
Abstract
Trends in transmitted drug resistance-associated mutations (TDRM) in HIV-1infection vary depending on geographic and cohort characteristics. The impact of TDRM among patients receiving fully active combination antiretroviral therapy (cART) is poorly characterized. This was a retrospective study of 801 HIV-1-infected treatment-naive patients from 2001 to 2009 who had pre-cART genotype resistance test results available. The prevalence of TDRM was compared for each year strata. Multivariate Cox proportional hazards regression models were used to assess factors associated with virologic failure at 48 weeks. TDRM was detected in 136 (17%) patients with ≥2 class TDRM in 20 patients. K103N/S was the most frequent (n=77). There were no changes in the prevalence of mutations over time (P trend=0.67). Six hundred and eleven patients were started on cART. Virologic failure occurred in 38% of those with TDRM and 24% of those without (p<0.01). In multivariate analysis, nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance was associated with a 1.5-fold increased risk of virologic failure. TDRM remains common among treatment-naive HIV-1-infected patients, affecting one in six patients. Transmission of NNRTI drug resistance was associated with risk of virologic failure despite initiation of genotype-guided cART.
Introduction
The use of potent combination antiretroviral therapy (cART) provides sustained virologic suppression for an individual living with HIV and substantially reducing the morbidity and mortality associated with HIV-1 infection. 1 Despite this advance in treatment, virologic failure can develop in 10–20% as a result of suboptimal medication adherence, the presence of preexisting drug resistance, or the emergence of drug resistance. 2,3 Transmitted drug resistance-associated mutations (TDRM) are of particular concern as they limit the choice of first-line cART, decrease efficacy of subsequent antiretroviral regimens and increase the risk of treatment failure. 4 –6 TDRM have been documented among treatment-naive HIV-1-infected patients with a prevalence ranging from 3% to 24%, depending on the cohort and geographic characteristics; the highest prevalence is noted in countries with long-established use of antiretrovirals. 7 –11 Studies on time trends in the prevalence of TDRM are inconsistent. In Belgium, the overall prevalence of TDRM was reported at 8.4% with no time trend. 12 Bracciale et al. demonstrated that the transmission of nucleoside reverse transcriptase inhibitor (NRTI) and protease inhibitor (PI) resistance declined over time, but nonnucleoside reverse transcriptase inhibitor (NNRTI) resistance increased from 3.7% during 1996–2001 to 7.8% during 2002–2004 and remained stable thereafter (5.8% in 2006–2007). 13
Previous data highlight that the presence of TDRM influences the outcome of initial cART and pre-cART genotype resistance testing improves clinical outcomes and is cost effective. 14,15 Therefore, routine genotype resistance testing is considered the standard of care for all newly diagnosed HIV-1-infected patients to guide the choice of initial treatment. 16 Yet there are few studies evaluating the impact of TDRM on virologic efficacy when patients initiate cART with at least three active agents chosen based on genotype resistance testing. We evaluated the prevalence and time trend of TDRM in a midwestern HIV outpatient clinic and the virologic outcomes of treatment-naive patients who were started on cART with at least three fully active agents guided by the result of genotype resistance testing.
Materials and Methods
All adult (age ≥18 years), treatment-naive HIV-1-infected patients who were new to Washington University HIV Outpatient Clinic from January 1, 2001 to June 30, 2009 were screened for the study. Patients with HIV-1 genotype resistance testing performed prior to starting on cART were included in the study. This study was approved by the Washington University School of Medicine Human Research Protection Office.
The following data were abstracted from electronic medical record: baseline demographics (age, sex, race, and HIV risk factors), psychiatric comorbidity, substance use (history of marijuana, cocaine, heroin, or methamphetamine use), tobacco use, sexually transmitted diseases (STDs: history of syphilis, gonorrhea, Chlamydia trachomatis infection, or genital herpes simplex virus infection), hepatitis C virus (HCV) coinfection (positive anti-HCV antibody), longitudinal CD4 cell counts, longitudinal HIV RNA levels, pre-cART HIV-1 genotype, antiretroviral regimen, pre-cART opportunistic infections, and the first date of virologic suppression on the cART initiated. The definition of cART was receipt of at least three active antiretroviral medications as part of a regimen.
The prevalence and trends of TDRM during the study period were calculated. Genotypic assays were obtained from either Quest Diagnostics or the Washington University Retrovirus Laboratory (ViroSeq HIV-1 Genotyping System, Celera Corporation, Alameda, CA). The genotype results were interpreted with the standardized list of mutations for surveillance of transmitted drug resistance (DRM) established by the World Health organization (WHO list). 17 TDRM were noted individually and also grouped by antiretroviral class: NRTI, NNRTI, and PI resistance mutations. To assess the impact of TDRM, two groups (those with TDRM and those without) were compared in regards to virologic outcomes after initiating cART. Virologic suppression was defined as HIV RNA level <400 copies/ml at 48 weeks. This cutoff was used because some data predated the use of ultrasensitive HIV RNA assays.
Statistical analysis
Differences between the groups were compared using chi-square and Fisher exact test for categorical data and Mann–Whitney tests for continuous variables. HIV RNA levels were log10 transformed. Calculations of TDRM prevalence in each antiretroviral class were conducted by using the number of new cases of resistance detected in each year divided by the number of new antiretroviral-naive patients in each year. Time trends of prevalence in TDRM for each antiretroviral class were analyzed by logistic regression. To assess the virologic outcomes, univariate analyses with a Cox proportional hazards regression models with one predictor was conducted. Patients were censored as virologic failure when they did not achieve virologic suppression at 48 weeks. Variables associated with virologic failure at p<0.10 in the univariate analyses were considered in the multivariate Cox proportional hazards regression models. All statistical calculations were performed using R 2.12.0 (R Foundation for Statistical Computing, Vienna, Austria), and statistical significance was defined as p<0.05.
Results
Among the 801 patients who had pre-cART genotype resistance testing, 68% were male, 72% were black, and 35% had a CD4 cell count <200 cells/mm3 (Table 1). Based on the WHO list, TDRM was detected in 136 (17%) patients; NRTI resistance was identified in 6% (n=48), NNRTI resistance in 12% (n=94), and PI resistance mutation in 2% (n=18). Mutations at T215 (n=23, 2.9%) and M41 (n=13, 1.6%) were the two most commonly found NRTI resistance and K103N/S (n=77, 9.6%) was the most commonly found NNRTI resistance, comprising almost half of the entire prevalence of TDRM. L90M (n=8, 1%), V82A/L (n=8, 1%), and M46I/L (n=7, 0.9%) were the three commonly found PI resistance mutations (Table 2). Among the 136 patients with TDRM, 20 (15%) patients had ≥2 class TDRM. There were no significant time trends in the prevalence of any specific TDRM (P trend=0.67), NRTI (P trend=0.75), NNRTI (P trend=0.99), and PI resistance (P trend=0.76) (Fig. 1).
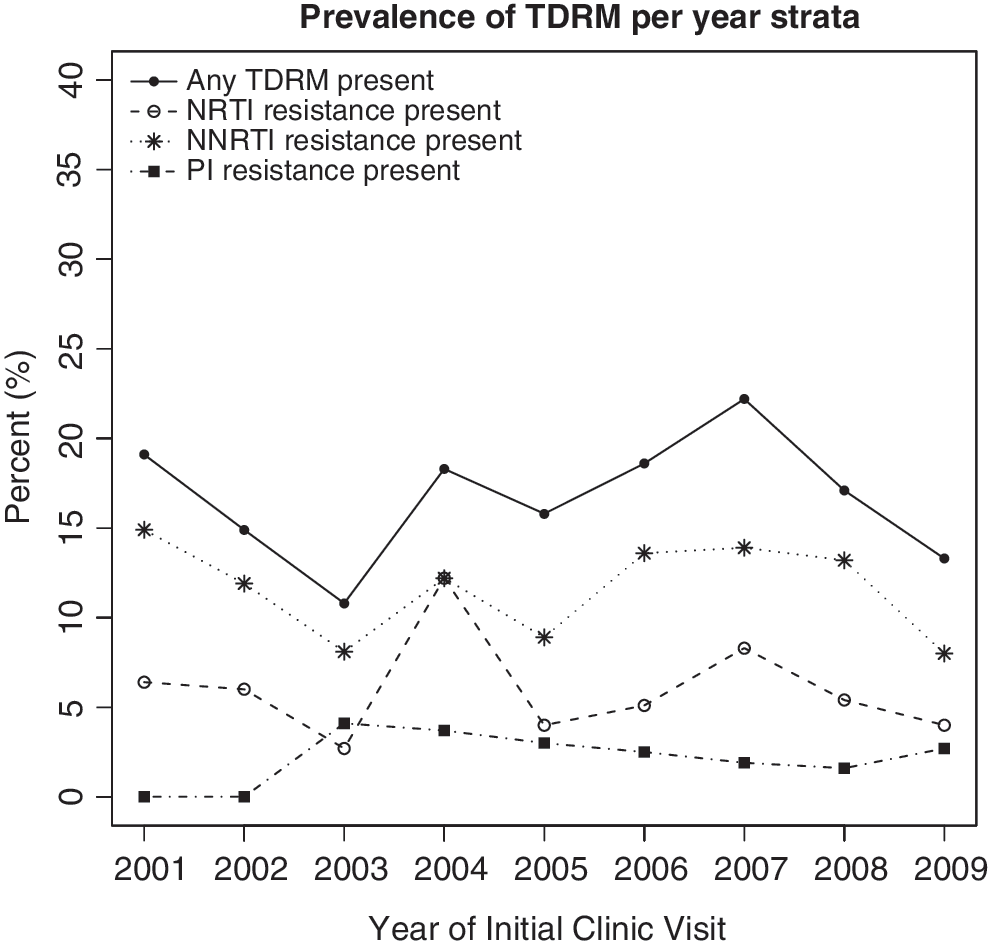
Prevalence and trends of TDRM per year strata. TDRM, transmitted drug-resistant mutation; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
Baseline Characteristics of the Study Population
Substance abuse, history of marijuana, cocaine, heroin, or methamphetamine use.
Baseline CD4 cell count and HIV RNA level.
TDRM, transmitted drug-resistant mutation; IQR, interquartile range; MSM, men who have sex with men; IDU, injection drug use; STDs, sexually transmitted diseases within 1 year of initiating cART; HCV, chronic hepatitis C virus infection; cART, combination antiretroviral therapy; CD4 cell count, CD4 cell count (cells/mm3); log10 HIV RNA, log10 HIV RNA plasma level (copies/ml).
Frequency of Individual Resistance Mutations
Drug resistance mutation based on the WHO list as described in the Materials and Methods section.
NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
Patients with TDRM and those without were compared. Those with TDRM were younger and less likely male (both p<0.05), but other characteristics, race, and HIV risk factors were similar. There were no differences in proportion of patients with psychiatric comorbidities, substance use, tobacco use, or those with a history of STDs. Baseline CD4 cell counts and HIV RNA levels did not differ between the groups (Table 1).
Among the 801 treatment-naive patients with genotype resistance testing, 611 patients (76%) were started on cART. Pre-cART CD4 cell count and HIV RNA level did not differ between the two groups. Patients with TDRM were started more frequently on PI-based cART regimen (p<0.001). Virologic failure was observed in 42 (38%) of patients in the TDRM group and 121 (24%) in those without (p<0.01). Changes in CD4 cell count at 24 weeks (median increase of 136 and 121 cell/mm3, p=0.85) and 48 weeks (median increase of 159 and 156 cell/mm3, p=0.78) did not differ between the two groups (Table 3).
Bivariate Analyses of Patients Started on cART
cART, combination antiretroviral therapy; TDRM, transmitted drug-resistant mutation; IQR, interquartile range; pre-cART, prior to initiation of cART; CD4 cell count, CD4 cell count (cells/mm3); log10 HIV RNA, log10 HIV RNA plasma level (copies/ml); NNRTI, nonnucleoside reverse transcriptase inhibitor; NRTI, nucleoside reverse transcriptase inhibitor; PI, protease inhibitor.
By univariate analyses, those with pre-cART opportunistic infections (HR 0.68; 95% CI 0.56–0.84), the presence of any TDRM (HR 0.70; 95% CI 0.54–0.91), the presence of NNRTI resistance (HR 0.65; 95% CI 0.47–0.90), and plasma HIV RNA level of greater than 100,000 copies/ml (HR 0.64; 95% CI 0.52–0.78) were less likely to achieve virologic suppression at 48 weeks. Conversely, persons receiving a NNRTI -based regimen rather than a PI-based regimen (HR 1.24; 95% CI 1.02–1.51) and use of an efavirenz-based regimen rather than a boosted atazanavir-based regimen (HR 1.31; 95% CI 1.02–1.68) were more likely to achieve virologic suppression at 48 weeks.
The impact of NNRTI resistance on virologic outcomes was analyzed by multivariate analyses, adjusting by the presence of pre-cART opportunistic infections, a plasma HIV RNA level of greater than 100,000 copies/ml, and use of an NNRTI-based regimen rather than PI-based regimen. NNRTI resistance had HR of 0.67 (95% CI 0.47–0.94), conferring a 1.5-fold increased risk of virologic failure (Table 4).
Hazard Ratios for Achieving Virologic Suppression at 48 Weeks by Univariate and Multivariate Analyses
Virologic suppression was defined as HIV RNA level <400 copies/ml at 48 weeks.
HR, hazard ratio; CI, confidence interval; TDRM, transmitted drug-resistant mutation; cART, combination antiretroviral therapy; pre-cART, prior to initiation of cART; NRTI, nucleoside reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse transcriptase inhibitor; PI, protease inhibitor; EFV, efavirenz; ATV/r, atazanavir boosted with ritonavir.
Discussion
In this cohort, the prevalence of TDRM was 17%, affecting one in six newly diagnosed, treatment-naive HIV-infected patients. Those with NNRTI resistance had a 1.5-fold increased risk of virologic failure at 48 weeks. These data highlight that TDRM, especially NNRTI resistance mutations, have a meaningful negative impact on virologic outcomes when HIV-infected treatment-naive patients initiate even genotype guided cART.
Our findings can be explained by three possibilities. The first is that NNRTI resistance mutations themselves confer a higher risk for virologic failure. Second, NNRTI-based regimens may simply be superior to PI-based regimens. In univariate analyses, patients initiating an NNRTI-based regimen were more likely to achieve virologic suppression at 48 weeks when compared to those initiating a PI-based regimen. A randomized clinical trial from the AIDS Clinical Trial Group (ACTG) A5142 study similarly demonstrated the superiority of an efavirenz-based regimen when compared to the PI-based regimen using lopinavir/ritonavir. 18 Conversely, other randomized controlled studies such as the ACTG A5202 study or the Altair study have demonstrated equivalent efficacy with efavirenz- versus boosted atazanavir-based regimens. 19,20 However, these studies excluded patients with known baseline NNRTI resistance and thus cannot specifically address the issue. A subanalysis of A5202 comparing the efficacy of efavirenz and boosted atazanavir between different males and females showed the inferiority of boosted atazanavir in in black race and females. 21 The third possibility is that the presence of NNRTI resistance may serve as a proxy for undetected drug resistance mutations. Ultradeep sequencing may provide more information about the presence of drug resistance mutations, but this technique is available only in research settings and is not clinically validated. 22
The TDRM prevalence of 17% is comparable to the data from the Centers for Disease Control and Prevention (16% prevalence), 23 and confirms the importance of monitoring for TDRM. We were unable to confirm the decline in the prevalence of TDRM in our population over time despite the simpler and potentially more potent cART regimen of the later years. Factors that affect the prevalence of TDRM are not well described and require further evaluation, particularly given the relationship between TDRM and virologic outcomes and the limited number of antiretroviral classes that are currently available to treat HIV infection.
There are several limitations in our study. This was a retrospective, single site study. We did not distinguish between acute HIV infection and chronic HIV infection. Our results potentially underestimate the prevalence of “nonfit” drug-resistant mutations that will be difficult to detect after the wild-type strains predominate. Nevertheless, the goal of our study was to provide findings relevant to routine patient care and genotypic testing is most commonly done in patients presenting with established chronic HIV infection. Measurement of virologic outcome was HIV RNA suppression at 48 weeks, which did not take into account subsequent virologic failure. A previous study illustrated that short-term virologic failure within 24 weeks may not translate to differences in long-term clinical outcomes. 24 Therefore, longitudinal data should be collected for further analyses. Lastly, because this was a retrospective review of data we did not have formal measurements of cART adherence.
In summary, transmitted drug resistance mutations remain prevalent in our community, affecting one in six newly diagnosed, treatment-naive HIV-infected patients. The presence of TDRM negatively impacted virologic outcomes when cART was initiated, especially when NNRTI resistance mutations were present. Considering the significant effect of the TDRM, its prevalence should be monitored and intervention studies to lower the transmission of drug resistance should be further developed.
Footnotes
Acknowledgments
We thank the staff at the Washington University Institute of Clinical and Translational Sciences and the patients and staff at the Washington University HIV Outpatient Clinic. This work was supported by Washington University School of Medicine, Department of Medicine, Division of Infectious Diseases.
Author Disclosure Statement
E.T.O. reports that he has served as a consultant, on speakers bureau, or on an advisory board for the following companies: Gilead, Bristol Myers Squibb, Glaxo-Smith-Kline, Tibotec, Merck, Monogram Sciences and Boehringer Ingelheim. He also reports that he has received research support from the following companies: Abbott, Gilead, Bavarian Nordic, Glaxo-Smith-Kline, Boehringer Ingelheim, and Tibotec. All other authors: no competing financial interests exist.