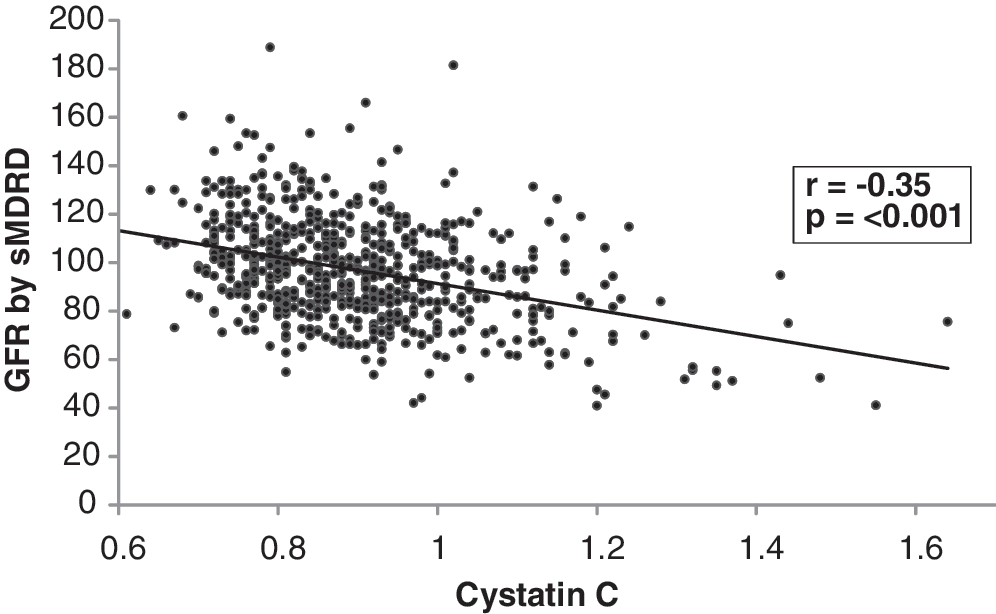
Correlation between cystatin C and estimated glomerular filtration rate (eGFR) calculated by simplified Modification of Diet in Renal Disease (sMDRD). Spearman's rank correlation was performed.
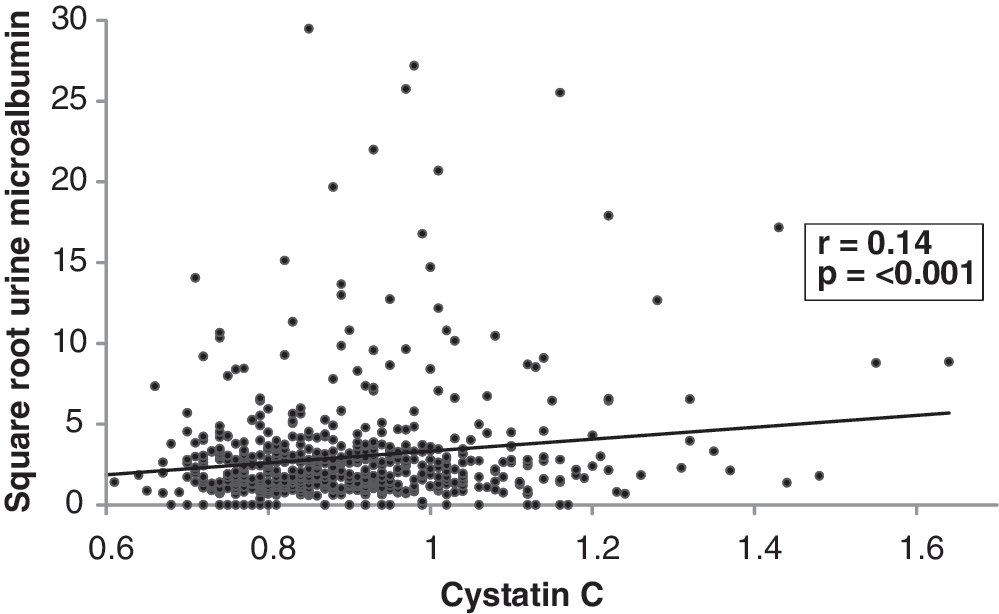
Correlation between cystatin C and urine albumin level. Spearman's rank correlation was performed. Microalbumin data were square root transformed to account for nonnormal distribution.
For subjects prescribed cART, elevated cystatin C was associated with current exposure to tenofovir (49% vs. 38%, p=0.026). In multivariate analysis, elevated cystatin C remained associated with older age, HCV coinfection, current tobacco smoking, current use of tenofovir, and microalbuminuria. Longer duration of cART and undetectable viral load were associated with lower levels of cystatin C (Table 2).
Discussion
Overall, these data confirm that end stage renal disease and chronic kidney disease are less common in the cART era among HIV-infected persons who are engaged in care. 5 –7 Nevertheless, impairment in renal function is of growing importance as comorbidities such as diabetes, hypertension, and atherosclerosis are becoming more prominent in the long-term management of HIV disease. 33,34 While the prevalence of renal dysfunction (eGFR <90 ml/min/1.73 m2) was high (40.3%) in this cohort, CKD (eGFR <60 ml/min/1.73 m2) was uncommon (3.3%), similar to other reported cohorts with access to cART. 7 Factors associated with renal dysfunction included traditional risk factors (e.g., older age, hypertension, elevated BMI), as well as current exposure to ritonavir and non-Hispanic white race/ethnicity. This latter association might have resulted from the effect of the race-based correction factor used in the sMDRD formula. Notably, when we focused our analysis on subjects with CKD (eGFR <60 ml/min/1.73 m2), non-Hispanic black race/ethnicity was associated with more advanced renal dysfunction, as expected.
Concern has been raised about the inherent bias of using creatinine-based formulas to estimate GFR for populations enriched in patients with chronic medical conditions such as HIV infection. 35,36 Notably, GFR estimation formulas have not been formally validated for HIV-infected adults. Several studies have assessed the utility of cystatin C as an alternative measure of glomerular filtration and found it to perform as well as, if not better, than creatinine-based formulas. 22,37 –39 In the Modification of Diet in Renal Disease (MDRD) Study, both cystatin C levels and serum creatinine were highly correlated with glomerular filtration estimates by iothalamate renal clearance, but only cystatin C was significantly associated with mortality endpoints. 38 The authors concluded that serum cystatin C levels better reflected renal function independent of confounding factors such as systemic inflammation or weight. 38 Given the recent use of the CKD-EPI formula, we also evaluated the correlation between eGFR calculated by the sMDRD and CKD-EPI formulas and found a strong correlation (Spearman correlation r=0.94, p<0.001) suggesting that the two formulas produce similar results in this cohort. Nevertheless, there is growing support for the use of CKD-EPI, particularly in persons with eGFR >60 ml/min/1.73 m2. 40,41
Our multivariate analyses demonstrated that factors traditionally associated with renal disease were also associated with elevated cystatin C (>1.0 mg/liter), such as hypertension, tobacco smoking, older age, and viral hepatitis C coinfection. Among HIV-specific risks, current use of tenofovir was also associated with elevated levels of serum cystatin C while longer duration of cART and controlled HIV viremia (plasma HIV RNA <400 copies/ml) were associated with decreased levels of serum cystatin C. The relationship with both chronic HCV infection and uncontrolled HIV viremia raises the concern as to whether elevated cystatin C is a marker of renal function or ongoing inflammation as a consequence of chronic viremia. Additional research is needed to explore these findings. Furthermore, the correlation between cystatin C and eGFR was significant but modest, suggesting that there are other factors that may better explain renal dysfunction. The fact that tenofovir use was associated with elevated cystatin C but not reduced creatinine clearance is also worthy of further study given that cystatin C may serve as a marker of preclinical renal disease. 42 This is particularly warranted given the expanding use of tenofovir for the treatment of hepatitis B infection and as a component of preexposure prophylaxis for HIV infection. 43,44
The relationship between uncontrolled HIV viremia and renal dysfunction has been noted in other research, most notably a recently published study. 45 In that study, subjects who followed a treatment interruption strategy were at higher risk of developing fatal or nonfatal renal disease when compared with patients randomized to continue antiretroviral therapy without interruption. In subsequent analyses from the same trial, it was reported that treatment interruption was also associated with elevated levels of cystatin C. 27,46 The authors suggested that this increase was likely related to direct viral toxicity on the renal tubule rather than the overall inflammatory milieu associated with poorly controlled HIV infection, although the local injury is potentially mediated by inflammation as suggested in several other published reports both in HIV-infected and HIV-negative subjects. 27,47 –49 Further evaluations of the role of cystatin C and its correlation with and regulation by inflammatory cytokines will improve the utility of this protein as a marker of renal function. 50,51 Clearly, there remains the need to further evaluate the utility of cystatin C as a marker of renal function. For the current cohort, we determined the threshold of cystatin C >1.0 mg/liter had a positive predictive value of only 0.57 and 0.12 for eGFR <90 and <60 ml/min/1.73 m2, respectively, and a negative predictive value of 0.64 and 0.99 for eGFR <90 and <60 ml/min/1.73 m2, respectively (data not shown). These data suggest that the use of cystatin C alone lacks adequate sensitivity for an effective screening test.
Urine dipsticks and spot urine microalbumin quantification, which are used extensively in the management of diabetes, can also provide the HIV practitioner with a means to monitor renal function and screen for incipient preclinical dysfunction potentially related to chronic HIV infection, its treatment, or concomitant comorbidities such as hypertension or diabetes. Overall, 13% of the SUN cohort had at least trace proteinuria by urinary dipstick and 11% had microalbuminuria, which was microalbuminuria was associated with elevated cystatin C levels. Considering the relatively inexpensive cost of spot urine microalbumin quantification, its integration into the routine care of HIV warrants further evaluation. Given that elevated cystatin C was also associated with renal dysfunction, further research is needed to identify cystatin C criteria that equate to various degrees of renal function by a gold standard such as iothalamate clearance.
Our analysis has a number of important limitations. It was cross-sectional and therefore limited in its ability to discern generalizable associations as well as to evaluate changes in renal function over time. Longitudinal follow-up will provide greater insight into the findings reported here. We cannot generalize our findings from this cohort to all HIV-infected patients; however, we believe our data are relevant to the care of contemporary and future patients in developed nations for many of whom HIV will be a chronic medical condition. Also, our treatment data are limited to prescribed medications and we do not have complete data on over-the-counter therapies, most notably nonsteroidal antiinflammatory medications, the use of which can contribute to renal dysfunction. The utility of cystatin C among HIV-infected subjects, specifically with regards to the relationship with inflammation and chronic viral infections and the mechanism by which it is increased in both renal disease and inflammatory states, requires further clarification beyond the scope of the present analysis.
In conclusion, the prevalence of CKD was low in this cohort of contemporary HIV-infected patients; however, a significant proportion of persons had preclinical renal dysfunction that might have negative long-term implications for future renal function and other parameters. We found that elevated cystatin C, a marker for preclinical renal dysfunction, was common and strongly associated with ongoing HIV viremia, a finding that suggests that the benefits of cART-associated virologic suppression go beyond immune reconstitution. Independent associations with modifiable risk factors, including hypertension, smoking, and hepatitis C coinfection, indicate that there are additional opportunities for prevention of renal disease. Further studies are warranted to explore the utility of cystatin C and the impact of cART on the prevention of end-organ disease.
Footnotes
Acknowledgments
Supported by the Centers for Disease Control and Prevention contract numbers 200-2002-00610, 200-2002-00611, 200-2002-00612, 200-2002-00613, 200-2007-23633, 200-2007-23634, 200-2007-23635, and 200-2007-23636. The investigation followed the guidelines of the U.S. Department of Health and Human Services regarding protection of human subjects. The study protocol was approved and renewed annually by each participating institutions' ethical review board. All study participants provided written, informed consent.
Prior Presentation: Prevalence and Predictors of Renal Insufficiency Among HIV-Infected Patients in the Study to Understand the Natural History of HIV/AIDS in the Era of Effective Therapy. XVII International AIDS Conference, August 3–8, 2008, Mexico City, Mexico. Abstract #THPE0231.
Author Disclosure Statement
E.T.O. has served as a consultant, on speakers' bureau, or on an advisory board for the following companies: Gilead, Bristol Myers Squibb, Glaxo-Smith-Kline, Tibotec, Merck, Monogram Sciences, and Boehringer Ingelheim. He also has received research support from the following companies: Abbott, Gilead, Bavarian Nordic, Glaxo-Smith-Kline, Boehringer Ingelheim, and Tibotec. F.R. has served as a consultant, on speakers' bureau, or on an advisory board for the following companies: Gilead, Glaxo-Smith-Kline/ViiV, Tibotec, Merck, and Boehringer Ingelheim. He also has received research support from the following companies: Gilead and Tibotec. K.H. has served as a consultant, on speakers' bureau, or on an advisory board for the following companies: Gilead and Glaxo-Smith-Kline/ViiV. He has received research support from Tibotec, Glaxo-Smith-Kline, Serono, Centers for Disease Control, and NIH (NIAID).
The findings and conclusions from this review are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.