
Abstract
Given that atazanavir (ATV) increases bilirubin in an exposure-dependent manner, we tested whether bilirubin levels could be used as a surrogate of virological response to ATV-based regimens in 182 patients. Bilirubin increases of ≥0.7 mg/dl were independently associated with early virological response with an odds ratio of 5.2 (95% confidence interval 2.2–11.9). Total bilirubin, a nonexpensive, simple, and widely available parameter, might be used as a surrogate of virological response to ATV-based regimens, especially in areas with limited resources where HIV-RNA testing is not available.
A
The assessment of the virological efficacy of antiretroviral therapy is made using laboratory markers such as plasma HIV-RNA, CD4+ T cell counts, drug resistance testing, and plasma drug plasma levels, all of which are quite expensive and often unavailable in areas with limited resources. Thus, alternative surrogate markers of virological response to antiretroviral therapy are much appreciated. Given that ATV-associated hyperbilirubinemia is exposure dependent and that ATV plasma trough concentrations are a good predictor of virological response to the drug, 5 we tested whether bilirubin levels, the determination of which is cheap and easy to perform, could be used as a surrogate of virological response to ATV-based regimens.
All HIV-infected patients who had initiated ATV-based antiretroviral therapy at our institution between January 2006 and December 2009 and had detectable viral load were retrospectively identified. Patients receiving at baseline drugs known to alter bilirubin levels such as indinavir, raltegravir, and/or ribavirin were excluded from the study. The main demographics and other clinical characteristics were recorded in a case report form specially designed for this study.
Plasma HIV-RNA was measured using Versant bDNA (Bayer, Barcelona, Spain) at baseline and at week 12 of therapy. Early virological response was defined as plasma HIV-RNA <50 copies/ml at week 12 of therapy. Total bilirubin was determined at baseline and subsequently every 12 weeks up to 72 weeks of therapy. Grade 3/4 hyperbilirubinemia was defined in accordance with the Division of AIDS Adverse Events guidelines, as serum total bilirubin ≥2.6 times the upper limit of normal. 6 Chronic hepatitis C virus (HCV) infection was defined as detectable serum HCV-RNA (>10 IU/ml). Chronic hepatitis B virus (HBV) infection was defined as positive HBV surface antigen. The UGT1A1*28 allele was examined by sequencing of the DNA extracted from peripheral blood mononuclear cells.
All statistical analyses were performed using the SPSS package version 13.0 (SPSS Inc, Chicago, IL). Categorical variables were expressed in absolute values and percentages and continuous variables were expressed as median and interquartile range (IQR) values. Proportions were compared using the Fisher's exact test. Lineal regression analyses were performed to assess factors independently influencing the increase in total bilirubin at week 12. Receiving operating characteristic (ROC) curves were performed to calculate the sensitivity and specificity values for distinct increases in total bilirubin for which early virological response was more likely to occur. Logistic regression analyses were performed to assess the impact of the increases in total bilirubin predicting early virological response.
A total of 182 patients who had initiated an ATV-based regimen during the study period were examined. All were white and 78% were male. The median age was 42 years (IQR, 38–45); plasma HIV-RNA 3.8 log copies/ml (IQR, 2.5–4.6); CD4 counts 336 cells/μl (IQR, 220–523), total bilirubin 0.6 mg/dl (IQR, 0.5–0.8), HCV coinfection in 35% of patients, and chronic hepatitis B in 4%. A total of 117 patients (64%) initiated boosted ATV (ATV/r 300/100 mg once daily) while 65 (36%) initiated unboosted ATV (ATV 400 mg once daily). Overall, tenofovir was used as part of the regimen in 113 patients (62%). A total of 84 patients (46%) carried at least one UGT1A1*28 allele, with 35% of patients being heterozygotes and 11% homozygotes.
The median total bilirubin level at week 12 was 2.0 mg/dl (IQR, 1.5–3.0). Overall bilirubin levels did not change over the 2 years of follow-up (p>0.05). The median increase in total bilirubin at week 12 (ΔBIL) was 1.3 mg/dl (IQR, 0.8–2.3). A total of 39 patients (21%) developed grade 3/4 hyperbilirubinemia.
Linear regressions were performed to evaluate which factors were associated with ΔBIL at week 12, including age, gender, baseline CD4 cells count, HCV coinfection, HBV coinfection, ATV dose, and UGT1A1*28 allele. The use of ATV/r and the presence of UGT1A1*28 allele were independently associated (β 95% CI) with higher increases in bilirubin [0.65 (0.22–1.1) p=0.003 and 0.98 (0.56–1.4) p<0.001, respectively].
Overall, 143 patients (79%) achieved virological response at week 12 of therapy. The median ΔBIL at week 12 was significantly higher in patients who achieved virological response compared to those who did not [1.5 (0.9–2.4) vs. 0.9 (0.1–1.7) mg/dl, p<0.001] (Fig. 1).
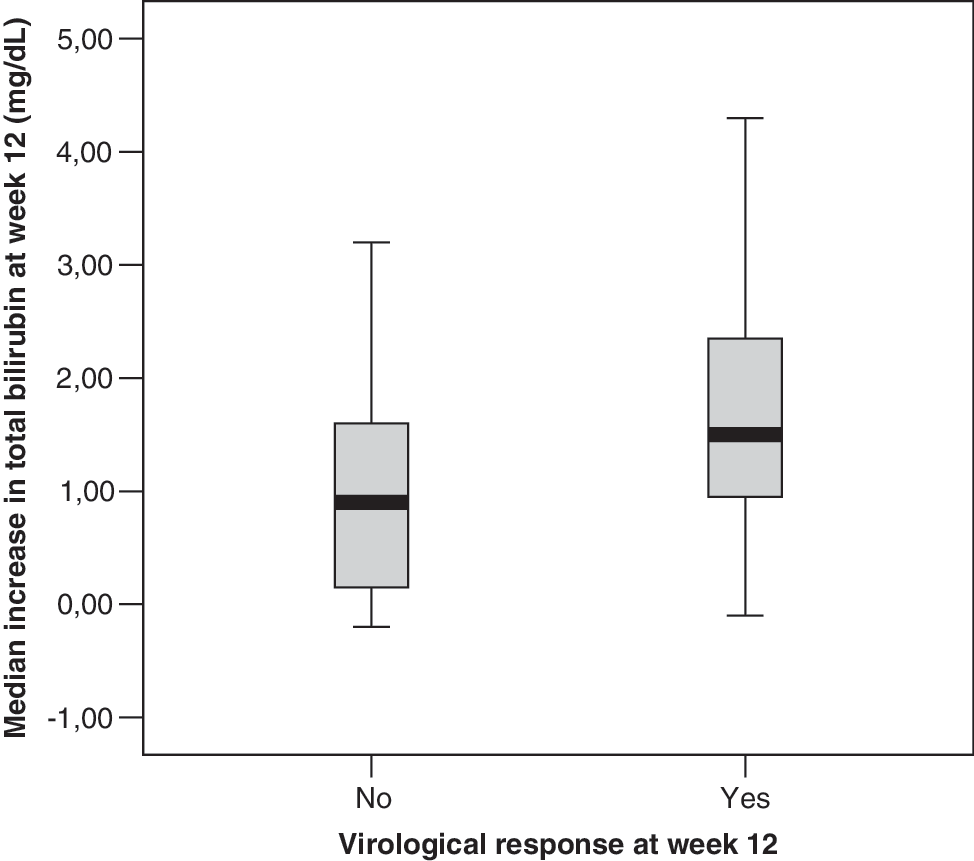
Increase in total bilirubin at week 12 of treatment in patients with and without early virological response.
Patients on ATV400 were selected to explore the minimum ΔBIL that might predict virological response. The best ΔBIL threshold associated with virological response was 0.7 mg/dl (87% sensitivity and 46% specificity, p<0.001). Logistic regression analyses were performed to analyze the predictive value of the defined threshold of ΔBIL. The variables included in the analyses were age, sex, baseline HIV viral load, baseline CD4 cells count, and ΔBIL threshold ≥0.7 at week 12 of therapy. In the multivariate analysis, baseline CD4 cells count and ΔBIL threshold ≥0.7 at week 12 independently predicted (OR 95% CI) early virological response [50.1 (50.0–50.2) per 50 cells/mm3 increase p=0.013 and 5.2 (2.2–11.9) p<0.001, respectively]. The positive and negative predictive values of ΔBIL threshold ≥0.7 were 86% and 50%, respectively.
These results suggest that the increase in total bilirubin after beginning ATV remains fairly stable for at least 2 years of follow-up. Moreover, ritonavir boosting and the presence of the UGT1A1*28 allele are independently associated with greater bilirubin increases on ATV therapy. Finally, increases in total bilirubin levels are independent predictors of virological response at week 12 of therapy. Thus, total bilirubin might be used as a surrogate marker of virological response to ATV-based therapy, especially in areas with limited resources where HIV RNA testing is not available. This parameter may help the clinician to promote early interventions that may improve the virological response (e.g., drug adherence enhancement, ritonavir boosting implementation).
Adverse drug events have previously been used as surrogates of drug exposure and virological efficacy to other drugs. This is the case for ribavirin-associated haemoglobin decrease as a surrogate of virological response to HCV therapy. 7,8 In a previous study, the association between increase in total bilirubin and virological response to ATV-based therapy was postulated, with bilirubin increases >0.4 mg/dl as predictors of a >2 log drop or of an undetectable viral load at week 8 of therapy. However, the study did not report ATV dosing nor the distribution of the UGT1A1*28 allele in the study population. Moreover, some patients in the study had undetectable viremia at baseline and others were on indinavir, which could affect baseline bilirubin levels. 9 In contrast, our study excluded patients on drugs that could potentially affect bilirubin levels (e.g., indinavir, raltegravir, ribavirin) as well as patients with undetectable viral load at baseline.
We found that increases in bilirubin ≥0.7 mg/dl independently predicted early virological response to ATV with an odds ratio of 5.2, with positive and negative predictive values of 86% and 50%, respectively. The limited negative predictive value could be due to the relatively high rate (79%) of early virological response in our study population, as it is well known that predictive values largely depend on rates of study variables. In addition, we did not distinguish between antiretroviral-naive and experienced patients or between patients with and without previous treatment failures. The impact of low bilirubin levels on the virological response could be less important in naive than in antiretroviral-experienced patients, which could result in a lower negative predictive value. In this regard, the results of this study should be interpreted carefully because experienced patients or patients harboring viruses with reduced drug susceptibility may require higher concentrations of atazanavir, and therefore greater increases in bilirubin, than naive patients to achieve a virological response.
In summary, changes in total bilirubin levels at week 12 of ATV-based therapy might be used as a surrogate of virological response in HIV-infected patients. This simple, cheap, and widely available laboratory parameter might be of particular interest in resource-limited settings.
Footnotes
Acknowledgments
This work was supported in part by grants from Fondo de Investigación Sanitaria (FIS CP07-00016), Fundación Investigación y Educación en SIDA (FIES), Red de Investigación en SIDA (RIS, ISCIII-RD06/0006/0040), and the European Union 6th Framework Programme (NEAT, LSHP-CT-2006- 037570).
J.M. and S.R.N. designed the study. L.C., J.M., and L.C. performed the genotypic analysis. J.M., L.C., E.A., and E.V. assisted in the collection of clinical information. J.M. and S.R-N. helped with the statistical analyses. J.M., S.R-N., and V.S. wrote the manuscript. All authors discussed, revised, and approved the current version.
Author Disclosure Statement
No competing financial interests exist.